
Translate this page into:
Complete avulsion of the adductor longus in a semi-professional football player: Rapid return to play with nonoperative treatment
Address for correspondence: Dr. Vince W. Lands, St. Luke′s University Health Network, 801 Ostrum Street, Bethlehem, Pennsylvania 18015, USA. E-mail: vince.lands@sluhn.org
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Lands VW, Avery DM, Puccio ST. Complete avulsion of the adductor longus in a semi-professional football player: Rapid return to play with nonoperative treatment. J Orthop Allied Sci 2016;4:45-8.
Abstract
The adductor longus has become recognized as one of the more commonly injured muscles in the medial compartment. Acute complete rupture injuries occurring at the proximal aspect of the muscle are less common. Limited data exist regarding management of the injuries in athletes required for return to play and functioning. The current data favors operative management; however, nonoperative treatment may be a viable option. Nonoperative management of avulsion injuries of the proximal adductor longus tendon may prove equal results to surgical repair in return to play and functioning. A semi-professional football player sustained a left groin injury while participating in the play. Due to continued pain, swelling, and suspicion of injury, a magnetic resonance imaging was performed diagnosing a complete tear of proximal adductor longus tendon. Physical examination, strength, and range of motion were recorded until the patient was able to function normally without strength deficit, the range of motion loss, and the return of speed. The player was treated nonoperatively and was eventually allowed to return to play. The time of return to play was 6 weeks. Strength deficit was not appreciated or loss of motion and player was able to return to baseline function. Nonoperative management of complete avulsion injuries of the proximal adductor longus tendon result in faster return to play than operative management even if significant retraction is present.
Keywords
Adductor
groin
injury

Introduction
Groin injuries in athletes can become difficult task for practitioners to evaluate and treat due to the complexity of injuries. There are numerous pathologic processes that can mimic one another. Injuries can include adductor strains, recalcitrant tendinopathy, adductor tears, or even athletic pubalgia. Pubalgia is defined as an injury to the rectus abdominis insertion onto the pubis symphysis, often accompanied by an injury to the conjoined tendon insertion and the adductor longus attachment to the pelvis.[1,2,3,4,5]
The thigh compartment contains an anterior, medial, and posterior compartment. The medial compartment of the thigh contains the gracilis, adductor longus, adductor magnus, and adductor brevis. Injury to the medial compartment is much less common than its anterior or posterior counterparts.[6] The adductor longus has become recognized as one of the more commonly injured muscles in the medial compartment. Most injuries occur proximally at the musculotendinous junction although there have been reports of injuries occurring at the proximal and distal parts of the adductor longus muscle. Injuries occurring at the origin of the muscle are infrequent with limited reported data.[7,8,9,10,11]
We present a case of a 27-year-old male, semi-professional athlete, who incurred an idiopathic proximal avulsion of his adductor longus. Following a structured therapy protocol, he was able to return to game play within 6 weeks with nonoperative management. To our knowledge, there is limited data in regards to outcomes of nonoperative treatment of idiopathic proximal avulsion injuries, but there have been a number of published articles in regards to the outcomes of surgical treatment of these injuries. There has been one published article of a proximal osseous avulsion,[12] but our case does not present with such. Distal ruptures seem to be more common with some recommending acute repair.[12] Also reported in the literature are controlled surgical releases of the adductor longus for pathologic conditions such as recalcitrant adductor tendinopathy.[5] Treatment options vary for lesions to the adductor longus. These options are determined by proximity, osseous abnormalities, and acuity. The subject of discussion will focus on proximal idiopathic avulsions of the adductor longus with significant retraction and early return to play. Informed and written consent was obtained from the patient for print and electronic publication of this case report and proofs. There are no disclosures to report.
