
Translate this page into:
Computed tomography scan morphometric study of adolescent vertebral laminae: From three-dimensional reconstruction to laminar hook
Address for correspondence: Dr. Elie Haddad, Department of Pediatric Surgery, Nord University Hospital, Saint Etienne 42055, Cedex 02, France. E-mail: elie.haddad@chu-st-etienne.fr
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Haddad E, Soulaine C, Dohin B. Computed tomography scan morphometric study of adolescent vertebral laminae: From three-dimensional reconstruction to laminar hook. J Orthop Allied Sci 2019;7:12-6.
Abstract
INTRODUCTION:
The authors report a descriptive analysis of spine computed tomography (CT) scan to describe the anatomy of the laminae of T2 and T3 vertebrae. The aim of the study was to establish reference data in the adolescent population. These data could be useful to improve the effectiveness of laminar hooks. Hook-claw anchorage has been considered as one of the best choices in terms of safety and durability in the spine surgery.
MATERIALS AND METHODS:
We systematically reviewed CT scans of 14–16-year-old healthy individuals who underwent CT scans in other indications than scoliosis during a 2-year period. Patients with spine, chest, or bone disease were excluded. The Risser sign was ≥ 2. CT scan data were converted into a three-dimensional reconstruction.
RESULTS:
Seven hundred and fifty measures were collected from 30 CT scans matching with the inclusion/exclusion criteria. The mean age was 15-years old. Gender was mixed. Mean T2 lamina's upper half height was 8.9 mm (8.2–9.6) corresponding to a thickness of 7.1 mm (6.6–7.7). Mean T3 lamina's lower half height was 9.0 mm (6.9–10.4) corresponding to a thickness of 7.3 mm (6.8 à 7.9).
DISCUSSION:
No previous study reported these data in adolescents. Laminae in adolescents appeared to be slightly oversized in this study relative to the previous reports in adults. It seems that the intracanal part length of the hook and depth of the gorge should be adapted in order to improve fitting of the implant with laminae.
CONCLUSION:
This study brings new data in the knowledge of anatomical characteristics of the vertebras that should help to improve safety and stability of implants as laminar hook and hook claw.
Keywords
Anatomy
computed tomography scan
laminae
laminar hook
spine
spine instrumentation
spine osteosynthesis
vertebrae

Introduction
Vertebral lamina is an easy and safe anchorage site when performing surgical correction of spine deformity. Hook claw at the top of the instrumentation provides a strong anchorage and a soft mechanical transition to the adjacent-free spine when performing spinal arthrodesis in spine deformity. It seems to be one of the best compromises in terms of safety, efficiency, and potential complication.[1-4] The authors have been using this implant for several years with positive results. Despite a long practice using hook claws, a specific implant had never been specially designed to the upper thoracic spine. It seemed to the authors that primary stability, easiness to implant, and bulk of implant could be improved using hooks with dimensions based on the anatomical features of the laminae. For example, the length of the intraspinal canal hook part could be adapted to the lamina's height: avoiding mechanical conflict between hooks when using hook claw at one vertebral level. In another way, using hooks with a gap larger than the thickness of the laminae could decrease its primary stability and increase the risk of implant pull-off. If anatomical description of the vertebral lamina is well-known in adults, its morphometric description is rare in the literature compared to other vertebral structures, especially in adolescents.[5-11] To the best of our knowledge, to date, no spinal implant has been specifically sized and shaped to optimize anchorage at the upper part of the thoracic spine in adolescents. The aim of this study was to quantify the morphological parameters of the second and third thoracic vertebral laminae in adolescents. Knowledge of anatomical features might allow improvement of the implants in order to obtain a better fitting to anatomy.
