
Translate this page into:
Comparison of transforaminal endoscopic lumbar foraminotomy (TELF) in patients with degenerative scoliosis and patients with normal alignment
*Corresponding author: Chay-You Ang, Department of Orthopaedic Surgery, Singapore General Hospital, Singapore. angchayyou@msn.com
-
Received: ,
Accepted: ,
How to cite this article: Ang GY, Bae J, Jeong SK, Shin SH, Lee SH. Comparison of transforaminal endoscopic lumbar foraminotomy (TELF) in patients with degenerative scoliosis and patients with normal alignment. J Orthop Spine 2023;11:56-60. doi: 10.25259/Joasp_46_23
Abstract
Objectives
Transforaminal endoscopic lumbar foraminotomy (TELF) is a well-described method of treating foraminal stenosis. However, there is little literature examining the usage of TELF to treat foraminal stenosis in patients with degenerative scoliosis. TELF is an attractive option for such patients as it results in lesser blood loss, shorter recovery time, and lower infection rates as compared to fusion surgery. However, TELF neither corrects the deformity nor alters the natural history of the disease. Therefore, the outcomes of TELF in patients with degenerative scoliosis may be worse than those without deformities. This study aims to compare the outcomes of TELF in these two groups of patients.
Material and Methods
This is a retrospective study of 19 patients who underwent TELF from July 2012 to April 2015. Eight patients had degenerative scoliosis, and 11 were without scoliosis. Visual analog scale and Oswestry disability index (ODI) scores were collected at 3 months postsurgery. Patient outcomes were graded as excellent, good, fair, and poor using a modified MacNab’s criteria.
Results
Both groups had significant improvements in back pain, leg pain, and ODI scores postoperatively. There were no differences between the two groups when comparing the preoperative and postoperative back pain, leg pain, and ODI scores. The majority of patients rated their outcomes as excellent or good.
Conclusion
The short-term outcomes of TELF in patients with degenerative scoliosis are comparable to those without scoliosis. Improvements in back and leg pain after surgery are expected. We recommend it as a palliative treatment for patients who are unable to undergo major surgery.
Keywords
Degenerative scoliosis
Endoscopic spine surgery
Foraminal stenosis
Transforaminal

INTRODUCTION
Transforaminal endoscopic lumbar foraminotomy (TELF) is a well-described method of treating foraminal stenosis. According to the literature, TELF is highly successful in reducing pain and disability in such patients with minimal serious adverse events.1 In comparison, there is a paucity of literature examining the usage of TELF to treat foraminal stenosis in patients with degenerative scoliosis (DS).
DS is a commonly encountered clinical problem in the ageing population. In East Asian populations, the prevalence of DS is more than 30%, with a higher incidence among females and individuals above 60 years old.2 DS is progressive, and patients are likely to experience symptoms of nerve impingement as the curvature worsens. Nerve impingement most commonly occurs within the intervertebral foramina on the concave side of the curve. This is due to the narrowing of the intervertebral foramina by the coronal deformity and hypertrophy of the facet joint, which exacerbates the stenosis.3–5 As such, the correction of the deformity with either direct or indirect decompression of the neural elements is frequently advocated by many authors.3,4,6 However, such surgeries are often major procedures with significant risks involved, and in the elderly population, such risks are compounded by comorbidities and osteoporosis.
TELF is an attractive option for such patients as it decompresses the neural elements, thereby providing symptomatic relief and it avoids hardware-related complications. Furthermore, it results in lesser blood loss, shorter recovery time, and lower infection rates as compared to fusion surgery.7 Several authors previously reported on the outcomes of TELF in patients with DS and had encouraging results.7–9 However, endoscopic foraminotomy does not correct the underlying deformity that contributed to the foraminal stenosis and does not alter the natural history of the disease. Therefore, without correcting the primary pathology, the outcomes of TELF in patients with DS may be worse than those without deformities. Hence, we propose this study to compare the clinical outcomes of patients with DS who underwent TELF versus patients with normal spinal alignment.
MATERIAL AND METHODS
This is a retrospective cohort study of 19 patients who underwent TELF at our institute from July 2012 to April 2015. This research has been approved by the Institutional Review Board (IRB) of the author’s affiliated institution. Patients were excluded if they had prior lumbar spine surgery or if they had scoliosis secondary to other causes. Patients were also excluded if the lumbar radiographs showed dynamic instability or if they had other concomitant pathologies such as fracture, infection, or spine tumour.
