
Translate this page into:
Comparison of the functional outcome of intramedullary nailing versus plating in displaced midclavicular fractures
Address for correspondence: Dr. Chandra Prakash Pal Department of Orthopaedics, SN Medical College, Agra, Uttar Pradesh, India. E-mail: drcportho@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Pal CP, Dinkar KS, Shakunt RK, Singh A, Hussain A, Sharma YK. Comparison of the functional outcome of intramedullary nailing versus plating in displaced midclavicular fractures. J Orthop Allied Sci 2018;6:13-6.
Abstract
AIMS:
The aim of this prospective study was to evaluate the effectiveness of intramedullary nailing and fixation by locking plates in displaced midclavicular fracture and to compare the functional outcome of intramedullary nailing versus plating.
MATERIALS AND METHODS:
This prospective comparative study was conducted at the tertiary center between October 2013 and September 2015 after being approved by the local Ethical Committee. A total of 66 patients ranging between 18 and 60 years of age were included in this study. They were randomized into two groups to be treated either by an intramedullary nail or by locking plate. Clinical and radiological assessments were performed at the 3rd week and 6th week and 3rd, 6th, and 12th month postoperatively. Outcomes and complications were compared to the 1-year follow-up in both groups.
RESULTS:
There was no significant difference found between two groups with regard to functional outcome after fracture union. Although lesser operative time, lower blood loss, less duration of hospital stay, easier implant removal, and better cosmetic appearance were noted in the nailing group. Constant shoulder scores were significantly higher in plating groups when compared to nailing group for the 1st 12 weeks of follow-up. However, this difference becomes insignificant between the two groups after 6 months of follow-up. Infection and revision surgery rates were more in plating group, but this difference is not significant.
CONCLUSIONS:
Functional outcome and complications remain same in intramedullary nailing and plating group. However, intramedullary nailing is advantageous concerning faster healing, secure implant removal, and better cosmetically appeared scars.
Keywords
Comparative study
midshaft clavicle fractures
nail
plate

Introduction
Fracture of clavicle accounts for approximately 3.2% of all the fractures and about 35% of all injuries of shoulder girdle.[1] About 80% of fractures involved the middle third region and about 50% are displaced. The mean age of patients sustaining clavicular fracture is about 33 years, and males are more commonly involved. Most common mechanism of injury is a fall or direct blow to shoulder, leading to axial compressive force.[2,3] Displaced midclavicular fractures were treated conservatively because early reports suggesting that nonunion fractures are very rare and malunion fractures are without any functional deficit and for radiographic interest only. Clavicle keeps upper limb away from torso for efficient function so work as “strut.”[4] However, recent studies concern about higher rates of delayed union, shoulder weakness, residual pain and deficits, and terminally affected movements associated with nonoperative treatment. Internal plate fixation and intramedullary nailing are essential operative techniques. Either technique provides superior functional results compared to the conventional method. In recently randomized studies results shows.maintaing the clavicular length in displaced mid clavicular fractures is very crucial for the best fuctional outcome of terminally affected movemnts.[5]
However, prospective randomized controlled trials (RCT) comparing these practical techniques for displaced midclavicular fractures were lacking.[6-8] The aim of this study was designed to examine the effectiveness of intramedullary nailing and fixation by locking plates in displaced midclavicular fractures and comparison of functional outcome and complications of two standard operative procedures.
Materials and Methods
This is a prospective comparative study done between October 2013 and September 2015, to study the functional outcome and complications of displaced midclavicular fracture treated either by intramedullary nailing or by internal locking plate fixation. A total of 100 unilateral displaced midclavicular fractures were admitted and 66 patients included in this study along with 1-year follow-up protocol. Intramedullary nailing included tense elastic nail and Rush pin used in 33 patients, whereas locking plates included anatomically precontoured locking plates and locking reconstruction plates used in rest 33 patients. Patients randomized into two groups by alternate (one by one) methods. Robinson classification treasured in choosing therapy as well as it is prognostically significant. Patients were followed monthly for the 1st 4 months and then 3 monthly. Assessment of shoulder function was carried out postoperatively clinically and radiologically.