Materials and Methods
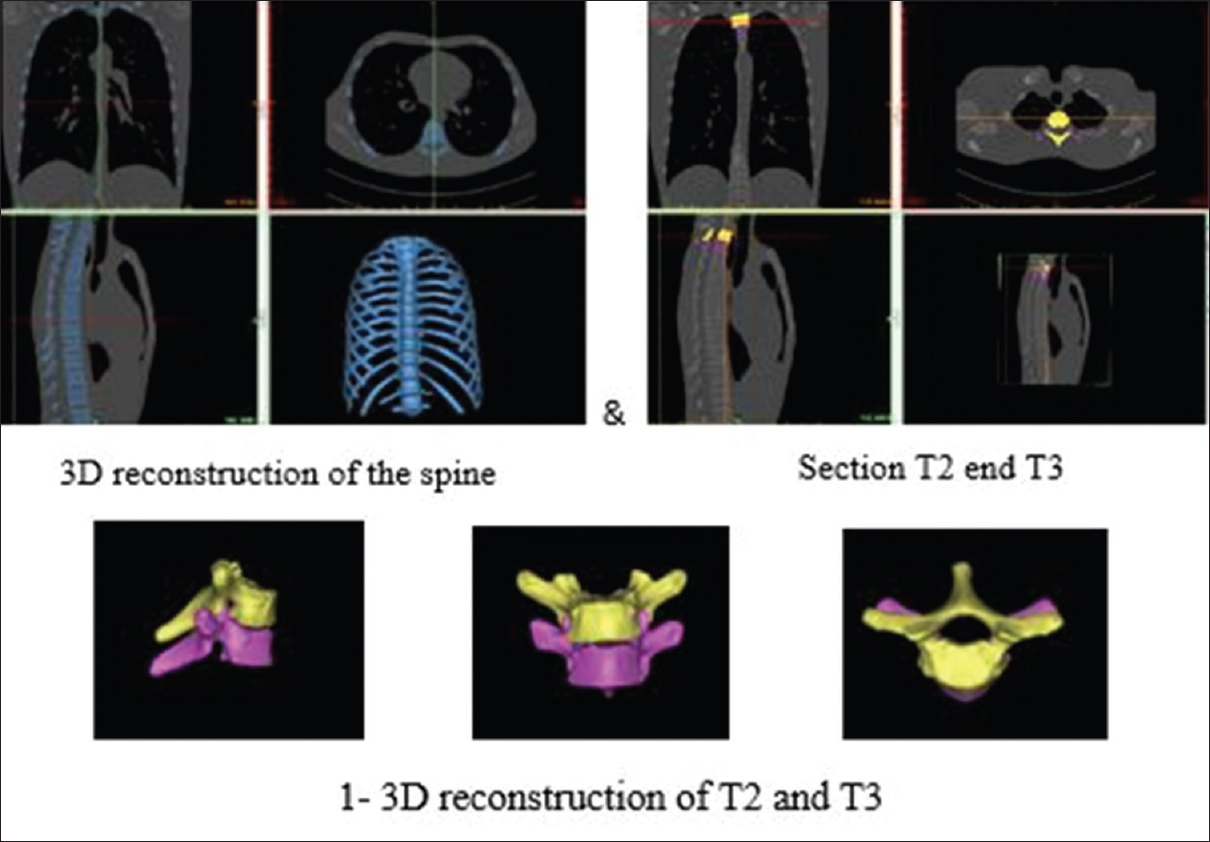
The present study reports morphologic data about the 2nd and 3rd thoracic vertebrae (T2 and T3) laminae. It is about a retrospective study performed with agreement of the local ethics committee (Ref: IRBN552016/CHUSTE). We collected 55 adolescent's chest computed tomography (CT) scans performed in our institution between 2015 and 2016. Inclusion criteria were: adolescents from 14 to 16 years old, without bone disease, and chest or spinal deformities. Gender was not considered. CT scans with an insufficient quality (wider than millimetric cross section) were rejected. Radiological charts were collected, and after being anonymized, the data were converted to a three-dimensional (3D) format to be studied. We made 3D reconstructions (software: Mimics 18.0 Materialise™ company, Louvain, Belgique) of T2 and T3 vertebrae with high-quality resolution, then we pinpointed optimum measures. Collected measures were statistically analyzed (Research and Development Department, Medicrea Europe™ company, Rillieux la Pape, 69140, France) using the Solidworks 2016® software (Dassault Systèmes™ company, Vélizy-Villacoublay, France).
