
Cardiac stroke following total knee replacement in an ochronotic arthropathy: Case report and literature review
Address for correspondence: Dr. Saurabh Jain, MGM Medical College and MY Hospital, Indore, Madhya Pradesh, India. E-mail: jaindrsaurabh@yahoo.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Jain S, Puri R, Reddy S. Cardiac stroke following total knee replacement in an ochronotic arthropathy: Case report and literature review. J Orthop Allied Sci 2016;4:75-9.
Abstract
Alkaptonuria is a rare autosomal recessive disorder caused by defective metabolism of homogentisic acid (HGA) which on accumulation in the connective tissues causes arthritis, darkening of urine and connective tissue pigmentation. Knee is most commonly affected joint whereas pigment deposition is seen in entire body causing cardiovascular, genitourinary, ocular, cutaneous, and musculoskeletal complications. We here report such a case of bilateral ochronotic arthropathy, who was diagnosed to be alkaptonuric only during joint exploration. He sustained a cardiac catastrophic stroke on 3rd post operative day of the left knee replacement which was done one week after the right knee replacement. With prompt treatment and good hospital care, the patient was revived successfully, without valvulotomy or valvular replacement. The spectrum of clinical manifestations are discussed in the report with emphasis on thorough history and clinical examination of the patient, before taking the patient to the total knee replacement to make accurate diagnosis before hand and be prepared for the complications or catastrophic by a multidisciplinary approach.
Keywords
Alkaptonuria
ochronosis arthropathy
homogentisic aciduria

Introduction
Alkaptonuria is a rare autosomal recessive disorder, affecting only one in 1 million individuals, which is caused by defective metabolism of homogentisic acid (HGA) which accumulates and is deposited in the connective tissues.[1,2,3,4] The common clinical features are arthritis, darkening of urine with exposure to air or reducing agents, and connective tissue pigmentation.[3,4,5] We report a case of bilateral ochronotic arthritic, who was only diagnosed to be alkaptonuric during knee replacement and was successfully revived after the cardiac catastrophic event occurring 3rd postoperative day of the left knee replacement which was done 1 week after the right knee replacement. The report emphasis on thorough history and clinical examination of the patient, before taking the patient to the total knee replacement to make accurate diagnosis beforehand and be prepared for the complications or catastrophic by a multidisciplinary approach.
Case Report
A 64-year-old male presented to the Department of Orthopedics with a history of pain in both knee joints for the past 10 years. On detailed history, pain was insidious in onset, localized to both knees but more on the medial aspect, nonradiating, initially mild, but for the past 2 years, the pain intensity has aggravated from moderate to severe in nature. Although the patient denied pain that interfered with sleep, he had rest pain as well. Pain was associated with mild swelling in both knee and difficulty in walking up as well as downstairs with ability to walk around 2-3 blocks only. He was initially treated by rest, analgesics, nonsteroidal anti-inflammatory drugs and physiotherapy which subsided his symptoms temporarily, without sustained improvement. He also gives history of occasional dull back pain and stiffness of spine.
His gait was stable secure with antalgic component. Examination showed mild swelling, with tenderness over the medial and lateral knee joint line with varus alignment of the both knees of around 15° each. Patellofemoral arthritis was also present as seen by positive patellar grinding test. Coarse crepitations were present in both knees. There was no laxity of the collateral or cruciate ligaments. Range of motion in right knee was 15-90° and in left knee was 10-100°. Preoperative knee scores were 41 and 47 for right and left knees, respectively, and functional score was 45 in both knees as per knee society score.[6] Distal neurovascular examinations of the lower extremities were intact and symmetric. Both hips did not reveal much except terminal restriction of movements. His lumbar spine showed mild stiffness and tenderness. Upper limbs did not reveal any symptoms. The respiratory, neurological, and abdominal examinations were normal. Thus, patient's medical history, symptomatology, and examination were typical for progressive degenerative arthritis affecting both knees.