Case Report
A 27-year-old male semi-professional football player sustained an injury to his left groin during a game. While sidestepping and engaged with another player, he felt a pop in his left groin area that was accompanied by immediate pain and weakness. The player was escorted to the locker room where examination revealed moderate swelling and ecchymosis over the groin and proximal thigh. He had tenderness to palpation just lateral to his symphysis pubis, pain with passive abduction, and pain on resisted adduction (adductor squeeze test) and resisted hip flexion were limited. He was not allowed to return to play.
One week following the injury, a magnetic resonance imaging of the left hip was obtained to evaluate his injury and revealed a complete avulsion of his left adductor longus from its proximal origin. Figure 1a-c shows complete rupture of adductor tendon from the pubis, with 5.1 cm retraction and adjacent edema in the medial compartment. Grade 1 strains were shown in pectineus, adductor brevis, and adductor magnus.
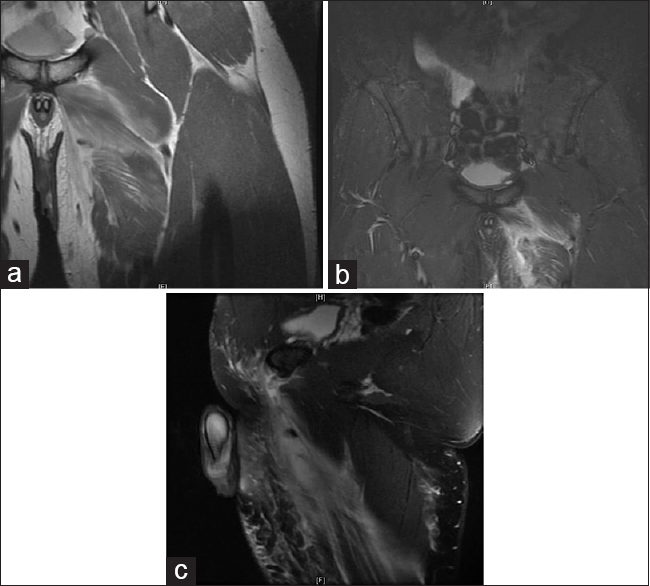
- Reveal postinjury magnetic resonance imaging's of a 27-year-old linebacker with obvious swelling, ecchymosis, and palpable defect of medial compartment. The study revealed complete rupture of adductor tendon from the pubis, with 5.1 cm retraction and adjacent edema in medial compartment. Grade 1 strains shown in pectineus adductor brevis and adductor magnus. (a) Coronal, proton dense image. (b) Coronal, short tau inversion recovery image. (c) Sagittal T2-weighted image
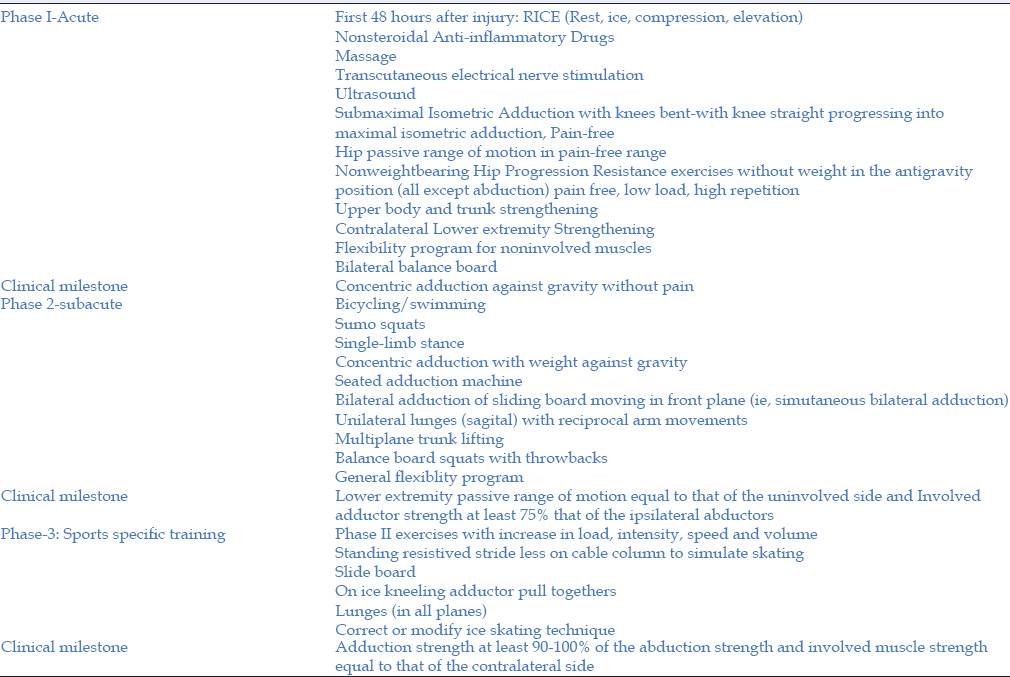
