
Translate this page into:
Corona mortis—A south Indian cadaveric study
Address for correspondence: Prof. Vetrivel Chezian Sengodan, Institute of Orthopaedics and Traumatology, Coimbatore Medical College Hospital, The Tamil Nadu Dr. MGR Medical University, Coimbatore, Tamil Nadu, India. E-mail: svcortho@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Sengodan VC, Sivagnanam M, Selvaraj R, Rathinasamy S. Corona mortis-A south Indian cadaveric study. J Orthop Spine 2022;10:30-4.
Abstract
BACKGROUND:
“Corona mortis” is an abnormal arterial or venous connection between the obturator and the inferior epigastric or external iliac arteries or veins, which can cause torrential bleeding leading to the death of the individual. It may be encountered during acetabular surgeries, hernia surgeries, and gynecological procedures. The purpose of our study is to determine the incidence and variations of corona mortis in the south Indian population.
MATERIALS AND METHODS:
Forty hemipelves of 20 cadavers were in our study group. With the cadaver in the supine position, dissection was done using Stoppa’s approach. After dissection, data about the presence or absence of corona mortis, the nature of corona mortis (arterial/venous/arteriovenous variant), and the distance between corona mortis and pubic symphysis were collected.
RESULTS:
Corona mortis was present in 33 (82.5%) hemipelves. It was bilateral in 13 (65%) cadavers. It was present in all the female cadavers on both sides, whereas it was present in 21 (75%) out of the 28 male hemipelves. Venous variant was present in 26 (78.78%), followed by arteriovenous variant in five (15.16%), and arterial variant in two (6.06%) hemipelves. The mean distance of corona mortis from pubic symphysis was 55.65 mm.
CONCLUSIONS:
The incidence of corona mortis was 82.5% in our study. Our study was dominated by the venous variant compared with the arterial and arteriovenous variants. Corona mortis had gender variations: it was present in all the females in our study, whereas it was not so among males as per our study.
Keywords
Cadaveric study
corona mortis
south Indian population

Introduction
“Corona mortis” is an abnormal arterial or venous connection between the obturator and the inferior epigastric or external iliac arteries or veins.[1] The term corona mortis means “crown of death,” because the damage to this vessel can cause torrential bleeding, which may lead to the death of the individual.[2] The corona mortis may be encountered during acetabular surgeries, hernia surgeries, and gynecological procedures. Hence it is very important for surgeons to have a clear knowledge about corona mortis.[2] The purpose of our study is to determine the incidence and variations of corona mortis in the south Indian population.
Materials and Methods
The study was performed between January 2020 and March 2021 after obtaining the institutional ethical committee approval. We included 40 hemipelves of 20 cadavers in our study group. Among the 20 cadavers, 14 (28 hemipelves) were male, and six (12 hemipelves) were female. Nondecomposed fresh adult cadavers were included in our study. Pediatric cadavers and mutilated or decomposed cadavers were excluded.
Both hemipelves of all the cadavers were dissected. With the cadaver in the supine position, dissection was done using Stoppa’s approach. A Pfannenstiel incision was made just above the pubic symphysis [Figure 1]. Subcutaneous tissue was divided in line with the skin incision to expose the rectus fascia [Figure 2]. The rectus fascia was incised longitudinally along the linea alba to expose the rectus muscles [Figure 3]. Both bellies of the rectus abdominis muscle were retracted laterally [Figure 4]. The medial part of the rectus muscle was partly detached from the upper part of the symphysis on the side of dissection to allow the rectus to retract for better exposure [Figure 5]. The upper border of the superior pubic ramus was identified, and blunt dissection was carried laterally along the pelvic brim to expose the corona mortis vessel [Figure 6]. After dissection, data about the presence or absence of corona mortis vessel, the nature of corona mortis (arterial/venous/arteriovenous variant) [Figure 7], and the distance between the corona mortis and the pubic symphysis using a digital vernier caliper with marker pins placed over the symphysis pubis and the site of corona mortis were collected [Figure 8].