A total of 23 patients underwent TELF during that period, and four patients were excluded as they had adjacent segment disease due to previous fusion surgeries. Of the remaining 19 patients, eight had DS (degenerative scoliosis [DS] group), and 11 had spinal alignment within normal limits (no scoliosis [NS] group). The eight patients in the DS group were confirmed to have DS based on the patient’s history, radiological findings, and previous radiographs.
All patients presented with severe back pain and radicular leg pain that was unresponsive to conservative treatment. Preoperative radiographs of the entire spine were obtained using EOS™ (EOS Imaging, ATEC Spine, USA), and routine lumbar spine radiographs with flexion and extension views were performed for all patients. Cobb angles were measured on the EOS™ images by two spine fellows who were not involved in the surgeries. An average of the two measurements was taken as the final measurement. All patients in the DS group had a Cobb angle of more than 10°, while patients in the NS group had a Cobb angle of 10° or less.
Preoperative Magnetic resonance imaging (MRI) of the lumbar spine showed severe foraminal stenosis in all patients. All patients within the DS group received counselling regarding alternative surgical options, including fusion and correction of the deformity. However, all patients chose full endoscopic surgery due to a strong aversion toward major surgery.
The patients were seen at three months postsurgery. Visual analogue scale (VAS) scores for back pain and leg pain and Oswestry disability index (ODI) scores were collected during that visit. Patient outcomes were graded as excellent, good, fair, and poor using a modified MacNab’s criteria at the three-month follow-up.
Statistical analysis
A paired t-test was used for the comparison of VAS and ODI scores between the pre- and postoperative periods. A P-value <0.05 was defined as statistically significant. All analyses were performed using the GraphPad QuickCalcs Web site: http://www.graphpad.com/quickcalcs/ (accessed January 2023).
RESULTS
In the DS group, one patient had two levels of surgery, and seven patients had single-level surgery. The remaining 11 patients in the NS group had single-level surgery. The Cobb angle was significantly higher in the DS group as compared to the NS group. The most commonly operated level was at L4/5. Patients in the DS group were significantly older than the NS group, corresponding to the natural history of DS [Table 1].
| DS | NS | P-value | |
|---|---|---|---|
| Age (range) | 75.8 | 63.8 | <0.05 |
| (66–87) | (47–79) | ||
| N | 8 | 11 | |
| Gender | |||
| Male | 2 | 7 | |
| Female | 6 | 4 | |
| Cobb angle (degrees [SD]) | 18.3 (8.2) | 5.4 (2.4) | <0.05 |
| Level of surgery | |||
| L3/4 | 2 | 2 | |
| L4/5 | 6 | 10 | |
| L5/1 | 1 | 2 | |
| Pre-op VAS score—back pain (SD) | 7.6 (1.3) | 7.6 (1.3) | 0.99 |
| Pre-op VAS score—leg pain (SD) | 8.1 (0.8) | 7.8 (1.0) | 0.48 |
| Pre-op ODI (SD) | 34.1 (5.0) | 29.3 (7.6) | 0.14 |
DS: Degenerative scoliosis, NS: No scoliosis, ODI: Oswestry disability index,
SD: Standard deviation, VAS: Visual analogue scale
In both groups, there were significant improvements in back pain, leg pain, and ODI scores after surgery. The back pain scores improved from 7.6 (95% Confidence Interval; CI, 6.5–8.7) to 2.9 (95% CI, 2.2–3.6) in the DS group and it improved from 7.6 (95% CI, 6.8–8.5) to 2.8 (95% CI, 2.3–3.3) in the NS group. The leg pain scores improved from 8.1 (95% CI, 7.4–8.8) to 2.9 (95% CI, 2.1–3.7) in the DS group and it improved from 7.8 (95% CI, 7.2–8.5) to 2.4 (95% CI, 1.7–3) in the NS group. Finally, the ODI scores improved from 34.1 (95% CI, 30–38.3) to 17.1 (95% CI, 15.3–19) in the DS group and it improved from 29.3 (95% CI, 24.2–34.4) to 18.4 (95% CI, 14.9–21.9) in the NS group. There were no significant differences between the two groups when comparing the respective preoperative back pain, leg pain, and ODI scores. Similarly, the differences between the postoperative scores were not statistically significant. The majority of patients in both groups rated their outcomes as excellent or good [Table 2].
| DS | P-value (pre vs. post-op) | NS | P-value (pre vs. post-op) | P-value (DS vs. NS) | |
|---|---|---|---|---|---|
| Post-op VAS score—back pain (SD) | 2.9 (0.8) | <0.05 | 2.8 (0.8) | <0.05 | 0.88 |
| Post-op VAS score—leg pain (SD) | 2.9 (1.0) | <0.05 | 2.4 (0.9) | <0.05 | 0.26 |
| Post-op ODI (SD) | 17.1 (2.2) | <0.05 | 18.4 (5.1) | <0.05 | 0.54 |
| MacNab Score | |||||
| Excellent | 2 | 4 | |||
| Good | 3 | 4 | |||
| Fair | 1 | 1 | |||
| Poor | 2 | 2 |
DS: Degenerative scoliosis, NS: No scoliosis, ODI: Oswestry disability index,
SD: Standard deviation, VAS: Visual analogue scale
Although no complications were encountered perioperatively, two of the patients in the DS group had a recurrence of their symptoms and underwent nerve root block.
