
Translate this page into:
Bone mineral density measurement in traumatic distal end radius fractures: A case–control study
Address for correspondence: Dr. Ankur Dilip Kariya, Quarter Number 6, Vivekanada Colony, Type 3, Dean Office Campus, MGIMS, Sewagram, Maharashtra, India. E-mail: ankurkariyaorth@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kariya AD, Jain PA, Patond KR. Bone mineral density measurement in traumatic distal end radius fractures: A case-control study. J Orthop Spine 2020;8:16-21.
Abstract
INTRODUCTION:
Osteoporosis is a global problem affecting over 200 million people worldwide. After a first osteoporotic fracture, there is an increased risk of a second fracture. Around 20% of patients experience a second fracture within 1 year of the first fracture. Early diagnosis of osteoporosis and its treatment after a fragility fracture are, therefore, very important interventions that can help in reducing the socioeconomic burden of osteoporosis. In this article, we present a case–control study of bone mineral density (BMD) in 100 cases of distal end radius fractures and matched controls.
MATERIALS AND METHODS:
One hundred patients with distal end radius fracture and 100 age- and sex-matched controls were selected based on predetermined selection criteria. All selected individuals were investigated for serum calcium, Vitamin D, and alkaline phosphatase. BMD was measured at calcaneum and distal radius. Data analysis was done to determine the strength of association between various parameters and BMD in cases and controls.
RESULTS:
The prevalence of osteoporosis was higher in age >45 years (35%) as compared to age <45 years (8%). Osteoporosis was higher in females (65%) with Distal end radius fractures (DER) fractures compared to males (33%). There was a significant association between serum Vitamin D, alkaline phosphatase, and BMD. The presence of DER fracture (39%) had a significant association with osteoporosis as compared to controls (17%).
CONCLUSION:
There is a significant association between increasing age, female sex, Vitamin D deficiency, high alkaline phosphatase, presence of DER fracture, and osteoporosis.
Keywords
Bone mineral density
distal end radius fracture
osteoporosis
Vitamin D

Introduction
Osteoporosis means a skeletal metabolic disorder which is characterized by low bone mass, deterioration of bone tissue and disruption of bone architecture, compromised bone strength, and an increase in the risk of fracture.[1] It is estimated to affect one in three women and one in eight men over the age of 50 years. Currently, it is estimated that over 200 million people worldwide suffer from this disease.[2] In India, even by modest estimates, in the population above 50 years, 20% of women and about 10–15% of men would be osteoporotic. Every fifth woman by the age of 80 years and 50% of women by the age of 90 years suffer a hip fracture.[3] After a first osteoporotic fracture, there is an increased risk of a second fracture, and around 20% of patients experience a second fracture within 1 year of the first fracture.[3]
Osteoporosis is a silent disease that goes unnoticed unless complicated by a fracture. This fracture generally occurs following a trivial trauma, and the severity of the trauma itself is not sufficient to explain the fracture. These fractures are called fragility fractures. These fragility fractures occur at various sites that include hip, spine, distal radius, and proximal humerus.[4] A DER fracture associated with minor trauma is indicative of an overall 50% increase in the risk of a subsequent hip fracture.[3] In the year following a distal radius fracture, studies have shown 5 and 10 times greater rates of vertebral fractures in women and men, respectively, in accordance with a 60% increase in the rates of hip fractures for women over 70 years.[5] Secondary prevention of a subsequent fragility fracture in a patient with DER fractures is very important considering the morbidity and mortality associated with fractures of the hip. Early diagnosis of osteoporosis and its treatment and secondary prevention of fragility fracture after a first fragility fracture are, therefore, very important interventions that can go a long way in reducing the socioeconomic burden of osteoporosis.
Materials and Methods
The present study was a case–control study conducted at a tertiary hospital over a period of 2 years. All patients sustaining distal end radius fractures and fulfilling inclusion and exclusion criteria were included in the study.