- Pfannenstiel incision made just above the pubic symphysis

- Subcutaneous tissue divided in line with the skin incision to expose the rectus fascia
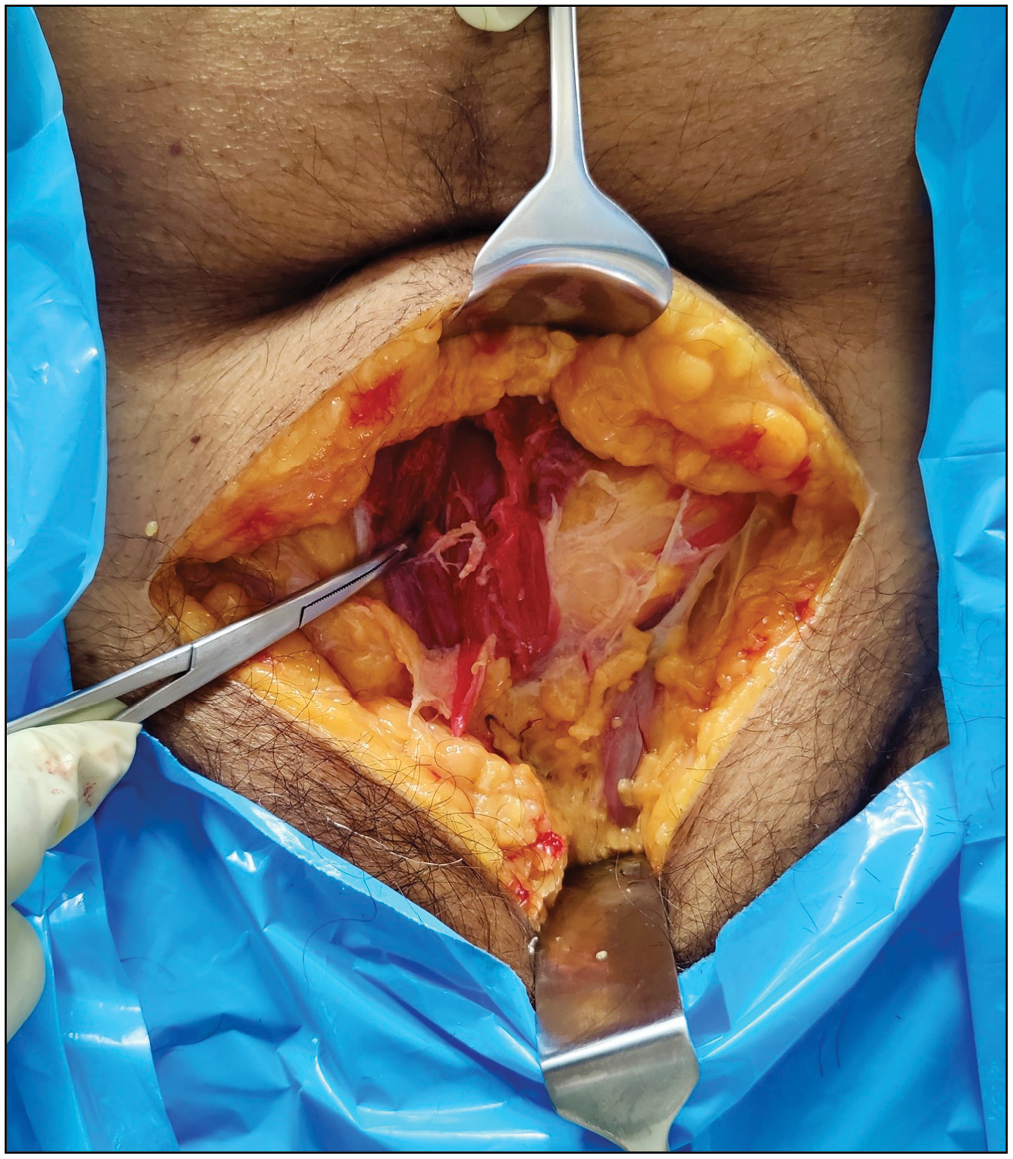
- Rectus fascia incised longitudinally along the linea alba to expose the rectus muscles

- Both bellies of the rectus abdominis muscle retracted laterally
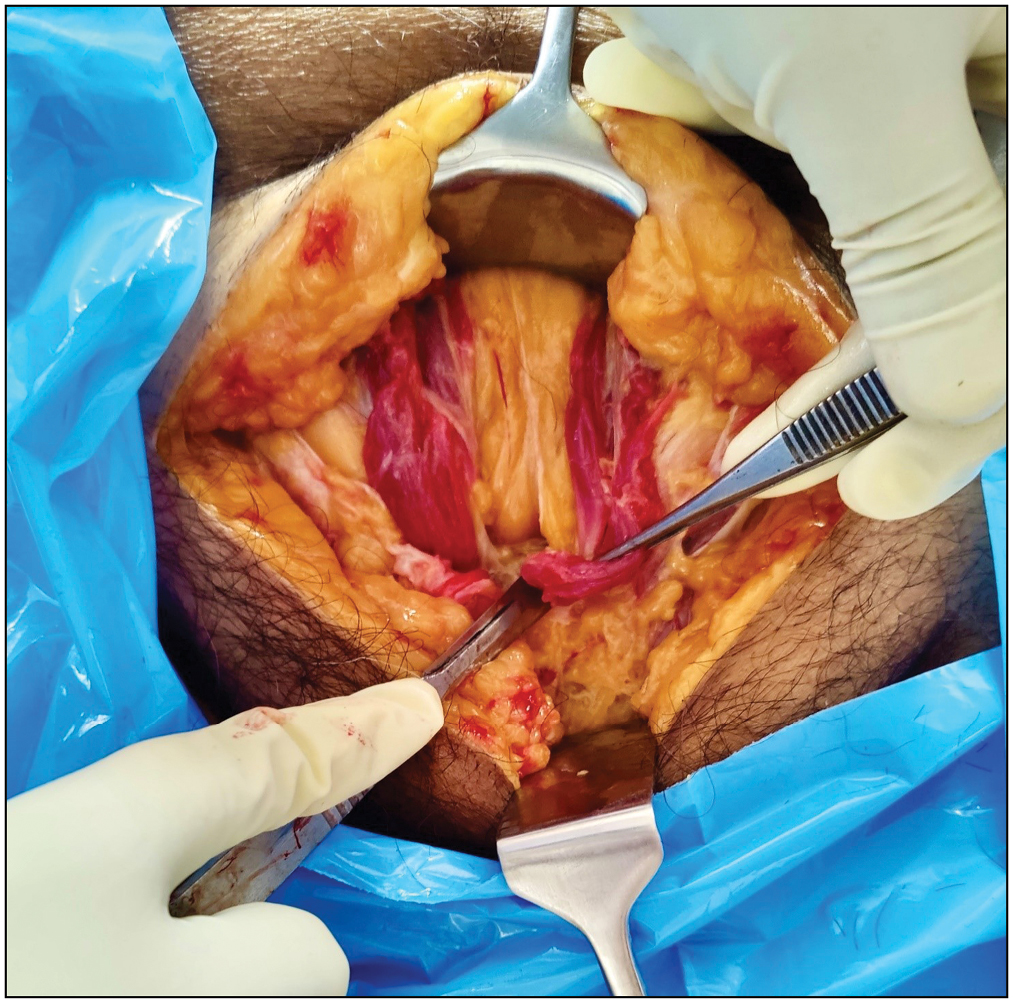
- Medial part of the rectus muscle partly detached from the upper part of the symphysis on the side of dissection to allow the rectus to retract for a better exposure
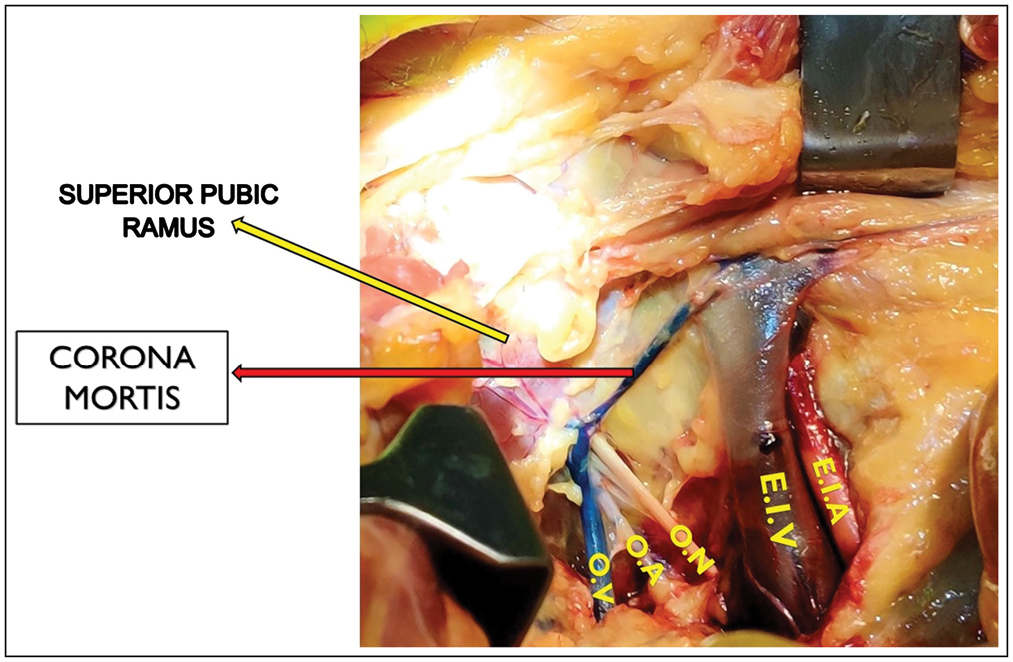
- Presence of corona mortis vessel (venous variant) connecting the external iliac vein and obturator vein