The patient's pain profile was assessed using a visual analog scale; functional outcomes were evaluated using the constant shoulder score and range of motion (ROM) at shoulder joint: clinical assessment included ROM measurement using a goniometer – abduction, forward flexion, elevation, adduction, and internal and external rotation were measured on both sides. Only unilateral complete displaced mid-clavicular fractures in the age group between 18 and 60 years with <2 week old, mark shortening of <2 cm and angulation >30 degree includes in the study. Bilateral, undisplaced, compound, severe comminiation, multitrauma patient, previously operated, malunited and nonunion fractures, and pathological fractures along with neurovascular injuries were excluded from our study.
Results
A total of 66 patients were analyzed who completed at least 1 year of complete follow-up. As per inclusion criteria, we had 33 patients in the plate group [Figure 1] and 33 in the nail group [Figure 2] for comparison. In the plate group, we had 7 (21.2%) female patients, whereas there were 10 (30.03%) female patients in the nail group. Statistically, there was no significant difference between two groups on gender (P = 0.398). Mean age of patients in Group I (31.79 ± 11.05 years) was slightly higher as compared to that of patients in Group II (28.88 ± 7.89 years), but the difference between two groups was not statistically significant (P = 0.223). In both the groups, the majority had involvement of the right side. Left side was involved in 36.4% of Group I and 39.4% of Group II patients. Statistically, this difference did not account significantly (P = 0.800).
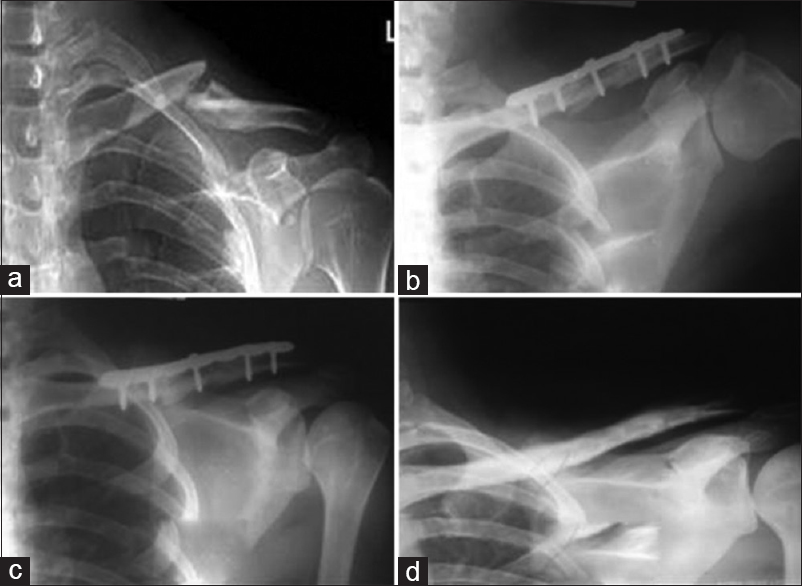
- Skiagrams of a left clavicle of a 20–year-old male patient showing (a) midshaft clavicle fracture, (b) immediate postoperative X-ray with plate in situ, (c) 3 months postoperative with fracture union, and (d) after implant removal
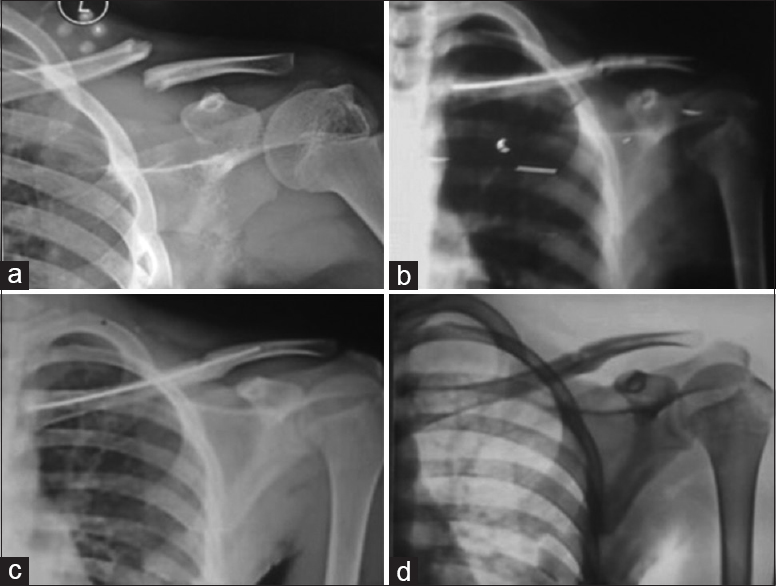
- Skiagrams of left clavicle of a 15–year-old male patient showing (a) clavicle fracture, (b) immediate postoperative X-ray with IM TEN in situ, (c) fracture united 3 months postoperatively, and (d) after implant removal
Mean injury time was 3.61 ± 3.28 days in Group I as compared to 3.64 ± 2.76 days in Group II. Statistically, this difference between two groups was not significant (P = 0.968). However, mean duration of hospital stay, as well as mean amount of blood loss, was higher in Group I (2.36 ± 1.03 days and 115.25 ± 30.54 ml) as compared to that in Group II (1.64 ± 0.78 days and 55.30 ± 16.77 ml), and this difference was statistically significant (P < 0.05). The mean length of incision was longer in Group I (10.35 ± 1.06 cm) as compared to that in Group II (4.38 ± 0.75 cm). For both these parameters, the difference between two groups was significant (P < 0.001). Mean pain score was higher in Group I (3.33 ± 1.47) as compared to that, in Group II (2.91 ± 1.42), yet this difference was not statistically significant (P = 0.238). Time taken for union ranged from 3 to 11 months with a mean value of 5.91 ± 1.89 months. Union time was slightly longer in Group I (6.00 ± 2.41 months) as compared to Group II (5.82 ± 1.89 months), but the difference between two groups was not statistically significant (P = 0.701).
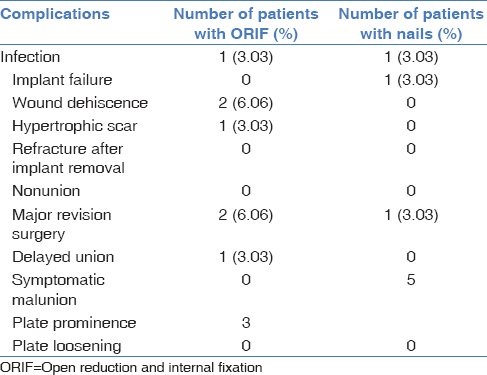
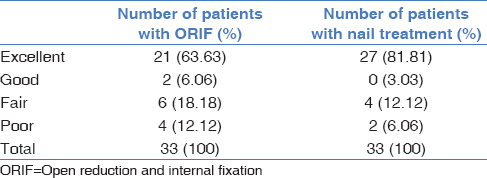