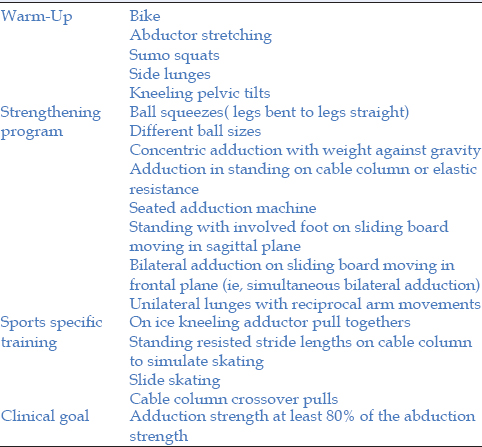
After a thorough discussion of operative and nonoperative treatment, the player elected for nonsurgical care. Rest, ice, and modified weight bearing were instituted for the 1st week after injury. Pain relief was adequate with oral anti-inflammatories. During his 2nd week, gradual stretching exercises were instituted, utilizing a hot whirlpool, for approximately 5 days/week for 2 h/day. The therapy protocol was adapted from article written by Tyler et al.,[1] however was modified to fit the players availability of resources. The protocol consisted of three phases including acute, sub acute, and sports specific training. The therapy protocol is listed in Tables 1 and 2.
Weeks two through four, the player was able to progress to routine stretching, jogging, and light strengthening; by the end of his 4th week, his pain was mild, and his strength was 4/5. Given his progression, strength training ensued with cutting exercises beginning at the 5th week. Strength testing and range of motion were assessed and compared to his contralateral leg. Testing was done by the adductor squeeze test and resisted hip flexion which revealed 5/5 motor strength and absence of discomfort. The range of motion for hip abduction did reveal loss of 10° compared to contralateral limb. The loss of motion did not limit the athlete's ability to perform. He was able to return to game play at the end of week 6. Following the conclusion of the season and at 3 months postinjury, the player returned without any recurrence of discomfort or loss of strength and full return of motion with continued stretching.