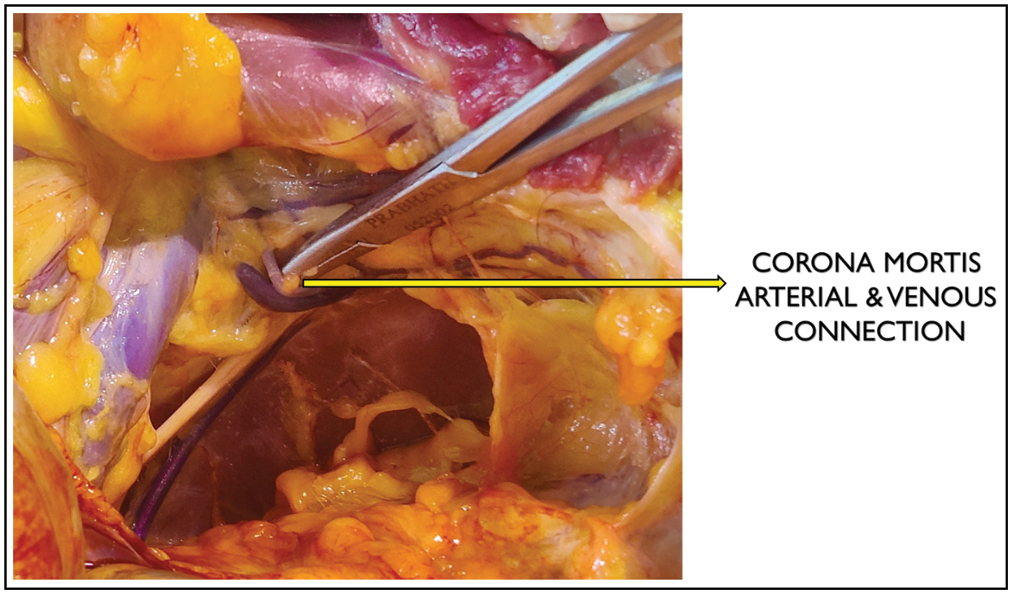
- Corona mortis with both arterial and venous variants
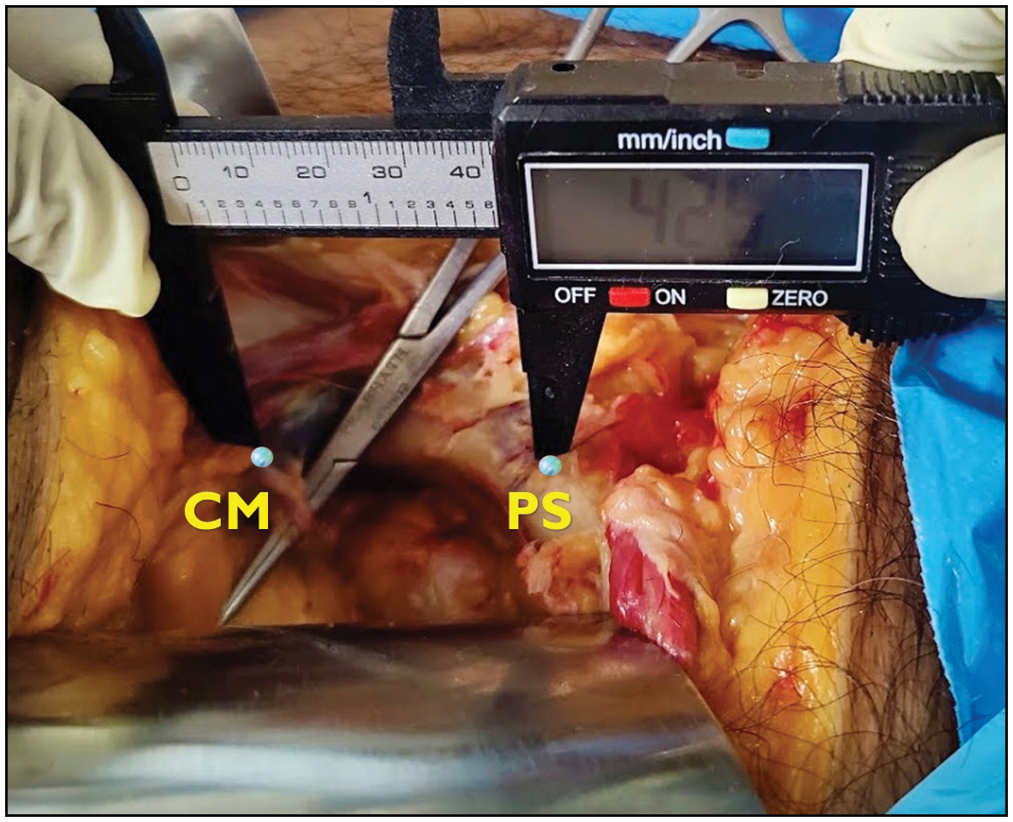
- Distance between the corona mortis and pubic symphysis is measured using a digital vernier caliper with marker pins placed over the symphysis pubis and the site of corona mortis
Results
Among the 40 hemipelves included in our study, corona mortis was present in 33 (82.5%) hemipelves and absent in seven (17.5%) hemipelves.
Regarding the side distribution, it was bilateral in 13 (65%) cadavers. Among the unilateral cases, as per our study, corona mortis was present on the right side in three (15%) cadavers and on the left side in four (20%) cadavers [Table 1].