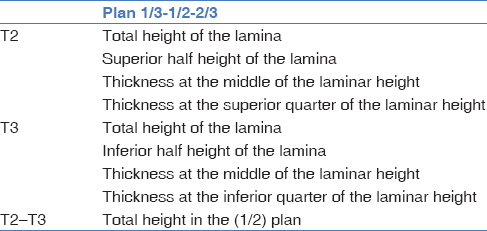
We collected 25 measures on each vertebra: height and thickness of the lamina at two different levels and three sagittal planes [Table 1 and Figures 1a,b and 2]. A statistical comparison between the right and left laminae was performed on five patients in order to study (based on Wilcoxon test) the significance of our results and the influence of the lamina's side on these results (P< 0.05).
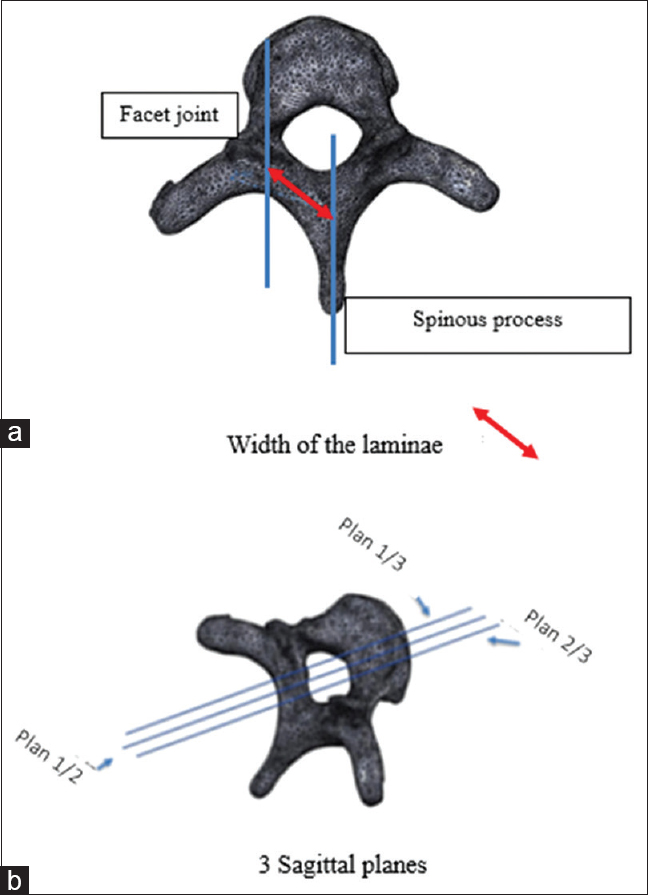
- (a) Width of the laminae, (b) 3 Sagittal planes
- Height and thickness at different levels in T2 and T3
Note: Measure method:
3D reconstruction of T2 and T3 vertebrae [Figure 3].
-
Reference plans for measures
The width of the lamina was measured between the medial limit of the facet joints and the intersection between the lamina and the spinous process [Figure 1a].