A total of 100 patients diagnosed with DER fractures were enrolled in the study as cases. The inclusion criteria were controls with the same sex and age (±2 years). One hundred controls were selected. The inclusion criterion for cases with DER fracture was age above 20 years. The exclusion criteria were presence of congenital anomalies of hand and foot, previous history of fracture of distal end radius on either side and history of fracture of calcaneus on nondominant side, pregnant women, cases of polytrauma or multiple fractures indicating high-velocity trauma, and cases with pathological fracture of distal end radius were excluded from the study, those consuming drugs that are implicated in causation of osteoporosis, having systemic disorders that are associated with osteoporosis.
Prior written informed consent was obtained from participants. A predesigned questionnaire was used for data collection. Information was collected on basic sociodemographic factors and biochemical parameters, namely serum Vitamin D, serum calcium, alkaline phosphatase, and bone mineral density (BMD) at distal radius and calcaneum.
Serum calcium estimation was done using random access analyzer (EM 360/XL 300). The normal reference value for serum calcium values was 9–11 mg/dl. Serum Vitamin D estimation was done by Thyrocare, Advia centaur machine which works on chemiluminescent immunoassay principle and measures total 25(OH) Vitamin D. The US Endocrine Society guideline was used to classify serum Vitamin D as normal (more than 30 ng/ml), insufficiency (20 ng/ml to 30 ng/ml), and deficiency (<20 ng/ml).
Serum alkaline phosphatase (ALP) estimation was done by random access analyzer, EM 360/XL 300 by the principle of photometry. The normal reference range of ALP is 60–170 IU/L.
Peripheral BMD (T score and Z score) was measured by Osteosys EXA-3000 bone densitometer which uses a digital radio beam scanner at two sites: calcaneum and distal radius. According to Min et al., there was a significant difference in the BMD T-scores between dominant and nondominant calcanea in 1794 healthy controls. The calcaneal BMD on the dominant side was found to be significantly higher. There was no significant difference in BMD of dominant and nondominant distal radiuses.[6] Hence, we measured BMD on the nondominant side in calcaneum in both cases and controls to prevent the underdiagnosis of osteoporosis. The BMD of left-side calcaneum was measured in a right-handed person and vice versa. Distal radius BMD was measured in cases from the normal side, whereas that of controls was taken from the nondominant side.
Results
A total of 100 patients with distal end radius fractures were taken up as cases for the purpose of the study and 100 age- and sex-matched controls were taken. Table 1 compares the demographic, biochemical parameters and BMD between cases and controls.
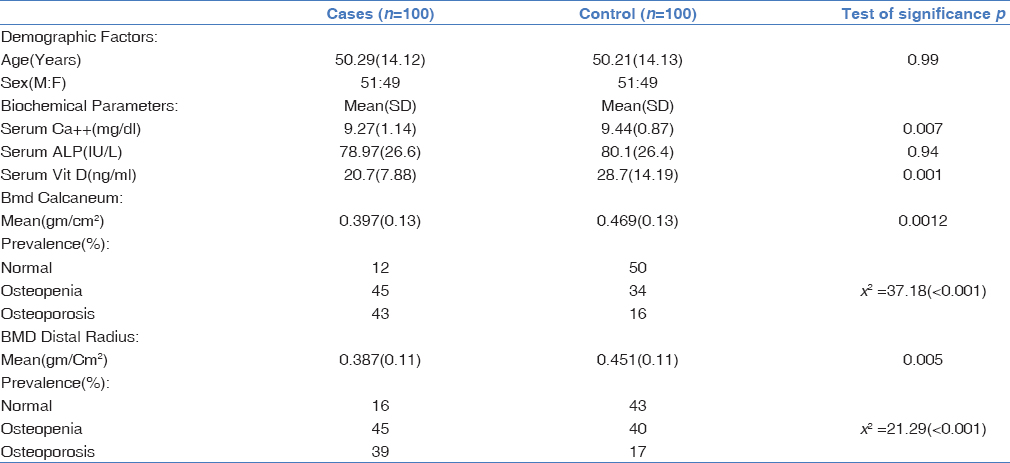
For the purpose of the study, we divided cases into two age groups. In the age group of <45 years, the mean BMD at both calcaneum and distal radius was lower in cases as compared to their controls, and the difference was statistically significant in both males and females as shown in Table 2.