| No. of cadavers | Corona mortis present | Corona mortis present in both hemipelves | Corona mortis present on the right side only | Corona mortis present on the left side only |
|---|---|---|---|---|
| 20 cadavers (40 hemipelves) | 33 (82.5%) hemipelves | 13 (65%) cadavers | Three (15%) cadavers | Four (20%) cadavers |
As per our study, corona mortis was present in all the female cadavers on both sides, whereas it was present in 21 (75%) out of the 28 male hemipelves [Table 2]. These values were analyzed with the chi-squared test and were found to be statistically insignificant (P > 0.05).
| Gender | No. of hemipelves | Corona mortis present | Corona mortis absent |
|---|---|---|---|
| Male | 28 | 21 (75%) | 7 (25%) |
| Female | 12 | 12 (100%) | Nil |
Regarding the anatomy of the corona mortis, the venous variant was present in 26 (78.78%) of the 33 hemipelves, which had corona mortis, followed by the arteriovenous variant in five (15.16%) hemipelves and arterial variant in two (6.06%) hemipelves [Table 3].
| Corona mortis present (total hemipelves) | Venous connection | Arterial connection | Both arterial and venous connection |
|---|---|---|---|
| 33 | 26 (78.78%) | 2 (6.06%) | 5 (15.16%) |
Regarding the distance of the corona mortis from the pubic symphysis, the maximum distance was 90 mm, the minimum distance was 40 mm, and the mean distance was 55.65 mm.