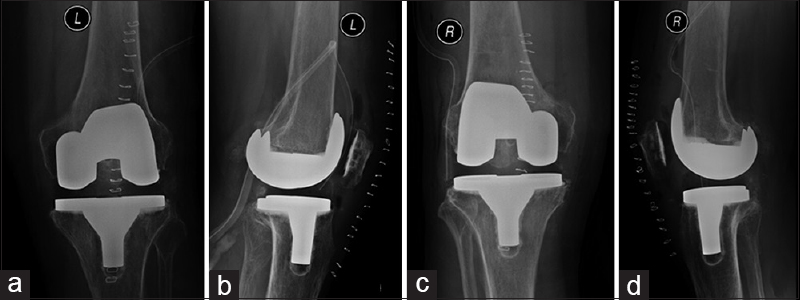
Radiographic evaluation of the both knee joints revealed advanced degenerative arthritis, with significant loss of joint space, subchondral sclerosis, and excessive osteophytosis. Both medial and lateral compartments were involved along with patellofemoral degenerative changes [Figure 1]. Other laboratory analyses including complete blood count, erythrocyte sedimentation rate, C-reactive protein, liver, kidney and thyroid function tests, calcium, phosphate, magnesium, parathyroid hormone, 25-OH Vitamin D, Vitamin B12, folate, and ferritin, as well as urinalysis, were within normal ranges. Rheumatoid factor and HLA-B27 were negative. His electrocardiogram and echocardiograph demonstrated sinus rhythm at 75 beats/min mild aortic stenosis with left ventricle hypertrophy but functioning well (ejection fraction 60%).

- Preoperative anteroposterior (a and b) and lateral (c and d) X-rays of the left right and left knee respectively of the patient showing typical features of advance degenerative arthritis, with significant loss of joint space, subchondral sclerosis and excessive osteophytosis along with patellofemoral changes with varus alignment
After medical and anesthetic fitness for total knee replacement, the patient was planned for cemented total knee replacement. Both knees were replaced in staged manner within a period of 1 week, right operated first followed by left. Until the surgery was done, we did not know that he was alkaptonuric. Both knees were operated with midline incisions and medial parapatellar arthrotomies under tourniquet. The ligaments, joint capsule, and synovium in both knees were having brownish-black discoloration. A deposition of black pigment was seen throughout the articular cartilage [Figure 2]. The menisci were degenerated, brittle, with large areas of black pigmentation. The collateral and cruciate ligaments were intact in both knees but with reduced bulk. There was no difficulty with the soft tissue balancing and implantation in knees. Histological sections of removed bone and soft tissue demonstrated classic findings of ochronosis, including multiple pigment-laden tissues, reactive giant cells, and thickened, inflamed synovium.
