
Translate this page into:
Correlation of clinical, MRI and arthroscopic findings in diagnosing meniscus and ligament injuries at knee joint: A prospective study
Address for correspondence: Dr. Kamini Gupta, Department of Radiodiagnosis, Dayanand Medical College and Hospital, Ludhiana, India. E-mail: kaminikshitij@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gupta K, Guleria M, Sandhu P, Galhotra R. Correlation of clinical, MRI and arthroscopic findings in diagnosing meniscus and ligament injuries at knee joint: A prospective study. J Orthop Allied Sci 2013;1:2-6.
Abstract
Objective:
The purpose of this study was to correlate clinical, MRI, and arthroscopic findings in diagnosing ligament and meniscus tears in knee joint injuries.
Materials and Methods:
Our study included 20 patients in the age range of 11-60 years who were referred to radiology department for MRI of knee joint following injury to the knee. Prior to MRI, a detailed history, clinical, and local examination was done in all the subjects. MRI was carried out on 1.5 Tesla MR Machine and the standard protocol consisted of fat-suppressed PD (TE 45, TR 2800) in axial, sagittal, and coronal planes, T2W (TE 80, TR 4000) in sagittal plane and T1W (TE 11, TR 495) in sagittal plane. All the patients underwent arthroscopy by an orthopedic surgeon.
Results:
MR had 100% sensitivity and NPV of diagnosing ACL tears in this study. Clinical examination had sensitivity of 88% and NPV 75% in diagnosing ACL injuries. There was high NPV of MR examination (96%) in diagnosing meniscus tear while the PPV of MR examination was low (71%). These values were low in case of clinical examination.
Conclusions:
MRI is a useful non-invasive modality having high diagnostic accuracy, sensitivity, and negative predictive value making it a very reliable screening test for diagnosing internal derangements.
Keywords
Arthroscopy
cruciate ligament
magnetic resonance imaging
meniscus

Introduction
Knee injuries represent roughly 6% of all acute injuries treated at emergency department and between 27% and 48% of these have been reported to be sports related.[1]
History taking regarding mechanism of knee injury gives a vital clue to the internal derangements of knee joint. Hyperextension with an audible pop suggests a likely diagnosis of anterior cruciate ligament (ACL) tear. Direct blow to the knee if sideways would point toward collateral ligament injury and if in the front would indicate cruciate ligament injury. Although clinical examination is most important for the diagnosis of ligament injury, painful stress examinations are not always accurate in the acute phase of the injury. For that reason, magnetic resonance imaging (MRI) is indicated for early diagnosis of the acutely injured knee.[2]
While the use of arthrography and arthroscopy improves the accuracy of the diagnosis, both are invasive and can cause complications. Diagnostic arthroscopy is an important advance, improving diagnostic accuracy to 64-94%. However, it is an operative procedure, with the possible complications of infection, hemarthrosis, adhesions, neurological problems, reflex sympathetic dystrophy, and broken instruments, as well as complications related to anesthesia. Selective MRI is a completely non-invasive diagnostic modality and there is no ionizing radiation.[3]
Moreover the ligaments of knee are divided into intra-articular and extra-articular, consequently MRI plays a most important role in their evaluation. This division is important as the extra-articular ligaments are not visible on routine arthroscopic procedures.[4]
Purpose
This prospective study aimed to compare and correlate the clinical, MRI, and arthroscopic findings in the diagnosis of various ligament and meniscus tears in knee joint injuries.
Materials and Methods
The ethics committee of our institute approved this prospective study. Informed consent was taken from all patients undergoing this study. We prospectively studied 20 patients in the age range of 11-60 years over a period of 18 months starting from January 2008. All patients of knee injury who underwent MR imaging were included in the study. Patients excluded from the study were those:-
With contraindications to MR
Prior arthroscopy or surgical intervention
Known joint disease like neoplasm, inflammatory or infectious disorder
History of old significant trauma to the currently injured knee.
Findings of specific local examination of injured knee were recorded in detail and a clinical diagnosis was established in all the cases. Screening X-rays were documented for evidence of bony injury. MR examination was done on all the patients and findings were documented as per proforma. [Table 1]. All the patients underwent athroscopy at our institute and findings were recorded.