In plate group patients, one (3.03%) had hypertrophic skin scar, infection was found in one patient (3.03%), and major revision surgery was found in 2 (6.06%) patients. Nonunion and refracture after implant removal were not encountered in this group. In nail group, infection was found in 1 patient (3.03%), implant failure occurred in 1 patient (3.03%), and major revision surgery was found in 1 (3.03%) patient [Table 1]. The functional outcome was assessed by Constant and Murley score. In this study, out of 33 patients treated with plate and screws, 21 patients (63.33%) had excellent functional outcome, good functional outcome in 2 patients (6.06%), and fair functional outcome in 6 patients (18.18%). Among 33 patients receiving nail method, 27 patients (81.81%) had excellent functional outcome results, 4 patients (12.12%) had fair functional outcome, and 2 patients (6.06%) had poor functional outcome [Table 2].
Discussion
Traditionally, displaced midclavicular fractures had been managed nonoperatively.[9] NEER and ROWER found minuscule incidence of nonunion (0.1% and 0.8%, respectively) in their studies in 1960 and recommended conservative treatment for clavicular fractures.[6]
Recent studies have shown that higher nonunion rate in nonoperatively treated patients is approximately 5%. Recent studies also show poorer functional outcome in displaced midclavicular fractures that treated traditionally when compared to surgically treated patients. Furthermore, the best treatment for displaced midclavicular fractures remains unclear and becomes a topic of debate. However, the current recommendation for displaced midclavicular fracture treatment is by operative fixation. Many authors advocate plate fixation as a standard operative procedure for displaced midclavicular fractures.[4,7,10] Plate fixation choice included 3.5 mm dynamic compression plates and anatomically precontoured locking plates. Locking reconstruction plates applied either anterosuperiorly or anteroinferiorly and fixed by three screws on either side of the fracture. Recent emerging mode of fixation is intramedullary nailing fixation either by anterograde or by retrograde technique.[11] Biomechanically, nailing is weak regarding better rotation control of fragments during early movement of the shoulder and thus allows the primary union. Patients can be allowed full ROM as soon as soft-tissue healing occurs.[6,9] The disadvantage of plating includes damage to the supraclavicular nerve, slight higher infection rates, more soft-tissue stripping, and significant refracture after plates removal. The advantage of intramedullary nailing is less soft-tissue trauma and enhanced bone healing. The higher advantage of intramedullary nailing is ease in implant removal and lesser scar in cosmetically conscious patients.[12-14] In our study, constant shoulder scores were significantly higher in the plating group when compared to intramedullary nailing group during the 1st 12 weeks of the follow-up period. However, no significant difference of standardized shoulder scores was found between the two groups after 6 months of follow-up period. Fu et al.[15] compared nail and reconstruction plate fixation in displaced midclavicular fractures and found no significant difference in functional outcome after 18 months of follow-up evaluated using DASH score. Azar et al.[16] compared low-contact dynamic compression plates and Rockwood pin fixation in displaced midclavicular fractures and no significant difference found in functional outcome at 1 year of follow-up.