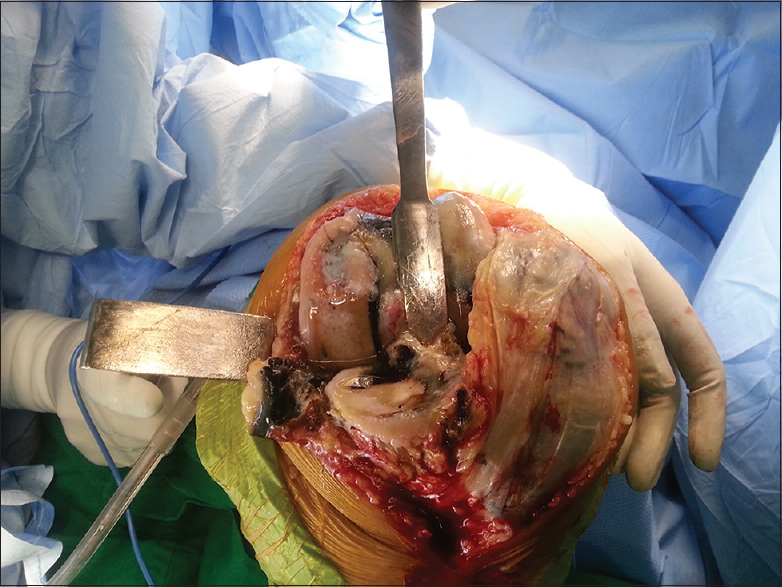
- Intraoperative clinical photograph of the right knee joint showing brownish-black discoloration in ligaments, capsule, synovium, and meniscus
Postoperatively, on suspecting it to be alkaptonuria, when we took specific history for ochronosis, the patient revealed that his urine turned black in sunlight. Nontender mild bluish-brown pigmentation was also seen in the sclera of the eyes, base of pinna and axilla, which was only appreciated, after thorough proper examination and high index for suspicion for alkaptonuria after the right knee was replaced [Figure 3]. The patient denied knowing about any other family members who may have noticed dark urine or experienced painful joints. Thus, finally, the diagnosis of alkaptonuria was made retrospectively. As the patient recovered well after the right knee replacement, the left knee was also replaced similarly after 1 week, with advantage of knowing the intraoperative finding earlier. Similar finding was seen in left knee as well.
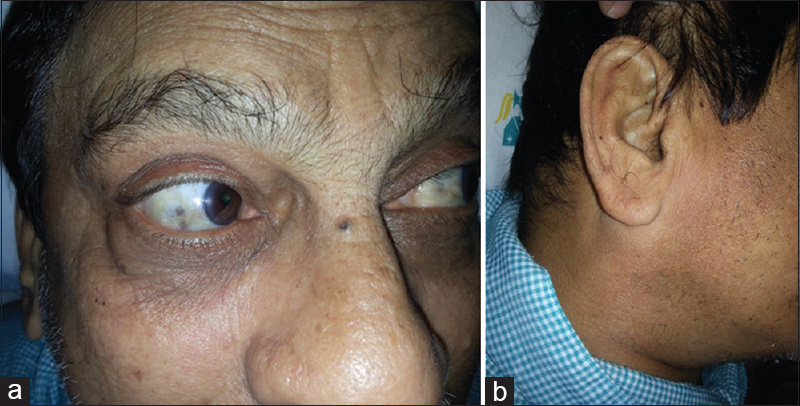
- Clinical photograph of patient showing mild bluish-brown pigmentation in sclera (a) and base of pinna (b), which was appreciated only after thorough proper examination and high index for suspicion for alkaptonuria
Although the surgeries were uneventful, in the postoperative period, i.e., on 3rd day postoperative of left knee replacement, patient sustained a cardiac stroke. Angiography was performed which showed coronary artery disease with calcified aortic valvular stenosis with a peak transvalvular gradient of 90 mm Hg. With prompt treatment and good hospital care, the patient was revived successfully without valvulotomy or valvular replacement.
Both knee joints were stable after surgery. Postoperative pain relief was excellent in the operated joints. There were no wound healing problems. Postoperative recovery period and rehabilitation protocol were similar to all other patients who underwent joint replacement. The patient progressed well, regaining good range of motion and independent ambulation 6 weeks after surgery. Postoperatively, radiograph revealed a valgus alignment of 5° in right and 4° in left lower limbs for the knees with total knee components in good position and alignment [Figure 4]. Knee scores improved significantly, 93 for right and 94 for left knee at 1 year follow-up. Functional score was about 85 in both knees. Range of motion in the right knee was 0-115° and in the left knee was 0-120°. At 1 year following surgery, the patient had returned to full activities, described no knee pain, and was very satisfied with the outcome.