Discussion
Injuries to the adductor longus are uncommon but are typically seen in soccer, football, and hockey.[9,10,11,13,14] In football players, these injuries are most commonly seen in linebackers.[15] Injuries are graded according to a standard muscle injury scale with Grade I signifying a strain, Grade II a partial tear, and Grade III a complete tear or avulsion. Preexisting discomfort in the groin can be an important historical component as degenerative change within the tendon can predispose to rupture.[3,15]
Grade I injuries are usually incurred secondary to inadequate warm-up and stretching before athletic participation.[3] Grade II and III injuries in the adductor longus typically occur at the distal insertion and are usually due to eccentric loading on the medial compartment.[3]
Suspicion for these injuries should be high when an athlete reports popping in the groin area after acute injury with obvious medial compartment deformity, swelling, ecchymosis, pain with passive abduction, resisted adduction, and difficulty with ambulation.[1,2,4,16]
Treatment surrounding these injuries has been controversial as there have been a few reports on operative and nonoperative intervention for these injuries. Full return of strength to allow high-level athletic participation in activities such as cutting seems to give operative treatment consideration.[10,11,12,14,15] A case series of National Football League players, comparing operative versus nonoperative intervention, demonstrated faster return to play in the nonoperative group which had retraction of the proximal tendon between 1 and 3 cm and no difference in return of strength.[15]
Questions still surround this injury and its treatment. Does the amount of retraction affect adequate nonoperative treatment? Does preexisting groin pain from degeneration of the tendon affect operative or nonoperative repair? Moreover, how long should a player rehabilitate before return to play, as a wide range of values has been shown.[1,2,16]
We present a semi-professional player with an idiopathic proximal avulsion of the adductor longus with significant retraction and a rapid return to play with full strength. Perhaps, his biology was adequate to rehabilitate in such a rapid manner, but this does give evidence to support the ability of nonoperative treatment to return athletes to high-level competition? Also would this suggest that pending a player's symptoms, would an accelerated program be an effective and safe treatment option? Idiopathic injuries to the adductor longus continue to occur in high-functioning athletes, and nonoperative treatment for these injuries may very well be a safe option for athletes to return to full play.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Groin injuries in sports medicine. Sports Health. 2010;2:231-6.
- [CrossRef] [PubMed] [Google Scholar]
- Groin injuries and groin pain in athletes: Part 1. Prim Care. 2005;32:163-83.
- [CrossRef] [PubMed] [Google Scholar]
- Zigler Terry Pulled Groin Muscle. Available from: http://www.sportsmd.com/Articles/id/23.aspx#sthash.rdVppOcn.dpuf; http://www.sportsmd.com. [Last retrieved on 2014 Sep 22]
- [Google Scholar]
- Groin injuries in sport: Treatment strategies. Sports Med. 1999;28:137-44.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical technique for treatment of recalcitrant adductor longus tendinopathy. Arthrosc Tech. 2014;3:e293-7.
- [CrossRef] [PubMed] [Google Scholar]
- Gross Anatomy. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008.
- [Google Scholar]
- Isolated traumatic rupture of the adductor longus muscle of the thigh. Clin Orthop Relat Res. 1972;88:64-6.
- [CrossRef] [PubMed] [Google Scholar]
- Adductor avulsive injuries near the symphisis pubis. Radiology. 1976;120:567-9.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical management of a completely avulsed adductor longus muscle in a professional equestrian rider. Case Rep Orthop. 2014;2014:828314..
- [CrossRef] [PubMed] [Google Scholar]
- Adductor longus ruptures in elite sportsmen - Pitfalls of surgical repair: A report of two cases. BMJ Case Rep 2013:2013. pii:bcr2013010073
- [CrossRef] [PubMed] [Google Scholar]
- Adductor longus rupture in professional football players: Acute repair with suture anchors: A report of two cases. Am J Sports Med. 2004;32:243-5.
- [CrossRef] [PubMed] [Google Scholar]
- Complete osseous avulsion of the adductor longus muscle: Acute repair with three fiberwire suture anchors. Arch Orthop Trauma Surg. 2007;127:613-5.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical recovery of two hip adductor longus ruptures: A case-report of a soccer player. BMC Res Notes. 2013;6:205..
- [CrossRef] [PubMed] [Google Scholar]
- Acute avulsion of the fibrocartilage origin of the adductor longus in professional soccer players: A report of two cases. Clin J Sport Med. 2008;18:167-9.
- [CrossRef] [PubMed] [Google Scholar]
- Success of nonoperative management of adductor longus tendon ruptures in National Football League athletes. Am J Sports Med. 2009;37:1394-9.
- [CrossRef] [PubMed] [Google Scholar]
- Management of groin pain in athletes. Br J Sports Med. 1997;31:97-101.
- [CrossRef] [PubMed] [Google Scholar]




