
Translate this page into:
Current view of bone regeneration using mesenchymal stem cells
Address for correspondence: Dr. Omar A. Al-Mohrej, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, P.O. Box 22490, Riyadh 11426, Saudi Arabia. E-mail: mohrejo@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Al-Mohrej OA, Al-Ayedh NK, Al-Awlah AY, Al-Kenani NS. Current view of bone regeneration using mesenchymal stem cells. J Orthop Allied Sci 2016;4:1-4.
Abstract
Bone regeneration, reparative and restorative techniques of bone length discrepancies, correction of posttraumatic and congenital defects and deformities can be induced mesenchymal stem cells (MSCs) which is taken from the bone marrow. In this review article, we aimed to have a look at MSCs for bone and tissue regeneration. MEDLINE®, Embase™, the Science Citation Index, and Google™ Scholar were used to look for relevant articles which published in English since January 2000. Studies on bone regeneration using MSCs in the field of clinical orthopedics were retrieved. The bone graft can create a self-reliant mechanism to induce bone cellular environment that adapts to the whole skeletal nature. There are several factors contributory to deciding which approach to take. These include the type of bone deformities, defects, the biological setting of the patient, the nature of the reparative process desired, and surgical or orthopedic possibility of conducting all these processes. All these factors and several others should be taken into consideration and careful medical consultation. Orthopedics along with osteology made much headway in restoring bone and tissue in uniquely medical approach that is MSCs through the autologous cancellous bone taken from the bone marrow.
Keywords
Bone regeneration
mesenchymal stem cells
orthopedics

Introduction
Before the medical amazing discoveries in the last 100 years, surgery and orthopedics were almost unable to treat complicated nonunion, tumors, deformities, and bone defects. However, Ilizarov devised a bone transport process - osteotomy - to regenerate bone and tissue [Figure 1].[1,2] Yet, Ilizarov device of distraction osteogenesis has some complications.[3] Therefore, Ilizarov devised a bone graft process using mesenchymal stem cells (MSCs), which have osteoconductive properties that stimulate the new growth of bone and tissue formation.[4]
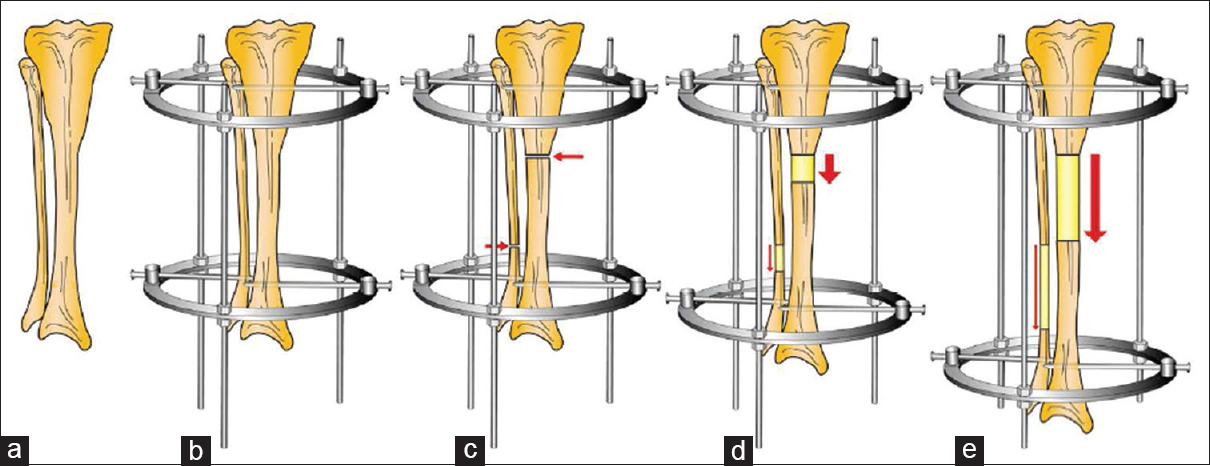
- The bone is encased by the Ilizarov device during the gradual phases in distraction osteogenesis. (a) The bone to be lengthened; (b) Ilizarov device application; (c) proximal tibia osteotomy; (d) beginning of the distraction and (e) end of distraction
MEDLINE®, Embase™, the Science Citation Index, and Google™ Scholar were used to look for relevant articles which published in English since January 2000. Studies on bone regeneration using MSCs in the field of clinical orthopedics were retrieved.