The mean age in the study was found to be 50.29 years. Of the 100 patients with DER fractures, 38 were ≤45 years, whereas 62 were >45 years. The male: female ratio in our study was 51:49. However, in the age group of >45 years, the male: female ratio was 24:38, and in the age group of ≤45 years, it was 27:11. In the age group of ≤45 years, the prevalence of osteoporosis was significantly higher in cases and controls for both males and females. In the age group of >45 years, the prevalence of osteoporosis was significantly higher in both males and females.
The mean BMD of cases in all the four groups, i.e., ≤45 years' males, ≤45 years' females as well as ≥46 years' males and females was significantly lower than the mean BMD of controls at both sites – distal radius and calcaneum.
In the age group of ≤45 years, 65.78% of the patients had osteopenia and 21.05% had osteoporosis. In the age group of ≥46 years, 33.8% of the patients had osteopenia and 56.45% had osteoporosis. BMD of cases decreased with an increase in age, and this association was statistically significant.
In our study, female sex was strongly associated with the prevalence of osteoporosis. Even in younger age group, females had lower mean BMD (0.393 g/cm2) compared to their normal counterparts (0.438 g/cm2), which was statistically significant (t = 2.3, P = 0.03, 95% confidence interval [CI]).
Of 39 patients of DER fracture with osteoporosis, 13 (33.3%) had hypocalcemia, whereas of 17 controls with osteoporosis, 5 (29.41%) had hypocalcemia. Odds ratio (OR) was found to be 1.1 (0.6–1.1), which was not statistically significant.
The mean value of serum ALP was 78.97 IU/L, whereas in age- and sex-matched controls, it was 80.10 IU/L. Of 39 cases with osteoporosis, 8 had normal serum ALP (20.51%). Of 17 controls with osteoporosis, only 3 (17.64%) had low serum ALP. OR was found to be 1.02 (0.82–1.2), which was found to be statistically insignificant.
Of 39 cases with osteoporosis, 24 (61.5%) had Vitamin D deficiency, whereas 4 (23.5%) of 17 controls with osteoporosis had Vitamin D deficiency. OR for cases and controls for relation between Vitamin D and osteoporosis was calculated to be 1.8 (1.2–3.6), which was found to be statistically significant. Fifty percent of the patients with DER fractures (mean: 20.7 ng/ml) had Vitamin D deficiency as compared to 24% of the controls (mean: 28.7 ng/ml).
Figures 1 and 2 depict the relationship between the BMD of cases and controls. There is a statistically significant negative association between age and BMD. The osteoporosis in females is significantly lower t- or Z-scores than males in both case and control groups.
