
Translate this page into:
Blood flow restriction therapy to restore quadriceps wasting persistent after anterior cruciate ligament reconstruction
Address for correspondence: Dr. Shubham Agarwal, Department of Orthopaedics, Dr SN Medical College, 88/3, Vijay Bari, Sikar Road, Jaipur 302023, Rajasthan, India. E-mail: shubham.ag1993@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Jain H, Agarwal S, Raichandani K, Vaishy A. Blood flow restriction therapy to restore quadriceps wasting persistent after anterior cruciate ligament reconstruction. J Orthop Spine 2022;10:1-5.
Abstract
INTRODUCTION:
Anterior cruciate ligament (ACL) is the most commonly injured ligament in the knee that requires surgical intervention. After ACL reconstruction, it has been reported that quadriceps wasting can persist for years even after complete rehabilitation and aggressive physiotherapy. Blood flow restriction (BFR) therapy is proposed to induce muscle growth and improve strength in chronic muscle atrophy. But the data on the efficacy of BFR therapy are controversial and lacking in the existing literature.
AIMS/OBJECTIVES:
In this study, we focus on identifying the patients having chronic quadriceps wasting after ACL reconstruction and intervene to restore the quadriceps wasting using BFR therapy.
MATERIALS AND METHODS:
All the participants had unilateral reconstruction of ACL tear >1 year back and completed the standard postoperative rehabilitation protocol but had >10% of difference in quadriceps thickness in the involved limb as compared to contra-lateral limb measured by ultrasonography. They were then proceeded further with BFR therapy and were re-examined after 6 weeks of BFR therapy.
RESULTS:
It was observed that 64% of the participants had persistent quadriceps muscle atrophy even after 1 year of completing standard post-rehabilitation protocol after ACL reconstruction with more than 10% deficit. The quadriceps thickness observed after the BFR therapy increased by 10 ± 7% at one-third of femur length from knee joint and 16.6 ± 4% at two-thirds of femur length in the involved extremity but did not show any change in uninvolved extremity. Post-training quadriceps femoris symmetry index also increased in the involved extremity compared to the baseline (87 ± 5% pre-procedure to 96 ± 4% post-procedure, P <0.01).
CONCLUSION:
This study concludes that BFR therapy after knee surgery may be a viable modality for the treatment of residual atrophy of quadriceps after years of ACLR. This can be used in patients who require extra assistance in resisting muscle atrophy or building muscle strength.
Keywords
Atrophy treatment
chronic wasting
quadriceps atrophy
rehabilitation