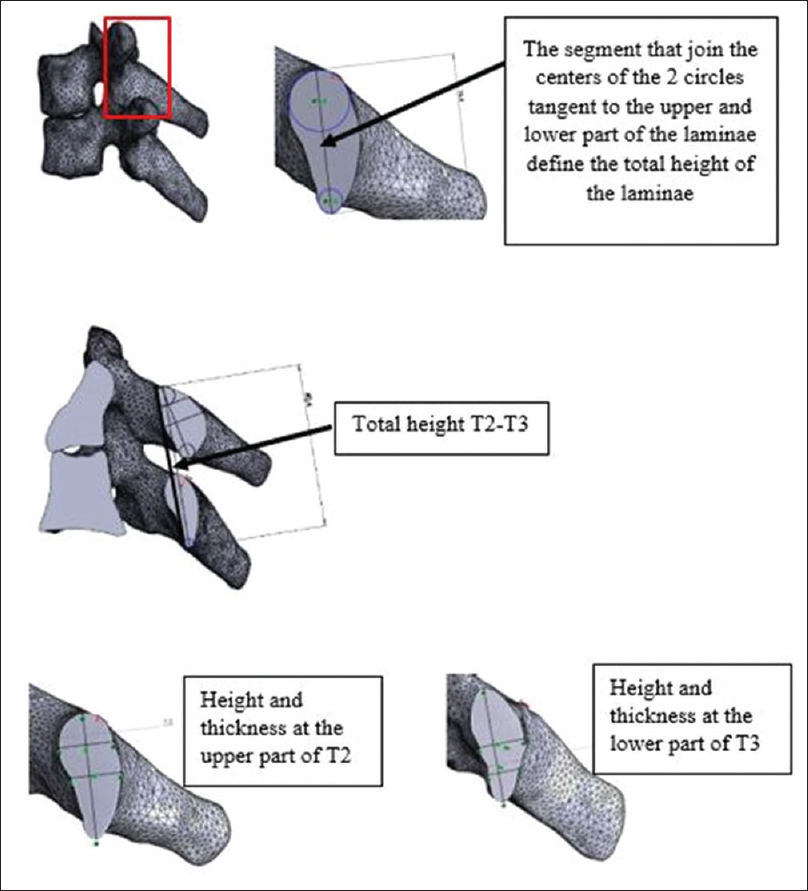
Two sagittal plans, perpendicular to the axis of the lamina were defined cutting lamina into three equivalent parts: 1/3 medial and 1/3 lateral. One plan was defined at the middle of the lamina (1/2) [Figure 1b]. At these three plans, the height of the lamina was determined as the distance between the upper edge and lower edge of the lamina (as a cross-sectional view). Total lamina's height was divided into two parts: superior (upper) half and inferior (lower) half [Figure 2].
The thickness of the lamina was measured at the superior quarter and at the midheight in T2 vertebrae (upper part) and at the inferior quarter and midheight in T3 vertebrae (lower part) [Figure 2].
The reproducibility of the measurements was considered reliable because of using a computerized geometric construction on each 3D image.
- Measure method
Results
Among the 55 CT scans, which met the eligibility criteria in the period defined, 25 has been excluded for lack of quality. The 30 remaining CT scans allowed a total of 750 measures, which were statistically analyzed [Chart 1]. Patients' mean age was 15-years old. There were 75% of females. The Risser sign was ≥2 in all cases.

At T2 level, lamina's superior half height (mean value) was 8.9 mm ([8.2–9.6]; standard deviation [SD]: 1.4 mm) and its corresponding mean thickness was 7.1 mm ([6.6–7.7]; SD: 1.1). The upper quarter lamina's mean thickness was 7.0 mm ([6.4–7.5]; SD: 1.1 mm).
At T3 level, lamina's inferior half height (mean value) 9.0 mm ([6.9–10.4]; SD: 3.5 mm) and its corresponding mean thickness was 7.3 mm ([6.8 à 7.9]; SD: 1.1 mm). The lower quarter lamina's mean thickness was 5.4 mm ([4.5 à 6.1]; SD: 1.6 mm).
To dismiss any effect of the laterality, we tested bilateral measurement in five cases. Based on the Wilcoxon test, we did not find a significant difference between measurements on the left and right laminae (P = 0.314).