- Postoperative anteroposterior (a and c) and lateral (b and d) X-rays of the left right and left knee revealing valgus alignment in both the knees with total knee components in good position and alignment, respectively
Discussion
During the metabolism of the amino acids tyrosine and phenylalanine, enzyme homogentisate 1,2-dioxygenase (HGO) breaks down intermediate product, HGA to maleylacetoacetic acid.[1,2,3,4,5] Alkaptonuria is caused by mutations in this HGO gene on chromosome 3q causing deficiency in homogentisate 1,2-dioxygenase activity, thus leading to accumulation of HGA.[7,8] Accumulated HGA and its product of oxidation, benzoquinone on polymerization forms blue-black colored pigment (ochronotic pigment) which is, thus, deposited in connective tissues and organs, binding irreversibly to collagen giving typical triad of ochronosis, i.e., homogentisic aciduria, ochronotic pigmentation, and degenerative arthritis.[3,4,5]
The only manifestation seen at birth and early childhood is dark-colored urine, due to large quantity of HGA in urine, a pathognomonic sign for alkaptonuria.[8,9,10,11,12] Same was seen in our case also although the patient concealed history of dark-colored urination since childhood.
Other clinical manifestations of alkaptonuria are observed only after the fourth decade because with aging the renal clearance of HGA decreases, leading to its deposition in tissues.[8,9,10,11,12] Deposition may affects the entire body, but mainly in skin, bones, joints, lungs, endocardium and valves, and kidneys causing cardiovascular, genitourinary, ocular, cutaneous, and musculoskeletal complications.[1,2,3,4,5,7,8,9,10,11,12] Features include disc narrowing, calcifications and herniation, porotic vertebral bodies, and osteophyte formation;[13,14] aortic and cardiac valve calcification and stenosis, coronary artery calcifications;[15,16] renal, urethral, and prostatic stones;[7,8] and pigmentation of face, hands, fingernails, sclera, and ear cartilage.[1,2,3,4,5,17] There are reports of ruptures of patellar and achilles tendons, due to heavy pigmentation binding with high collagen content, leading to inflammation, calcification, and ruptures.[5,18,19,20] An asymptomatic small left renal calculus was also documented in our patient. Our patient also had aortic stenosis and left ventricle hypertrophy but well-functioning heart (ejection fraction 60%). Although on the 3rd day of second knee replacement, he sustained a cardiac stroke, which on angiography showed coronary artery disease with calcified aortic valvular stenosis, we were able to successfully revive the patient with prompt treatment, without valvulotomy or valvular replacement, which may sometimes be needed for such type of patients. To prevent such catastrophic event, we recommend complete work up of the patient and be prepared for the prompt treatment if it occurs.
Progressive arthropathy of the large weight bearing joints particularly knee, followed by the hip and shoulder, is the most common clinical feature of ochronosis, appearing after the fourth decade.[1,2,3,4,5,21,22] The polymerized, deposited HGA discolors and weakens the connective tissue and cartilage, which is easily disrupted, fragmented, creates loose shards and finally leads to chronic inflammation, joint space narrowing, sclerosis and eventually osteoarthritis, which stimulates other osteoarthritic pattern with a small inflammatory component due to synovial irritation.[23] Although the smaller joints do not appear to develop arthritis, the cartilage within these joints also demonstrates pigmentation.[2] These changes are seen in the bones as well but are less severe than those in cartilage due to calcification and bone remodeling.[24] There have been case reports of ribs being affected and bone fractures.[25,26]
Spectrum of clinical variability may delay the diagnosis. Diagnostic confirmation of alkaptonuria is made by alkalinization of urine. Confirmatory tests for diagnosis are chromatographic, enzymatic, or spectrophotometric or quantitative determination of HGA in urine.[4] Ochronotic arthropathy may be diagnosed intraoperatively, on finding a blackened joint, as in our case, the diagnosis of ochronosis was not made until exploration of the joint. Long-term use of levodopa, methyldopa, antimalarials, or products containing hydroquinone, phenol, resorcinol, mercury, or picric acid may give rise to pseudo-ochronosis.[27] Coexistence of ochronosis with rheumatoid arthritis,[28] ankylosing spondylitis,[29] or chondrocalcinosis[30] has also been reported. Our patient lacked rheumatoid factor and the HLA-B27 antigen.