Development of Mesenchymal Stem Cells
MSCs are by definition "plastic-adherent cell population that can be directed to differentiate in vitro into cells of osteogenic, chondrogenic, adipogenic, myogenic, and other lineages."[5] MSCs are also stromal and embryonic connective, as well.[6] MSCs are self-renewed with a morphology of fibroblast-like.[7]
The history of MSCs dates back to about 1924 by Maximow[8] when he conducted a histological study showing how MSCs developed into blood cells. In 1960s, Till and McCulloch[9] discovered the cloning property of marrow cells - colonizing into cellular units. In several studies, MSCs were used by Friedenstein et al. in 1970s.[10,11,12] Later, MSCs were cultured and proved to be osteoinductive for tissue and bone formation as a reparative and restorative medical uses in orthopedics and surgery.[13] The efficacy of the cell-gene-based method through engineered MSCs to induce bone and tissue formation was evaluated by micro-computed tomography.[14]
Cultured MSCs are a good osteoinductive technique to generate bone formation in vivo. To generate bone connective tissue, it is important to seed MSCs on a ceramic scaffold.[15] Generally speaking, the number of MSCs in 60-year olds is fewer than those found in 20-year olds. MSCs make a good source of cell transplants for self-osteogenesis for the same patient - cellular regenerative method.[16]
The main source of MSCs is the bone marrow. Although MSCs are few, they can be cultivated through in vitro technique for medical uses.[17] The other secondary sources of MSCs can be the adipose tissue, peripheral blood, placenta, heart, muscles, skin, and umbilical cord [Figure 2].[18,19] It is not easy to identify MSCs because they have different physiology, morphology and endothelial and hemopoietic surface antigens are not in MSCs. In one word, MSCs are heterogeneous.[20] As MSCs have immunological properties, they can be used as allogenic transplant.[21]
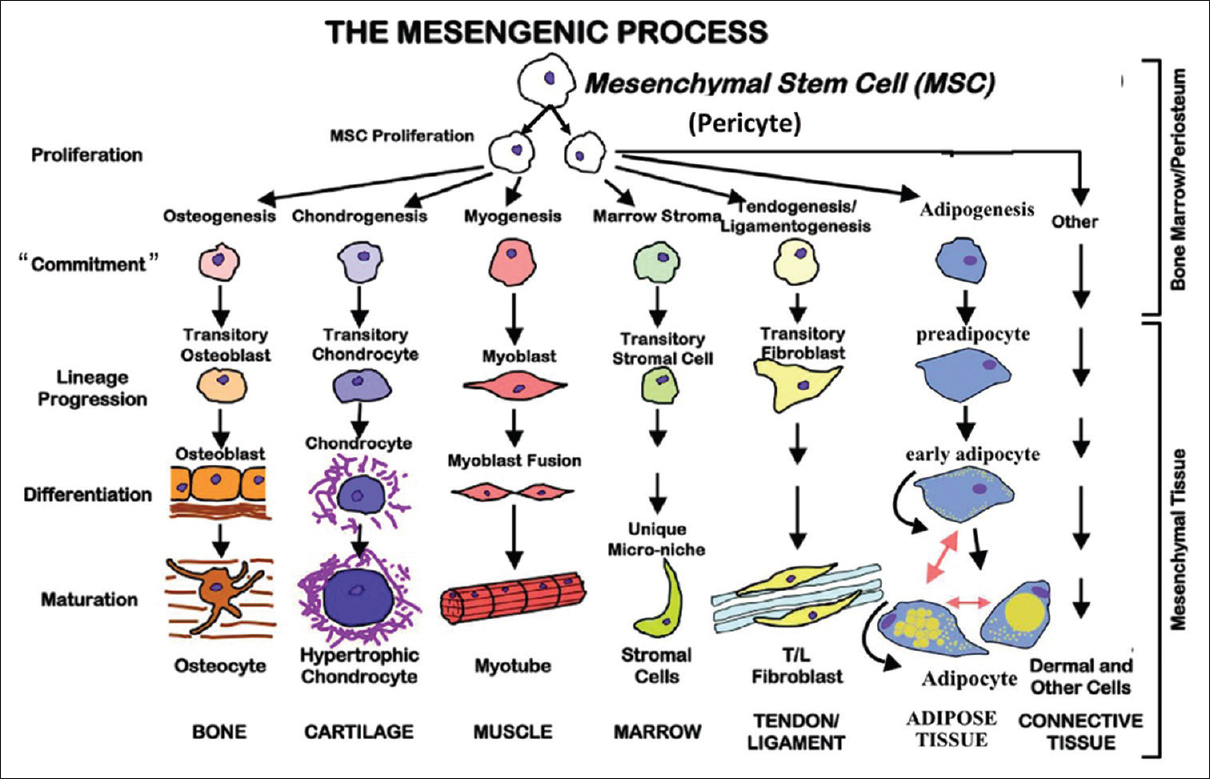
- The mesengenic process of mesenchymal stem cells showing purebred progression and maturation
Bone Regeneration and Mesenchymal Stem Cells
MSCs can be used for bone and tissue regeneration and engineering. In the formation of intramembranous bone, MSCs move to the bone formation. After MSCs condensate and align, MSCs produce an extracellular matrix known as the osteoid. Then the cells keep on proliferating. MSCs that differentiated into osteoblasts start to deposit calcium and then form a bone matrix.[22]