DISCUSSION
Adult scoliosis is defined as a coronal plane deformity of the spine with a Cobb angle of more than 10° in a skeletally mature individual. It can be classified into three groups: Type 1 represents degenerative or de novo scoliosis.10 DS occurs in a previously straight spine and only after skeletal maturity. It results from asymmetrical degeneration of the functional spinal units, leading to uneven spine loading. This causes further asymmetrical degeneration and worsening of scoliosis, triggering a vicious cycle of progressive deformity.3 DS typically progresses at an average of 3° a year, and the risk factors for progression include curvatures of more than 30°, high-grade apical rotation, lateral listhesis of the apical vertebrae, and a high L5.11
Since degeneration increases with age, DS becomes increasingly more common in nations with longer life expectancies. Patients with DS report higher levels of pain compared to the general population. This can result in decreased quality of life for these patients with significant implications for the healthcare system.12 The two commonly encountered patterns of pain are back pain and radiculopathy. Up to 80% of the patients experience back pain due to spondylosis of the spine and muscle fatigue from spinal malalignment.4 However, the primary indication for surgery is lower limb radiculopathy resulting from foraminal stenosis. In patients with DS, spinal stenosis is found in 90% of symptomatic patients, and foraminal stenosis is more prevalent than central stenosis.5 Hence, TELF is ideal for addressing the foraminal stenosis and decompressing the exiting nerve in this group of patients.
Multiple surgical options for DS have been described in the literature. These range from decompression alone to multilevel fusions with correction of scoliosis. Decompression alone has been recommended for patients with curves less than 30° and without lateral subluxation. However, there are concerns about the destabilisation of the spine post-decompression surgery.5 TELF does not seem to cause iatrogenic instability as compared to open decompression surgery. Several studies examined the outcomes of TELF in patients with DS, and none of the authors reported stability-related complications. In addition, TELF has the advantage of lower anaesthetic risks, faster recovery, and lesser postoperative pain as compared to deformity correction surgeries.7–9
This is the first study comparing the outcomes of TELF in patients with DS and patients without deformity. We hypothesised that patients with DS will have poorer outcomes because the underlying pathology remains uncorrected. Whereas in patients without deformity, the foraminal stenosis is secondary to spondylotic changes with the facet and ligamentum flavum hypertrophy.13 Such pathology is typically amendable through foraminoplasty and is a common indication for TELF at our institute.
In both groups, patients had significant improvement in VAS and ODI scores postoperation. However, there was no significant difference in outcomes between the two groups at the end of the three-month follow-up. This lack of difference may be attributed to the short follow-up period of our study but in similar studies by Li et al.7 and Jin et al.9, their results approach the peak at three months with no differences at 12 months. In the landmark SPORT trial by Weinstein et al.,14 the improvement in clinical outcomes for the surgical group peaked at three months and was largely maintained at the end of two years. Therefore, our results may not change significantly with a short-term follow-up of two years. Nevertheless, this is a major limitation of our study as DS is likely to progress, and it remains to be determined if the patients in the DS group will require more surgery in the future or if their symptoms will recur. Hence, a mid-term follow-up of 60 months or even a long-term follow-up of 150 months may be required to detect the differences in outcomes between these two groups and to prove our hypothesis.15
Our results indicate that decompression alone significantly reduces back pain and radicular symptoms, which are the two most common presenting complaints among patients with DS. This result is in line with other authors’ studies that showed a similar reduction in back and leg pain postsurgery. We postulate that back pain in patients with DS is partly attributed to referred pain from foraminal stenosis with exiting nerve impingement. However, we do not advocate TELF in DS patients with back pain as their main complaint, but these patients can expect improvement in their back pain and be counselled accordingly.