Discussion
Our study describes morphometric characteristics of the second and third thoracic vertebral lamina in the adolescent. These data are known in adult populations with anatomic studies based on Corpse or CT scan images.[5-9,11]
Computed morphometric data provided by CT scan imaging reduces surgical difficulties and complications and surgeons can even optimize their surgery using “custom-fitted implants” based on these data.[12,13]
We choose CT scan images with high-quality resolution to ensure the highest precision for our measure's method.
Our study has a limited number of patients, but the sample is representative of adolescent's population candidate to spine arthrodesis for adolescent idiopathic scoliosis in terms of civil age, bone maturity (Risser sign), and gender.
In fact, based on our results, the length of the intraspinal canal hook part must not exceed half the height of the laminae (8.9 mm for T2 and 9.0 mm for T3) to avoid hooks contact when the hook claw is applied on 1 vertebral level. The depth of the hook gap must be slightly smaller than the thickness of the lamina at the midheight (7.1 mm for T2 and 7.3 mm for T3) providing to the hook a direct anchorage on the laminae and increasing its primary stability. These characteristics might avoid neurological complications, facilitating surgical procedure, and preventing risk of pulling off or intracanal overhanging even in osteoporotic spine such as in cerebral palsy scoliosis or osteogenesis imperfecta cases.[14] Biomechanical studies confirmed the interest of using hooks in osteoporotic spine.[15-17]
Anatomy of adult's vertebras is well known. Nevertheless, morphometric parameters of laminae have rarely been studied compared to other parts of the vertebrae (i.e., pedicles, facet joints, or vertebral body).[6,7,11,18,19] Zindrick et al. in 1989 established the thoracic laminar height and thickness as factors affecting the penetration of wires into the spinal canal. Based on the evaluation of 13 cadaveric spines, they reported values ranging from 18 to 24 mm for laminar height and from 7 to 8 mm for laminar thickness (highest value).[20] Pampliega et al. in 1992 documented mean laminar height up to 20 mm and laminar thickness up to 5–6 mm (highest value) between T4 and L2 in eight human cadavers.[21] Gayet et al. in 1998 found a mean value of 17 ± 2 mm for laminar height and 6 ± 2 mm for laminar thickness in 72 thoracic vertebras (T1 to T8) of the human cadaveric spine (mean age 67 years).[14] Xu et al. in 1999 reported the dimensions of laminae from C2 to L5 in 37 cadaveric adult spines (42–74 years old – 21 males) in order to provide quantitative data about them.[10] Their measurements, made with an electronic caliper, included laminar height and thickness. Regarding gender, no significant difference was found in their study despite measurements were slightly greater in male specimens than in female. These authors made three measurements of thickness: (1) 2 mm below the superior laminar margin, (2) 2 mm above the inferior laminar margin, and (3) equidistant point from the two previous points.
Data collected in the present study on adolescent vertebrae highlight a difference with those presented by Xu et al. about human adult vertebrae [Chart 2]. Decreasing the size of the laminae underlines the potential interest of specifically sized implants for the adolescent population and justifies the present study. More studies comparing adults and adolescents with same ethnic characteristics, and in the same period, could confirm our findings.
Moreover, it has been reported that hook claw at the upper part of spinal instrumentation in scoliosis could improve mechanical transition between the instrumented spine (rigid) and the mobile spine above and decrease the incidence of proximal junctional kyphosis.[4]

The present study brings anatomical data in order to improve hook-claw implant in terms of stability and safety. These data have not been documented previously, and it is thefirst report about adolescent's anatomy of the vertebral laminae. Obviously, further biomechanical studies should be performed in the future to prove the effectiveness of the hook claw based on the anatomical characteristics of the vertebral laminae.
Conclusion
This study brings new data in the knowledge of anatomical characteristics of the vertebras. The best the implants fit the anatomy, the more surgeons can expect in terms of stability and safety.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Comparative analysis of pedicle screw versus hybrid instrumentation in adolescent idiopathic scoliosis surgery. Int Orthop. 2008;32:523-8.