As it is stated, "it has been demonstrated that mesenchymal stem cells from the bone marrow from the iliac crest graft have great osteoinductive properties."[23] MSCs make up a reparative and restorative material for osteogenesis. MSCs opened up a new frontier for osteosynthesis that can treat bone defects and deformities and even make up lost parts of the human body.[24] In addition, MSCs can medically mediate the proliferation, angiogenesis, osteogenesis, and differentiation of cells. As an alternative way to correct bone defects and deformities through distraction osteogenesis, MSCs can regenerate bone and tissue formation through a transplant process- biologically constructed osteogenesis.[25]
The most successful material for bone grafting is the autologous cancellous that can be taken from the bone marrow.[26] The autologous cancellous bone has three unique properties; it is osteogenic, osteoinductive and nonimmunogenic. This means that infections and sepsis and other possible traumatic or cancerous elements are not factored in the process of using the autologous cancellous bone. MSCs can marvelously differentiate in cell lines where bone zone needs to be repaired and restored [Figure 3].[27,28]
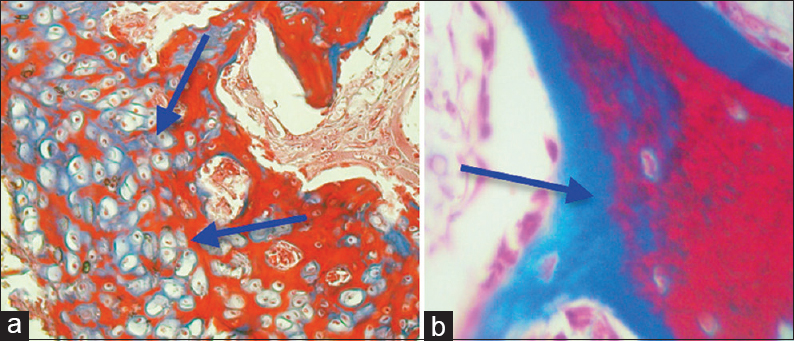
- Osteogenesis in good quality was induced through undifferentiated stem cells in a radius of dog. (a) Endochondral ossification. (b) Intramembranousossification
Limitations of Mesenchymal Stem Cells
One limitation of MSCs used in osteogenesis is that MSCs cannot induce osteogenesis where the zone of the bone defect is large; MSCs are enough to fill the zone to induce bone formation.[29] Alternatively, bone substitutes or bone grafts are a better medical solution to induce osteogenesis.[30] Another limitation of using autologous cancellous bone in correcting bone defects is rejection or failure to adapt to the process and the possible instability of the whole bone grafting process.[31]
However, MSCs may not be always medically advantageous and easy to manage; one limitation is the morbidity of procuring MSCs.[32] Another limitation is that MSCs produce a low number of stem cells.[33] Lack of precision in managing MSCs is another limitation.[34] Furthermore, procuring MSCs brings about the function loss of the donor's nerve graft site and a sort of mismatch of dimensions.[35]
Conclusion
Bone and tissue regeneration can be induced through different treatment modalities. There are several factors contributory to deciding which approach to take. These include the type of bone deformities, defects, the biological setting of the patient, the nature of the reparative process desired and surgical or orthopedic possibility of conducting all these processes. All these factors and several others should be taken into consideration and careful medical consultation.