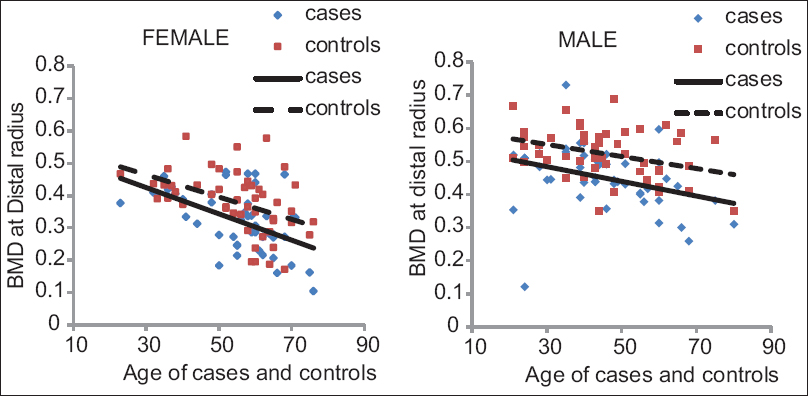
- Linear regression depicting negative association between age and bone mineral density at distal radius in cases and controls
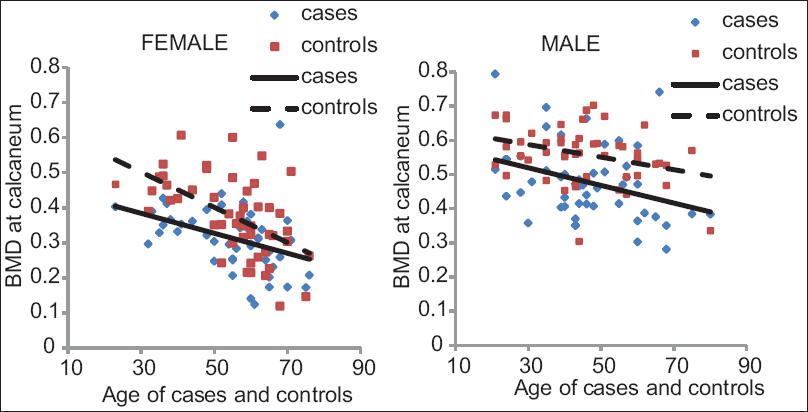
- Linear regression depicting negative association between age and bone mineral density at calcaneum in cases and controls
Linear regression for BMD at the radius and calcaneum among cases was found to be negatively correlated with age and sex as shown in Figures 1 and 2 and was statistically significant (P < 0.05).
Discussion
The present study highlights the significance of osteoporosis and its involvement in distal end radius fractures. In this study, a comparison of the T-scores of 100 patients with fracture of distal end radius with 100 age- and sex-matched controls was done, which was measured BMD T-scores using peripheral dual-energy x-ray absorptiometry (pDEXA) at 2 sites: distal radius and calcaneum. The comparison of other parameters such as serum Ca++, ALP, and Vitamin D between the cases and controls was also done.
Age is one of the most important risk factors for osteoporosis. The mean age for cases was 50.29 (±14.09) years, of which majority (28.0%) of the participants were between the age groups of 51 and 60 years. Mallmin et al.[7] in a study among 74 cases and 74 controls recorded a mean age of 66 ± 11 years. Similarly, Wigderowitz et al.[8] (2003) observed a mean age of 65.3 ± 10.6 years among males and 67.8 ± 10.5 years which is slightly higher as compared to the present study. The difference may be due to the selection process in both the studies. The selected cases in these studies were more than 45 years, Whereas, in this study, only cases over 20 years of age were included. However, we found the mean age 59.8 years (±8.4) in the age group of 45 years and above which is similar to their studies.
Mallmin et al.[7] demonstrated an inverse relationship between bone mass and age at both measuring sites. Similarly, in our study, we identified an inverse relationship between age and BMD at calcaneum as well as distal radius, which was statistically significant.
In the present study, of 100 patients with distal end radius fractures, 51 were male and 49 were female. Sixteen of 51 (31.3%) males had osteoporosis, whereas 23 of 49 females (46.9%) had osteoporosis. Only 5 of 51 (9.80%) male controls had osteoporosis, whereas 12 of 49 (24.48%) female controls had osteoporosis. We found OR = 1.2 (CI: 1.1–1.4) at distal radius and OR = 1.3 (CI 1.1–1.6) at calcaneum BMD for age-matched cases and controls, which was significant.
Makovey et al.[9] in their case–control study of 93 pairs of opposite-sex twins identified a significant relation between BMD and female sex.
Serum calcium level is maintained at 9–11 mg/dl by a complex interplay between parathyroid hormone (PTH), Vitamin D, and calcitonin.[10] Hence, serum Ca++ may be normal in the cases with osteoporosis.[10] Of the total 100 cases, 38% had serum calcium values below 9 mg/dl and 62% had serum calcium values in normal range of 9–11 mg/dl. In the present study, we did not observe any significant association between Ca++ and BMD.
Harinarayan et al.[11] measured serum Ca++ and Vitamin D in 191 women and found no relationship between serum Ca++ and BMD. In the present study, we obtained similar results.