MRI technique
MR scan in all the patients included in this study was carried out on MAGNETOM Avanto 18 Channel 1.5 Tesla MR Machine by Siemens India Ltd.
Patient positioning
Patient was positioned supine and feet-first in the MR imager, with the knee to be imaged in approximately 100-150 degree external rotation to aid the imaging of the ACL in the sagittal plane. Studies were performed with a 5'/2-inch flat surface coil placed posterior to the knee of interest. The knee to be imaged was centered within the 16-cm field of view, including in the image both the suprapatellar bursa and the insertion of the patellar ligament on the tibial tubercle.
MRI protocol
Localizer was taken in axial, sagittal, and coronal planes after making proper positioning of the patient. The MRI protocol consisted of fat-suppressed PD (TE 45, TR 2800) in axial, sagittal, and coronal planes, T2W (TE 80, TR 4000) in sagittal plane and T1W (TE 11, TR 495) in sagittal plane. A 170-mm field of view and a 256 × 192 matrix with one signal average was used. The slice thickness was 4 mm.
The images were interpreted by two qualified radiologists individually who had experience of about 10 years in this field. All clinical and MR Imaging findings were recorded as per proforma. All the patients underwent arthroscopy by a qualified and experienced orthopedic surgeon. Surgeon was aware of MRI findings in all the cases prior to arthroscopy. Subsequently analysis for comparison between clinical, MRI, and arthroscopic findings was undertaken.
Results
Specific history and relevant clinical examination of injured knee was done in all 20 patients and a clinical diagnosis was established. All of them underwent a dedicated MR knee examination as per the protocol. Considering arthroscopy as gold standard, MR and clinical findings were compared with arthroscopic findings.
In our study, in case of meniscus tears, MR had sensitivity of 91% and NPV of 96%. These values were low in case of clinical examination, 66% and 86%, respectively.
There was not much difference in specificity and positive predictive value (PPV) of MR and clinical examination in case of meniscus tears.
Sensitivity and NPV of MR examination were very high in diagnosing ACL tears. MR had 100% sensitivity and NPV of diagnosing ACL tears in this study. Clinical examination had sensitivity of 88% and NPV of 75% in diagnosing ACL injuries. Specificity and PPV were relatively low for MR as compared to clinical examination in diagnosing ACL tears. MR had specificity of 50% and PPV of 89% while clinical examination had specificity and PPV of 100%.
Diagnostic accuracy was 90% in diagnosing ACL tears for both clinical and MR examination while MR had marginally higher diagnostic accuracy in case of meniscus tears [Tables 2 and 3].


The criterion to diagnose meniscus tear was hyperintense signal extending to the articular surface (Grade III signal) on PD and STIR seq [Figure 1].

- Linear intrasubstance high signal intensity is seen in the body of medial meniscus on STIR images (white arrow). The signal is extending till the inferior articular surface-meniscus tear.
Other findings in our study were a full-thickness longitudinal tear leading to the development of bucket handle tear. In a bucket handle tear, the inner fragment becomes displaced either centrally giving "fragment in notch" sign [Figure 2] or "double PCL" sign [Figure 3] or anteriorly giving "large anterior horn" or "Flipped Fragment" sign [Figure 4], Partial tear of PCL leading to its buckling [Figure 5], Complete tear of ACL seen as disruption of fibers with hyperintense signal [Figure 6].