The mean distance of the corona mortis from the pubic symphysis in males was 59.09 mm, and in females, it was 60 mm. As per our study, the mean distance of the corona mortis from the pubic symphysis is more among females compared with males.
The mean distance of the corona mortis from the pubic symphysis on the right side was 60 mm, whereas it was 51.30 mm on the left side [Table 4].
| Gender | Mean (mm) | Right (mm) | Left (mm) |
|---|---|---|---|
| Male and female | 55.65 | 60 | 51.3 |
| Male | 59.09 | 60 | 58.18 |
| Female | 60 | 61.67 | 58.33 |
These values were analyzed with paired sample t-test and were found to be statistically insignificant (P > 0.05).
Discussion
Corona mortis is an anatomical variant between the obturator and the inferior epigastric or the external iliac arteries or veins.[1] Thus, it is a communication between the internal iliac and the external iliac vascular systems.[2]
According to the literature, it is present on the posterior aspect of the superior pubic ramus at a variable distance from the pubic symphysis.[1] In corona mortis, the venous connection is more common than arterial connection, and the presence of both arterial and venous connections has been documented in 20% of the specimens.[1]
In 2004, Okcu et al. in Turkey reported the incidence of corona mortis to be 61%. As per the study, the venous variant was the predominant type (85.71%) followed by the arterial variant (14.29%).[3]
In 2004, Hong et al. in China reported that the incidence of corona mortis was 72%. They reported the mean distance of the corona mortis vessel from the pubic symphysis was 52 mm.[4]
In 2016, Nayak et al. in Karnataka, India, reported a 51% incidence of corona mortis. According to the study, the arterial variant was the most predominant type (83.79%) followed by the venous variant (16.21%).[5]
In 2017, Pillay et al. in Kerala, India, reported the incidence of corona mortis to be 77%. The venous variant was the most predominant (54.07%), followed by the arteriovenous variant (37.83%) and the arterial variant being the least predominant type (8.10%).[6]
In 2018, Kashyap et al. in Shimla, India, reported 58.3% incidence of corona mortis. According to his study, the bilateral presence of corona mortis was seen in 41.7% of the cadavers, followed by the left-sided presence in 37.5% and the right-sided presence in 20.8% of the cadavers. As per their study, the venous variant was the most predominant type (85.72%) followed by the arterial variant (14.28%). The mean distance of the corona mortis vessel from the pubic symphysis was 41 mm.[7]
In 2021, Abbas et al. in Sudan reported a 43% incidence of corona mortis. As per their study, the arteriovenous variant was the predominant type (61.5%), followed by the arterial variant (30.8%), and the venous variant was the least predomina nt type (7.7%).[8]
We compared our study with similar studies done in other parts of the world [Table 5]. As per our study, the incidence of corona mortis was 82.5%, which is significantly higher than other studies in the world.