However, Singh et al.[12] in a study of 230 postmenopausal women found a significant relation between serum Ca++ and BMD. The findings of these studies from different settings may not be consistent with the findings of our study, and the reason might be due to small sample size and single-center study with hospital-based population.
In our study, there was no significant relation between serum ALP and BMD. However, Ali et al.[13] found a significant correlation between serum ALP and BMD in their study.
The mean value of serum Vitamin D in patients included in the study was 20.72 ng/ml, and for controls, the mean value was 28.74 ng/ml. OR for relationship between Vitamin D and BMD was calculated to be 1.8 (CI: 1.2–3.6) for distal radius BMD and OR for calcaneal BMD was calculated to be 1.7 (CI: 1.1–3.2), which was found to be statistically significant.
Our findings support the findings by Sahota et al.[14] who measured serum Vitamin D in 421 women and found a significant relation between BMD and serum Vitamin D. Arya et al.[15] measured BMD in 92 young healthy volunteers (67 females and 25 males) and found a significant association between serum Vitamin D and BMD.
Garg et al.[16] studied Vitamin D, PTH, and BMD in 1829 adolescents (males – 816 and females – 1013) and 1346 adults >50 years (males – 643 and females – 703), and there was a significant association between Vitamin D and BMD. They also suggested that 30%–40% of patients with Vitamin D deficiency have hyperparathyroidism.
Distal end radius fracture is one of the most important predictors of osteoporosis.[3] The presence of distal end radius fracture is evidence enough to initiate prophylactic antiosteoporotic medications irrespective of BMD T-score of an individual[17] in elderly patients and postmenopausal women.
In this study of 100 cases and matched controls, the prevalence of osteoporosis and osteopenia was 45% and 43% at calcaneum and 45% and 39% at distal radius, respectively. The mean BMD was significantly lower in cases compared to their controls.
In the case–control study of 664 females and 85 males with distal end radius fractures, Oyen et al.[18] found the prevalence of osteoporosis in patients with DER fractures (34% in females and 17% in males) to be significantly higher than in controls (10% in females and 13% in males. OR was calculated to be 7.1 (CI: 4.3–11.6) for the association of DER fractures with osteoporosis.
Dhainaut et al.[19] in their case–control study of 123 females with DER fractures and 170 controls found a significant association between DER fracture and osteoporosis. Mallmin et al.[7] found a significant association between BMD of 7 males and 67 female patients with DER fractures and matched controls. They suggested that patients with DER fractures constitute a distinct target group for the prevention of osteoporosis.
Rozental et al.[17] in their study of 40 premenopausal women with DER fractures and 80 matched controls found lower distal radius BMD in cases compared to controls, and the association was statistically significant (OR: 1.52, CI: 1.1–2.39), but they found that trabecular microarchitecture was significantly deteriorated in cases than controls even with normal BMD based on high-resolution peripheral quantitative computed tomography (HR-pQCT). In this study, in the age group of <45 years' females, the mean BMD was significantly lower in patients with DER fractures than controls. Wigderowitz et al.[8] in their study of 235 women with DER fractures between the age group of 20 and 80 years found a significant correlation between contralateral distal radius pDEXA and presence of DER fractures. They also found significantly lower BMD in premenopausal women with DER fractures <45 years which is similar to our study.
This study was a single-center study, and the number of male participants in our study was higher than that of females. It was found that female patients were generally reluctant in participating in the study. This may have been due to the high cost of investigations such as pDEXA and Vitamin D. Our study was a nonfunded study. This may have a source of selection bias in our study.