- Coronal STIR sequence: Fragment in notch sign (arrow) in bucket handle tear

- Sagittal PD sequence: Double PCL Sign (arrow) in bucket handle tear
- Sagittal PD sequence: Flipped fragment sign in bucket handle tear

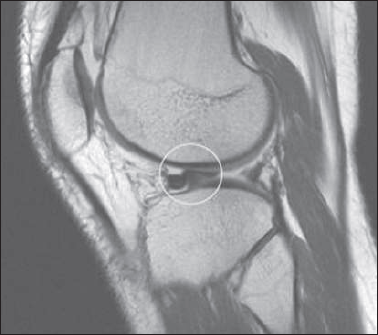
- Sagittal STIR sequence: Osteochondral fracture along the posterior tibial plateau at the site of insertion of PCL (white circle). Also there is acute angulation and buckling (arrow) of PCL in its upper part - partial tear

- Sagittal PD sequence: There is disruption of ACL from its tibial attachment (black circle) with intermediate signal in the ligament (white arrow)
Discussion
The single most common indication of performing a knee MRI is to diagnose internal derangements in an injured knee.
Clinical examination may be difficult in acute injury and is inconclusive in cases with injuries of multiple ligaments/menisci.
MRI being non-invasive and a highly sensitive tool of investigation, early and subtle changes in the soft tissues often are picked up by MRI. Arthroscopy, being highly sensitive and specific procedure is both diagnostic and therapeutic. But it is invasive and has complications associated with it, thus limiting its use as a diagnostic modality alone.
In this prospective study of 20 subjects, we compared the findings of MR and clinical examination with the arthroscopic findings. We calculated sensitivity, specificity, PPV, NPV, and accuracy of clinical and MR examination in diagnosing ligament and meniscus tears presuming arthroscopy to be gold standard.
In case of ACL tears diagnostic accuracy for both clinical and MR examination came out to be 90% but MR was more sensitive than clinical examination. Sensitivity for diagnosing ACL tear by MR was 100% while it was 88% for clinical examination. NPV of MR examination was 100% making it a very good screening test. Thus, when we interpreted ACL as normal on MR scan, it was normal all the times on arthroscopy. PPV of MR examination was 89%. There were two false positive examinations by MR. These were two subjects with partial ACL tears which were not picked on arthroscopy. Dowdy et al.[5] documented that a positive MRI for an ACL tear combined with a normal arthroscopy did not necessarily represent a false positive MRI and that an intrasubstance tear may be present which is difficult to detect with arthroscopy.
Specificity of MR for diagnosing ACL tears was low to the tune of 50% in our study. Low specificity was due to low percentage (10%) of negative MRI results. Specificity of clinical examination was quite high virtually reaching 100% mark. There was not even a single false positive clinical examination. Thus, whenever there was a clinical suspicion of ACL tear on account of various clinical tests like Lachmann test or anterior drawer test, there was a corresponding tear on arthroscopy.
Overall in case of ACL tears we suggest MR has the advantage in those subjects where clinical tests are equivocal and we do not want to unnecessarily subject the patient to an invasive procedure in diagnostic arthroscopy. MR confirms the clinical diagnosis and the patient can be taken up for therapeutic arthroscopy.
Barronian et al.[6] in their study of 22 patients showed results similar to ours. They calculated PPV and NPV of MR examination and concluded that the NPV was 92% for cruciate ligaments, whereas the PPV was 50%. (i.e., a negative MRI was more accurate). The high NPV is important and indicates that a negative MRI is quite reliable for cruciate ligaments.
Diagnostic accuracy of MRI was 88% for menisci (80% for MM and 95% for LM) in our study which corresponds to studies done by Glashow et al.[7] Kinnunen et al.[8] İncesu et al.[9]
Diagnostic accuracy of clinical examination (83%) was relatively low as compared to MR examination (88%) in our study. These results regarding diagnostic accuracy have also been shown in previous studies. The accuracy of the clinical diagnosis of meniscus tears is about 75-80%[10,11] compared with 88-90% for MRI.[12]
There was high NPV of MR examination (96%) in diagnosing meniscus tear as was in the case of ACL while the PPV of MR examination was low (71%). In the study by Barronian et al. the NPV was 91% for menisci, whereas the PPV was 65%. Thus it is evident again that MRI's NPV makes it the investigation of choice.