| Sample size (hemipelvis) | CM present (%) | Bilateral presence (%) | Right (%) | Left (%) | Venous (%) | Arterial (%) | Venous and arterial (%) | Mean distance (PS to CM) (mm) | |
|---|---|---|---|---|---|---|---|---|---|
| Okcu et al. (Turkey, 2004)[3] | 150 | 61 | - | - | - | 85.71 | 14.29 | Nil | - |
| Hong et al. (China, 2004)[4] | 50 | 72 | - | - | - | - | - | - | 52 |
| Abbas et al. (Sudan, 2021)[8] | 30 | 43 | - | - | - | 7.7 | 30.8 | 61.5 | - |
| Our south Indian study | 40 | 82.5 | 65 | 15 | 20 | 78.78 | 6.06 | 15.16 | 55.65 |
CM = corona mortis, PS = pubic symphysis
In our study, venous variant was more predominant (78.78%), which is similar to the study in Turkey where the venous variant was more predominant (85.71%).[3]
In our study, the mean distance of the corona mortis from the pubic symphysis was 55.65 mm, whereas it was 52 mm in the study done in China.[4]
We also compared our study with similar studies done in India [Table 6]. In our study, the incidence of corona mortis was 82.5%, whereas it was 77.08% in the study done in Kerala,[6] followed by 58.3% in the study from Shimla[7] and 51% in the study from Karnataka.[5]
| Sample size (hemipelvis) | CM present (%) | Bilateral presence (%) | Right (%) | Left (%) | Venous (%) | Arterial (%) | Venous & arterial (%) | Mean distance (PS to CM) (mm) | |
|---|---|---|---|---|---|---|---|---|---|
| Nayak et al. (Karnataka, India 2016)[5] | 73 | 51 | - | - | - | 16.21 | 83.79 | Nil | - |
| Pillay et al. (Kerala, India, 2017)[6] | 48 | 77.08 | - | - | - | 54.07 | 8.10 | 37.83 | - |
| Kashyap et al. (Shimla, India, 2018)[7] | 24 | 58.3 | 41.7 | 20.8 | 37.5 | 85.72 | 14.28 | Nil | 41 |
| Our south Indian study | 40 | 82.5 | 65 | 15 | 20 | 78.78 | 6.06 | 15.16 | 55.65 |
CM = corona mortis, PS = pubic symphysis
In our study, the venous variant was more predominant (78.78%), which is similar to the studies done in Shimla (85.72%)[7] and Kerala (54.07%),[6] where the venous variant was more predominant.
In our study, the bilateral presence of corona mortis was 65%, whereas it was 41.7% in the study from Shimla.[7]
The mean distance of the corona mortis from the pubic symphysis in our study was 55.65 mm, whereas it was 41 mm in the study done in Shimla.[7]
Conclusions
The identification and isolation of the corona mortis are very important during pelvic-acetabular and hernia surgeries. The incidence of corona mortis was 82.5% in our study. Our study was dominated by the venous variant compared with the arterial and arteriovenous variants. Corona mortis had gender variations: it was present in all the females in our study, whereas it was not so among males as per our study. Our sample size is small. A large multicentric study may be necessary to confirm our results.
Financial support and sponsorship
Nil.
Acknowledgments
We would like to thank Prof. T. Jeyasingh and the Department of Forensic Medicine, Coimbatore Medical College Hospital for their support.
Conflicts of interest
There are no conflicts of interest.
References
- Corona mortis: An anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat. 2007;20:433-9.
- [CrossRef] [PubMed] [Google Scholar]
- The anatomy of pelvic corona mortis vessels in black Africans: A cadaveric study. East Afr Orthop J. 2015;9:67-71.
- [Google Scholar]
- The incidence and location of corona mortis: A study on 75 cadavers. Acta Orthop Scand. 2004;75:53-5.
- [CrossRef] [PubMed] [Google Scholar]
- An anatomical study of corona mortis and its clinical significance. Chin J Traumatol. 2004;7:165-9.
- [Google Scholar]
- south Indian cadaveric study on obturator neurovascular bundle with a special emphasis on high prevalence of “venous corona mortis”. Injury. 2016;47:1452-5.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomical considerations on surgical implications of corona mortis: An Indian study. Ital J Anat Embryol. 2017;122:127-36.
- [Google Scholar]
- The majority of corona mortis are small calibre venous blood vessels: A cadaveric study of north Indians. Hip Pelvis. 2019;31:40-7.
- [CrossRef] [PubMed] [Google Scholar]
- Anatomical and clinical implication of corona mortis in the anterior approaches of pelvis in Sudanese patient. Open J Orthop. 2021;11:85-95.
- [CrossRef] [Google Scholar]