Currently, there is no specific or effective treatment for ochronosis.[1,2,3,4,5,7,8,9,10,11,12] General accepted approach is symptomatic treatment, which includes treatment of pain, physiotherapy, chiropractic care, adequate anti-osteoporotic therapy, education of the patient for a home exercise program, and dietary protein restriction of phenylalanine and tyrosine which had to be continued lifelong to prevent further disability.[1,2,3,4,5,7,8,9,10,11,12] High-dose Vitamin C decreases urinary benzoquinone acetic acid but has no effect on HGA excretion, and clinical studies have not shown its effectiveness.[31,32] Nitisinone, a potent inhibitor of 4-hydroxyphenylpyruvate dioxygenase, which catalyzes the formation of HGA from hydroxyphenylpyruvic acid, reduces production and urinary excretion of HGA, but role of nitisinone in treating ochronosis remains unknown.[1,2,3,4,5]
Total joint replacement of the hips, knees, elbows, and shoulders for significant degenerative arthritis for alleviation of pain and increases in activity is well accepted. However, there are very few reports published on outcome comparison, cemented versus uncemented or unilateral or bilateral replacement, and these reports lack uniformity. Reports on total joint replacement have shown equally good results, comparable to osteoarthritic patients without ochronosis.[1,2,3,4,5] There is no safe information in the literature about the type of the prosthesis but both cemented as shown by Fisher and Davis[3] and uncemented as shown by Konttinen et al.,[33] Aydogdu et al.[34] have shown excellent outcomes. To prevent acceleration of the osteoarthritis in contralateral knee due to load asymmetry and better dynamic balance, bilateral replacement is favored in the literature.[35]
To conclude, surgeons should be aware that alkaptonuria had multiple system involvement, with wide spectrum of clinical presentation. A proper history and through examination, before surgery can help in making accurate diagnosis early and appropriate treatment of complications, which may significantly improve the quality of life in these patients. Advances in orthopedic and cardiac surgery have enabled patients to overcome progressive disability. Understanding the genetic and molecular basis of alkaptonuria has the potential to offer a new therapeutic approach, enzyme replacement therapy with recombinant HGO.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Total knee arthroplasty in ochronosis: A case report and critical review of the literature. Eklem Hastalik Cerrahisi. 2013;24:169-72.
- [CrossRef] [PubMed] [Google Scholar]
- Degenerative arthritis of the knee secondary to ochronosis: A case report. Bull NYU Hosp Jt Dis. 2011;69:331-4.
- [Google Scholar]
- Alkaptonuric ochronosis with aortic valve and joint replacements and femoral fracture: A case report and literature review. Clin Med Res. 2004;2:209-15.
- [CrossRef] [PubMed] [Google Scholar]
- Patellar ligament rupture during total knee arthroplasty in an ochronotic patient. Acta Orthop Traumatol Turc. 2014;48:367-70.
- [CrossRef] [PubMed] [Google Scholar]
- Rationale of the knee society clinical rating system. Clin Orthop Relat Res. 1989;248:13-4.
- [CrossRef] [Google Scholar]
- New developments in ochronosis: Review of the literature. Rheumatol Int. 2005;25:81-5.
- [CrossRef] [PubMed] [Google Scholar]
- Ochronotic arthropathy: Case report and review of the literature. Int Orthop. 1999;23:122-5.
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral hip arthroplasty for ochronotic arthropathy. Clin Rheumatol. 2000;19:150-2.
- [CrossRef] [PubMed] [Google Scholar]
- The pathology of alkaptonuric ochronosis. Hum Pathol. 1989;20:40-6.
- [CrossRef] [PubMed] [Google Scholar]
Erratum in: Hum Pathol. 1989;20:500. - Alkaptonuria and ochronosis: Case report and review. J Am Acad Dermatol. 1992;27:609-14.