There were four false positive MR examinations in our study accounting for low PPV of MR examination. Out of these four false positive examinations, site of the three tears were located predominantly in the posterior and one was in the anterior horn. Posterior horn tears of menisci are likely to be missed on arthroscopy especially if anterior approach is used and if the menisci are not probed. Inferior surface of the meniscus is in particular vulnerable to this flaw in arthroscopy. Thus acceptance of MRI findings as false positive is controversial. It is suggested that the reason of false positive and false negative meniscal lesion diagnosis was related to diagnostic errors in MRI as well as faults in arthroscopic evaluation. Levinsohn et al.[13] MRI seems to over-diagnose tears of the menisci resulting in a low PPV.
Mink et al.[14] reported (in a series of five studies) a total of 47 false-positive results with MRI, 70% of which were in the posterior horn. This may occur because the lesion is missed at arthroscopy as there is difficulty in visualizing the posterior compartments similar to that encountered in the false positive cases in our study. Meniscal degeneration has also been suggested to explain over-diagnosis because of the increased signal intensity.
So in our prospective study we have found out that sensitivity and NPV of MR examination for diagnosing ACL and meniscus tears are quite high.
So, one can rely on MRI to avoid diagnostic arthroscopy as MRI has a high sensitivity and low false-negative rate.
Thus we conclude that MRI is a useful non-invasive modality having high diagnostic accuracy, sensitivity and negative predictive value making it a very reliable screening test for diagnosing internal derangements at knee joint. MRI is advantageous in conditions where arthroscopy is not useful like peripheral meniscus tears and inferior surface tears.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Acute rotational trauma to the knee: Poor agreement between clinical assessment and magnetic resonance imaging findings. Scand J Med Sci Sports. 2007;17:109-14.
- [CrossRef] [PubMed] [Google Scholar]
- Proper use of MR imaging in internal derangement of the knee (orthopedic surgeon's view) Semin Musculoskelet Radiol. 2001;5:143-5.
- [CrossRef] [PubMed] [Google Scholar]
- The accuracy of selective magnetic resonance imaging compared with the findings of arthroscopy of the knee. J Bone Joint Surg Am. 1988;70:192-8.
- [CrossRef] [Google Scholar]
- Knee: Ligaments. Imaging of Orthopedic Sports Injuries Springer 2007:284-303.
- [CrossRef] [Google Scholar]
- Magnetic resonance imaging of the partially torn anterior cruciate ligament: an in vitro animal model with correlative histopathology. Clin J Sport Med. 1994;4:187-91.
- [CrossRef] [Google Scholar]
- Magnetic resonance imaging of the knee: correlation with arthroscopy. Arthroscopy. 1989;5:187-91.
- [CrossRef] [PubMed] [Google Scholar]
- Double-blind assessment of the value of magnetic resonance imaging in the diagnosis of anterior cruciate and meniscal lesions. J Bone Joint Surg Am. 1989;71:113-9.
- [CrossRef] [Google Scholar]
- Diagnostic performance of low field MRI in acute knee injuries. Magn Reson Imaging. 1994;12:1155-60.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of magnetic resonance imaging (MRI) and arthroscopic findings in knee joint pathologies. Turk J Med Res. 1997;15:21-5.
- [Google Scholar]
- A comparison of accuracy between clinical examination and magnetic resonance imaging in the diagnosis of meniscal and anterior cruciate ligament tears. Arthroscopy. 1996;12:398-405.
- [CrossRef] [PubMed] [Google Scholar]
- A prospective study comparing the accuracy of the clinical diagnosis of meniscus tear with magnetic resonance imaging and its effect on clinical outcome. Arthroscopy. 1996;12:406-13.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging of the knee: diagnostic performance studies. Clin Radiol. 1996;51:251-7.
- [CrossRef] [PubMed] [Google Scholar]
- Prearthrotomy diagnostic evaluation of the knee: review of 100 cases diagnosed by arthrography and arthroscopy. AJR Am J Roentgenol. 1980;134:107-11.
- [CrossRef] [PubMed] [Google Scholar]
- Tears of the anterior cruciate ligament and menisci of the knee: MR imaging evaluation. Radiology. 1988;167:769-74.
- [CrossRef] [PubMed] [Google Scholar]