Conclusion
Our study indicates that distal end radius fracture is a significant risk factor for osteoporosis independent of age or sex. It emphasizes the critical role of advancing age, female sex, and low serum Vitamin D level as significant predictors for osteoporosis. Since a distal end radius fracture is a predictor of a second fragility fracture, all patients of distal end radius fractures should be screened for osteoporosis by measuring BMD irrespective of age and sex of the patients. These patients should also be tested for serum Vitamin D which is an independent risk factor for osteoporosis. Early detection of osteoporosis and timely initiation of antiosteoporotic therapy can go a long way in reducing the socioeconomic burden of osteoporosis and associated fragility fractures. It is, therefore, necessary to create awareness among rural masses about the risk of osteoporosis and importance of its screening. Efforts must be made so as to make the screening of osteoporosis a routine medical practice as we continue our efforts of making the world a healthier place to live in.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Consensus Development Conference-Diagnosis, Prophylaxis, and Treatment of Osteoporosis. New York: Excerpta Medica Inc.; 1993.
- Hip fractures in the elderly: A world-wide projection. Osteoporos Int. 1992;2:285-9.
- [CrossRef] [PubMed] [Google Scholar]
- Secondary prevention of osteoporosis after colles fracture: Current practice. Joint Bone Spine. 2008;75:50-2.
- [CrossRef] [PubMed] [Google Scholar]
- The orthopaedic treatment of fragility fractures. Clin Cases Miner Bone Metab. 2007;4:108-16.
- [Google Scholar]
- The epidemiology of distal radius fractures. Hand Clin. 2012;28:113-25.
- [CrossRef] [PubMed] [Google Scholar]
- Side differences in the bone density of the distal radius and calcaneus in Koreans aged 4-86 years. J Clin Densitom. 2007;10:184-8.
- [CrossRef] [PubMed] [Google Scholar]
- Colles' fracture associated with reduced bone mineral content. Photon densitometry in 74 patients with matched controls. Acta Orthop Scand. 1992;63:552-4.
- [CrossRef] [PubMed] [Google Scholar]
- Peripheral bone mineral density in patients with distal radial fractures. J Bone Joint Surg Br. 2003;85:423-5.
- [CrossRef] [PubMed] [Google Scholar]
- Gender differences in relationships between body composition components, their distribution and bone mineral density: A cross-sectional opposite sex twin study. Osteoporos Int. 2005;16:1495-505.
- [CrossRef] [PubMed] [Google Scholar]
- Calcium metabolism in health and disease. Clin J Am Soc Nephrol (5 Suppl 1):S23-30.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D status and bone mineral density in women of reproductive and postmenopausal age groups: A cross-sectional study from south India. J Assoc Physicians India. 2011;59:698-704.
- [Google Scholar]
- Screening of bone mineral density by densitometer and correlation with serum calcium and Vitamin D levels to detect early osteoporotic changes in postmenopausal women in slum areas of Raipur and Kalupur of Ahmedabad. International Journal of Basic and Clinical Pharmacology. 2015;4:960.
- [CrossRef] [Google Scholar]
- Validity of osteocalcin and alkaline phosphatase biomarkers in postmenopausal women with low bone mineral density. Chem Mater Res. 2014;6:13-9.
- [Google Scholar]
- The relationship between Vitamin D and parathyroid hormone: Calcium homeostasis, bone turnover, and bone mineral density in postmenopausal women with established osteoporosis. Bone. 2004;35:312-9.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D status and its relationship with bone mineral density in healthy Asian Indians. Osteoporos Int. 2004;15:56-61.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between serum 25-hydroxy vitamin D, parathormone and bone mineral density in Indian population. Clin Endocrinol (Oxf). 2014;80:41-6.
- [CrossRef] [PubMed] [Google Scholar]
- Premenopausal women with a distal radial fracture have deteriorated trabecular bone density and morphology compared with controls without a fracture. J Bone Joint Surg Am. 2013;95:633-42.
- [CrossRef] [PubMed] [Google Scholar]
- Osteoporosis as a risk factor for distal radial fractures: A case-control study. J Bone Joint Surg Am. 2011;93:348-56.
- [CrossRef] [PubMed] [Google Scholar]
- Cortical hand bone porosity and its association with distal radius fracture in middle aged and elderly women. PLoS One. 2013;8:e68405.
- [CrossRef] [PubMed] [Google Scholar]