MSCs can be taken from various body sites but most importantly is the bone marrow. Autologous cancellous bone is biologically osteogenic, osteoinductive and nonimmunogenic. These three biochemical properties make an ideal environment for bone and tissue formation.
Orthopedics along with osteology made much headway in restoring bone and tissue in uniquely medical approach that is MSCs through the autologous cancellous bone taken from the bone marrow. The method is still embryonic but is effective in restore bone and tissue defects where distraction osteogenesis cannot be applied.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Clinical application of the tension-stress effect for limb lengthening. Clin Orthop Relat Res. 1990;250:8-26.
- [CrossRef] [Google Scholar]
- Distraction osteogenesis and its challenges in bone regeneration. In: Tal H, ed. Bone Regeneration. Croatia : InTech; 2012. p. :185-212.
- [Google Scholar]
- Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res. 1990;250:81-104.
- [CrossRef] [Google Scholar]
- Effect of acute blood loss on stromal regulation of hematopoietic stem cells and reparative bone regeneration. Patol Fiziol Eksp Ter. 1986;5:54-8.
- [Google Scholar]
- 19-mesenchymal stem cells. In: Atala A, Lanza R, Thomson JA, Nerem RM, eds. Principles of Regenerative Medicine. San Diego: Academic Press; 2008. p. :318-43.
- [CrossRef] [Google Scholar]
- Stem cells: Units of development, units of regeneration, and units in evolution. Cell. 2000;100:157-68.
- [Google Scholar]
- Multilineage potential of adult human mesenchymal stem cells. Science. 1999;284:143-7.
- [CrossRef] [PubMed] [Google Scholar]
- Relation of Blood Cells to Connective Tissues and Endothelium. Physiological Revue. 1924;4:533-63.
- [CrossRef] [Google Scholar]
- A direct measurement of the radiation sensitivity of normal mouse bone marrow cells. Radiat Res. 1961;14:213-22.
- [CrossRef] [PubMed] [Google Scholar]
- Precursor cells of mechanocytes. Int Rev Cytol. 1976;47:327-59.
- [CrossRef] [PubMed] [Google Scholar]
- The development of fibroblast colonies in monolayer cultures of Guinea-pig bone marrow and spleen cells. Cell Tissue Kinet. 1970;3:393-403.
- [CrossRef] [PubMed] [Google Scholar]
- Stromal cells responsible for transferring the microenvironment of the hemopoietic tissues. Cloning in vitro and retransplantation in vivo. Transplantation. 1974;17:331-40.
- [CrossRef] [PubMed] [Google Scholar]
- Osteoinductive biomaterials - Properties and relevance in bone repair. J Tissue Eng Regen Med. 2007;1:25-32.