The limiting factor of our study is small sample size and study done at a single center. Longer RCT is needed at the various centers to evaluate the outcomes and complications further. What we can conclude from our study is that both intramedullary nailing and fixation by locking plate are equally alternative methods for treating displaced midclavicular fractures as for as functional outcome is concerned. Although from our study we recommended the use of minimally invasive anterograde intramedullary nailing in displaced midclavicular fractures in light of faster fracture union, easier plant removal and better cosmetic result in cosmetically conscious patients.
Conclusions
Intramedullary nailing for midclavicular displaced fracture is advantageous as compared with the clavicular platting as it provides fast healing, easy to remove, less cumbersome, and cosmetically good for patient.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Fracture clavicle and injuries around the shoulder. Essentials of Rehabilitation for Orthopaedic Surgeons. Ch. 6 2004:80-9. 10.5005/jp/books/10296_
- [CrossRef] [Google Scholar]
- Effect of different statistical methods on union or time to union in a published study about clavicular fractures. J Shoulder Elbow Surg. 2013;22:471-7.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of trauma victims admitted to a level 2 trauma center of North India. Int J Crit Illn Inj Sci. 2017;7:107-12.
- [CrossRef] [PubMed] [Google Scholar]
- Radiological and functional outcomes 2.7 years following conservatively treated completely displaced midshaft clavicle fractures. Arch Orthop Trauma Surg. 2015;136(1):17-25.
- [CrossRef] [PubMed] [Google Scholar]
- Elastic Intramedullary Nailing of Midclavicular Fractures. Acta Chir Belg. 2008;108(4):428-32.
- [CrossRef] [PubMed] [Google Scholar]
- The Washington Manual of Critical Care, Second Edition, by Martin Kollef and Warren Isakow. Published by Lippincott Williams & Wilkins, Philadelphia. Crit Care Med. 2013;41(4):e39.
- [CrossRef] [Google Scholar]
- Long-term functional outcome assessment of operative treatment for clavicular nonunion. Ir J Med Sci. 2002;171:63..
- [CrossRef] [Google Scholar]
- Long-term functional outcome assessment of plate fixation and autogenous bone grafting for clavicular non-union. Injury. 2004;35:575-9.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical versus conservative treatment in the management of displaced mid shaft clavicular fractures: A clinical study. J Appl Sci Res. 2012;3:343-6.
- [CrossRef] [Google Scholar]
- Rockwood and Green's fractures in adults. Eur J Orthop Surg Traumatol. 2011;22:631.
- [CrossRef] [Google Scholar]
- Bilateral fracture of the medial clavicles treated by open reduction and internal fixation using angle stable locking T-plates. Injury Extra. 2008;39:276-8.
- [CrossRef] [Google Scholar]
- Intramedullary bone formation after intramedullary nailing. J Orthop Trauma. 2009;23:288-93.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary Nailing of the Clavicle. In: Rommens P., Hessmann M., eds. Intramedullary Nailing. London: Springer; 2015. p. :105-15.
- [CrossRef] [Google Scholar]
- Orthopedic Traumatology: An Evidence-Based Approach. Pringer Science & Business Media; 2012:454.
- [Google Scholar]
- Anatomical reduction for treatment of displaced midshaft clavicular fractures: Knowles pinning vs. Reconstruction plating. Orthopedics. 2012;35:e23-30.
- [CrossRef] [Google Scholar]