- [Google Scholar]
- Evaluation of proximal junctional kyphosis in adolescent idiopathic scoliosis following pedicle screw, hook, or hybrid instrumentation. Spine (Phila Pa 1976). 2010;35:177-81.
- [CrossRef] [PubMed] [Google Scholar]
- Type of anchor at the proximal fusion level has a significant effect on the incidence of proximal junctional kyphosis and outcome in adults after long posterior spinal fusion. Spine Deform. 2013;1:299-305.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical analysis of the proximal adjacent segment after multilevel instrumentation of the thoracic spine: Do hooks ease the transition? Global Spine J. 2016;6:335-43.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of the morphometric characteristics of the thoracic and lumbar pedicles. Spine (Phila Pa 1976). 1987;12:160-6.
- [CrossRef] [PubMed] [Google Scholar]
- Articular facets of the human spine. Quantitative three-dimensional anatomy. Spine (Phila Pa 1976). 1993;18:1298-310.
- [CrossRef] [PubMed] [Google Scholar]
- Thoracic human vertebrae. Quantitative three-dimensional anatomy. Spine (Phila Pa 1976). 1991;16:888-901.
- [CrossRef] [PubMed] [Google Scholar]
- Projection of the lumbar pedicle and its morphometric analysis. Spine (Phila Pa 1976). 1996;21:1296-300.
- [CrossRef] [PubMed] [Google Scholar]
- Projection of the thoracic pedicle and its morphometric analysis. Spine (Phila Pa 1976). 1997;22:233-8.
- [CrossRef] [PubMed] [Google Scholar]
- The quantitative anatomy of the laminas of the spine. Spine (Phila Pa 1976). 1999;24:107-13.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative morphometric study of thoracic spine A preliminary parameters statistical analysis. Eur J Orthop Surg Traumatol. 2000;10:85-91.
- [CrossRef] [Google Scholar]
- Reconstruction of thoracic spine using a personalized 3D-printed vertebral body in adolescent with T9 primary bone tumor. World Neurosurg. 2017;105:1032.e13-20.
- [CrossRef] [PubMed] [Google Scholar]
- Systematic review of 3D printing in spinal surgery: The current state of play. J Spine Surg. 2017;3:433-43.
- [CrossRef] [PubMed] [Google Scholar]
- Study of the posterior thoracic vertebral arc's resistance to traction. Rachis. 1998;1:19-26.
- [Google Scholar]
- Classification of different posterior vertebral mountings according to their tensile strength. Rachis. 2004;16:51-60.
- [Google Scholar]
- Influence of bone mineral density on the fixation of thoracolumbar implants. A comparative study of transpedicular screws, laminar hooks, and spinous process wires. Spine (Phila Pa 1976). 1990;15:902-7.
- [CrossRef] [PubMed] [Google Scholar]
- Axial and tangential fixation strength of pedicle screws versus hooks in the thoracic spine in relation to bone mineral density. Spine (Phila Pa 1976). 2002;27:937-42.
- [CrossRef] [PubMed] [Google Scholar]
- A morphometric study of human lumbar and selected thoracic vertebrae. Spine (Phila Pa 1976). 1987;12:362-7.
- [CrossRef] [PubMed] [Google Scholar]
- Vertebral body and posterior element morphology: The normal spine in middle life. Spine (Phila Pa 1976). 1988;13:1082-6.
- [CrossRef] [PubMed] [Google Scholar]
- Factors influencing the penetration of wires into the neural canal during segmental wiring. J Bone Joint Surg Am. 1989;71:742-50.
- [CrossRef] [Google Scholar]
- Neurologic complications after sublaminar wiring. An experimental study in lambs. Spine (Phila Pa 1976). 1992;17:441-5.
- [CrossRef] [PubMed] [Google Scholar]