This study showed that the short-term outcomes of TELF in patients with DS are comparable to those without deformity, and it may be a feasible option for patients who are unable or unwilling to undergo major deformity correction. Furthermore, patients in the DS group are older, with shorter life expectancy and lower functional demands. Hence, it may not be cost-effective to perform major deformity correction surgeries for this group of patients. We, therefore, recommend TELF as a palliative treatment option, given the encouraging short-term results. However, this is a small study, and more extensive trials may be necessary to demonstrate a difference in outcomes between the two groups.
Although there were no complications in both groups of patients, TELF is a technically challenging procedure in patients with deformities. Preoperative planning is critical to the success of TELF, and advanced imaging studies such as CT and MRI should be obtained before surgery for patients with DS. These imaging studies allow the surgeon to plan the optimal trajectory for the endoscope’s insertion and avoid critical structures such as nerve roots and the retroperitoneal space. In addition, these patients often present with extensive lumbar spondylosis and deformities that alter the normal anatomical landmarks. Hence, further imaging is useful in delineating the critical structures and pathology.
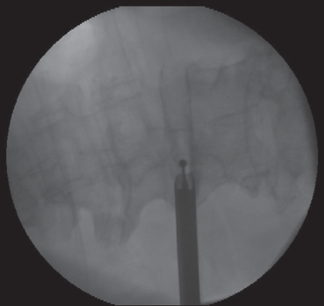
DS results in a considerable amount of osteophytes, and power burrs are often necessary to achieve adequate decompression of the foramen. This may lead to higher complication rates since the usage of power burrs has been associated with an increased risk of durotomies. Furthermore, during the usage of power burrs, turbulence, and bleeding affect the visual field, which increases the difficulty of the procedure.16 One of our senior authors recommends the usage of power burrs under fluoroscopic guidance [Figure 1] and completing the decompression under direct visualisation. Fluoroscopy reduces the reliance on visualisation and allows for better orientation during the burring.
In addition, the burring of bony structures often causes bleeding, leading to the disorientation of the surgeon. Hence, haemostasis is critical and can be achieved through the usage of haemostatic agents, radiofrequency coagulation, a temporary increase in water pressure, bone wax, and repositioning of the working cannula to tamponade the bleeding.
CONCLUSION
TELF is a well-described technique for treating lumbar foraminal stenosis, and previous studies have shown that it is effective for symptomatic relief in patients with DS. This study demonstrates the short-term clinical outcomes of TELF in patients with DS are comparable to those without. Patients are likely to experience improvements in back and leg pain after the procedure. Hence, we recommend it as a palliative treatment for patients who are unable to undergo deformity correction surgery.
Ethical approval
The research/study approved by the Institutional Review Board at Wooridul Spine Hospital, number 2023-03-WSH-004, dated 1st March 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Transforaminal endoscopic decompression for foraminal stenosis: Single-arm meta-analysis and systematic review. World Neurosurg. 2022;168:381-91.
- [CrossRef] [PubMed] [Google Scholar]
- The prevalence of adult de novo scoliosis: A systematic review and meta-analysis. Eur Spine J. 2020;29:2960-9.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical treatment of adult degenerative scoliosis. Asian Spine J. 2014;8:371-81.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive surgery in adult degenerative scoliosis: A systematic review and meta-analysis of decompression, anterior/lateral and posterior lumbar approaches. J Spine Surg. 2016;2:89-104.
- [Google Scholar]
- Comparison of percutaneous transforaminal endoscopic decompression and short-segment fusion in the treatment of elderly degenerative lumbar scoliosis with spinal stenosis. BMC Musculoskelet Disord. 2021;22:906.
- [CrossRef] [PubMed] [Google Scholar]
- Early experience with endoscopic foraminotomy in patients with moderate degenerative deformity. Neurosurg Focus. 2016;40:E6.
- [Google Scholar]
- Therapeutic strategy of percutaneous transforaminal endoscopic decompression for stenosis associated with adult degenerative scoliosis. Global Spine J. 2022;12:579-87.
- [Google Scholar]
- The prevalence and radiological findings in 1347 elderly patients with scoliosis. J Bone Joint Surg Br. 2010;92:980-3.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation of foraminal parameters with patient-reported outcomes in patient with degenerative lumbar foraminal stenosis. J Clin Med. 2023;12:479.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med. 2008;358:794-810.
- [Google Scholar]
- Follow-up definitions in clinical orthopaedic research: A systematic review. Bone Jt Open. 2021;2:344-50.
- [CrossRef] [PubMed] [Google Scholar]
- Difficulties, challenges, and the learning curve of avoiding complications in lumbar endoscopic spine surgery. Int J Spine Surg. 2021;15:S21-37.
- [CrossRef] [PubMed] [Google Scholar]