- [CrossRef] [PubMed] [Google Scholar]
- Tissue Engineering: Roles, Materials, and Applications. (1st). New York: Nova Science Publishers; 2008.
- [Google Scholar]
- Biological scaffolds for regenerative medicine. In: Atala A, Lanza R, Thomson JA, Nerem RM , eds. Principles of Regenerative Medicine (2nd). San Diego: Academic Press; 2011. p. :623-35. Ch. 34
- [CrossRef] [Google Scholar]
- In vitro cultivation of islet-like cell clusters from human umbilical cord blood-derived mesenchymal stem cells. Transl Res. 2008;151:293-302.
- [CrossRef] [PubMed] [Google Scholar]
- Different populations and sources of human mesenchymal stem cells (MSC): A comparison of adult and neonatal tissue-derived MSC. Cell Commun Signal. 2011;9:12..
- [CrossRef] [PubMed] [Google Scholar]
- Mesenchymal stem cells in tissue repair. Front Immunol. 2013;4:201..
- [CrossRef] [PubMed] [Google Scholar]
- Functional heterogeneity of mesenchymal stem cells: Implications for cell therapy. J Cell Biochem. 2012;113:2806-12.
- [CrossRef] [PubMed] [Google Scholar]
- The immune properties of mesenchymal stem cells. Int J Biomed Sci. 2007;3:76-80.
- [CrossRef] [PubMed] [Google Scholar]
- Functional Bone Tissue Engineering Using Human Mesenchymal Stem Cells and Polymeric Scaffolds. North Carolina: North Carolina State University ; 2006. p. :271.
- [Google Scholar]
- Fundamentals of Tissue Engineering and Regenerative Medicine. Berlin: Springer; 2009. p. :1049.
- [CrossRef] [Google Scholar]
- Mesenchymal stem cells for bone, cartilage, tendon and skeletal muscle repair. Bone. 2006;39:678-83.
- [CrossRef] [PubMed] [Google Scholar]
- Bone-grafting and bone-graft substitutes. J Bone Joint Surg Am 2002:454-64.:84-64.
- [CrossRef] [PubMed] [Google Scholar]
- Tissue engineering strategies for bone regeneration. Adv Biochem Eng Biotechnol. 2005;94:1-22.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of autologous stem cells on regenerated bone during distraction osteogenesis by Ilizarov technique in the radius of dogs. Histomorphometric analysis. Acta Cir Bras. 2013;28:574-81.
- [CrossRef] [PubMed] [Google Scholar]
- Osteogenicity of biphasic calcium phosphate ceramics and bone autograft in a goat model. Biomaterials. 2008;29:1177-88.
- [CrossRef] [PubMed] [Google Scholar]
- Stem cells associated with macroporous bioceramics for long bone repair: 6- to 7-year outcome of a pilot clinical study. Tissue Eng. 2007;13:947-55.
- [CrossRef] [PubMed] [Google Scholar]
- The biology of bone graft repair. Clin Orthop Relat Res. 1983;174:28-42.
- [CrossRef] [Google Scholar]
- Comparison of anterior and posterior iliac crest bone grafts in terms of harvest-site morbidity and functional outcomes. J Bone Joint Surg Am 2002:716-20.:84-20.
- [CrossRef] [PubMed] [Google Scholar]
- The use of mesenchymal stem cells in orthopedics. In: Stem Cells and Cancer Stem Cells. Vol 1. Netherlands: Springer; 2012. p. :173-9.
- [CrossRef] [Google Scholar]
- Mesenchymal stem cells suppress lymphocyte proliferation in vitro and prolong skin graft survival in vivo. Exp Hematol. 2002;30:42-8.
- [CrossRef] [PubMed] [Google Scholar]
- Micro and Nanotechnologies in Engineering Stem Cells and Tissues. New Jersey: Wiley; 2013.
- [Google Scholar]