- [CrossRef] [PubMed] [Google Scholar]
- Alkaptonuria and lumbar disc herniation. Report of three cases. J Neurosurg. 2003;98(1 Suppl):87-9.
- [CrossRef] [PubMed] [Google Scholar]
- Alcaptonuria with lumbar disc prolapse: Case study and review of the literature. Spine J. 2007;7:495-8.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular findings in alkaptonuric ochronosis. Am Heart J. 1990;120(6 Pt 1):1460-3.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular ochronosis: A case report and review of the medical literature. Cardiology. 1990;77:477-83.
- [CrossRef] [PubMed] [Google Scholar]
- Hereditary ochronosis: Hyperpigmented skin overlying cartilaginous structures. Cutis. 1999;63:337-8.
- [Google Scholar]
- Bilateral spontaneous rupture of the quadriceps tendon as an initial presentation of alkaptonuria - A case report. Knee. 2006;13:408-10.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous tendon ruptures in alkaptonuria. J Bone Joint Surg Br. 2003;85:883-6.
- [CrossRef] [Google Scholar]
- Bilateral achilles tendon ruptures in a patient with ochronosis: A case report. Clin Orthop Relat Res. 2004;424:180-2.
- [CrossRef] [PubMed] [Google Scholar]
- Endogenous ochronosis: Case report and a systematic review of the literature. Int J Dermatol. 2011;50:262-7.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroplasty for ochronotic arthritis: No failure of 11 replacements in 3 patients followed 6-12 years. Acta Orthop Scand. 2004;75:355-8.
- [CrossRef] [PubMed] [Google Scholar]
- Chronic ochronotic arthritis: Clinical, arthroscopic, and pathologic findings. J Rheumatol. 2000;27:2272-4.
- [Google Scholar]
- A morphological study of bone and articular cartilage in ochronosis. Virchows Arch. 2000;436:74-81.
- [CrossRef] [PubMed] [Google Scholar]
- Medial femoral neck fracture in ochronotic alkaptonuria. Zentralbl Chir. 1969;94:806-10.
- [Google Scholar]
- A rare case of high dorsal radicular-medullary compression in a patient with ochronotic arthropathy. Clinico-radiological features. Minerva Med. 1995;86:61-6.
- [Google Scholar]
- Exogenous ochronosis. An update on clinical features, causative agents and treatment options. Am J Clin Dermatol. 2001;2:213-7.
- [CrossRef] [PubMed] [Google Scholar]
- Coexistence of ochronosis and rheumatoid arthritis. Clin Rheumatol. 1994;13:135-8.
- [CrossRef] [PubMed] [Google Scholar]
- The coexistence of ochronosis and ankylosing spondylitis. J Rheumatol. 1991;18:1639-40.
- [Google Scholar]
- A case report: Ochronosis in combination with chondrocalcinosis. Z Orthop Ihre Grenzgeb. 1999;137:76-8.
- [Google Scholar]
- Reversal of clinical symptoms and radiographic abnormalities with protein restriction and ascorbic acid in alkaptonuria. Ann Clin Biochem. 2003;40(Pt 1):108-11.
- [CrossRef] [PubMed] [Google Scholar]
- Alkaptonuria and ochronosis in three siblings. Ascorbic acid treatment monitored by urinary HGA excretion. Clin Exp Rheumatol. 1988;6:289-92.
- [Google Scholar]
- Ochronosis: A report of a case and a review of literature. Clin Exp Rheumatol. 1989;7:435-44.
- [Google Scholar]
- Cementless total knee arthroplasty in ochronotic arthropathy: A case report with a 4-year follow-up. J Arthroplasty. 2000;15:539-43.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of static and dynamic balance in patients with unilateral and bilateral total knee arthroplasty. Eklem Hastalik Cerrahisi. 2009;20:93-101.
- [Google Scholar]