Introduction
Anterior cruciate ligament (ACL) is the most commonly injured ligament in the knee that requires surgical intervention. After ACL reconstruction, it has been reported that quadriceps wasting can persist for years even after complete rehabilitation and aggressive physiotherapy. This can lead to altered gait mechanics and increase the chances of re-injury in the patients. Due to asymmetry in the quadriceps and disturbance in weight mechanics, it can also lead to the development of early osteoarthritis of the knee joint.
Blood flow restriction (BFR) therapy is proposed to induce muscle growth and improve strength in population.[1,2,3] Here, we occlude the venous outflow to the extremity while restricting arterial inflow using a pneumatic tourniquet followed by low resistance exercises. The anaerobic conditions are induced and act as angio-genic stimulus via vascular endothelial growth factor (VEGF). There is also a proliferation of satellite cells[4,5] activation of type 2 muscle fibers[6,7,8] and recruitment of endothelial progenitor cells. Low-intensity training is an attractive method of recovery of quadriceps in postsurgical rehabilitation after ACLR.
BFR therapy is yet to be established as a conclusive method for rehabilitation as the data on the efficacy of BFR therapy is controversial and lacking in the existing literature. The purpose of this study was to evaluate the BFR therapy to increase quadriceps strength and symmetry 1 year after ACLR. We also report the safety considerations and indications for the same.
Objectives
In this study, we focus on identifying the patients having chronic quadriceps wasting after ACL reconstruction and completing the rehabilitation protocol. We will also intervene to restore the quadriceps girth using BFR therapy.
Materials and Methods
The study was conducted in the Department of Orthopedics of a tertiary level health care center, for a period of 12 months from March 1, 2019 to February 29, 2020 after obtaining ethical clearance from Institutional Ethical Committee.
All the patients between the age of 18 and 45 years, with ACL complete tear operated arthroscopically, with semi-tendinosus and gracilis graft used for reconstruction, and those giving consent to participate in the surgery were included. All the participants had unilateral reconstruction of ACL tear >1 year back and completed the standard postoperative rehabilitation protocol but had >10% of difference in quadriceps thickness in involved limb as compared to contralateral limb.
We excluded the patients who had any comorbidity that can affect the muscle rehabilitation and strength such as polio, paralysis, and any condition requiring prolonged immobilization. Patients with suspected/any old episode of DVT, those having any infections postoperatively, with multi-ligaments injuries, having any injury in contra lateral knee, refusing to participate in the study, or those who did not return for proper follow-ups were also excluded from the study.
After 12 months of the surgery, the patients were evaluated for quadriceps thickness. The femur length was taken from the medial joint line to greater trochanter (GT) and divided into three equal parts by 2 points, at one-third of femur length and two-third of femur length (from knee joint). Ultrasonography (USG) (7 MHz, Aloka portable USG machine) was then performed to measure quadriceps thickness for both the limbs, that is, the involved and the contralateral limb at these two fixed points (one-third and two-thirds of femur length from knee joint). Participants were positioned supine (10° knee angle), while images of the quadriceps were taken at one-third and two-thirds of the distance from knee joint line to the greater trochanter of femur. To maintain the uniformity, the evaluation was done by a single radiologist in the department of radio diagnosis for all the patients.
These participants were informed about the therapy, informed consent was taken and proceeded further with BFR therapy [Figure 1]. A pneumatic tourniquet cuff was applied to the thigh and set to a limb occlusion pressure of 70%–80% of arterial occlusive pressure (AOP). In this study, AOP was measured using Doppler ultrasound. All the patients were then allowed to follow standard rehabilitation at the same physical therapy clinic for 40 min, three times a week. This included the following:

- BFR tourniquet with exercises
Straight leg raise: 40 reps
Quad sets: 40 reps
Cycling: 10 min
Step ups: 40 reps
Balancing on affected limb: 5 min
Apart from the BFR therapy at clinic, the patients were allowed to continue the same without tourniquet at home for the other 4 days of the week.
Thickness of the quadriceps was re-evaluated after 6 weeks of therapy in the involved and uninvolved limb using B-mode ultrasound. Symmetry index was used to compare wasting of involved and un-involved limb:

Results
Demography: We evaluated 75 patients during the course of study for the thickness of quadriceps after 1 year of ACLR. Out of 75, we found wasting of quadriceps in operated limb of >10% in 48 candidates and were included for study. The demographic profile is listed in [Table 1].
| Variable | |
|---|---|
| Age (years) | 28 ± 6 |
| Weight (kg) | 74 ± 9 |
| Sex | |
| Male | 33 |
| Female | 15 |
| Time from ACLR (years) | 1.5 ± 0.4 |
BFR exercise
Mean arterial occlusion pressure was observed to be 188 ± 24 mm Hg and mean occlusion pressure was accordingly taken as 132 ± 17 mm Hg. All the participants were observed to complete all the sets of rehabilitation protocols. Muscle soreness was reported by 30% of the patients during the first few sets of therapy, but it gradually reduced with subsequent therapies. None of the patients reported DVT or any nerve injuries.
The quadriceps thickness observed after the BFR therapy increased by 10 ± 7% at 1/3 of femur length from knee joint and 16.6 ± 4% at two-thirds of femur length in the involved extremity but did not show any change in uninvolved extremity [Figure 2].
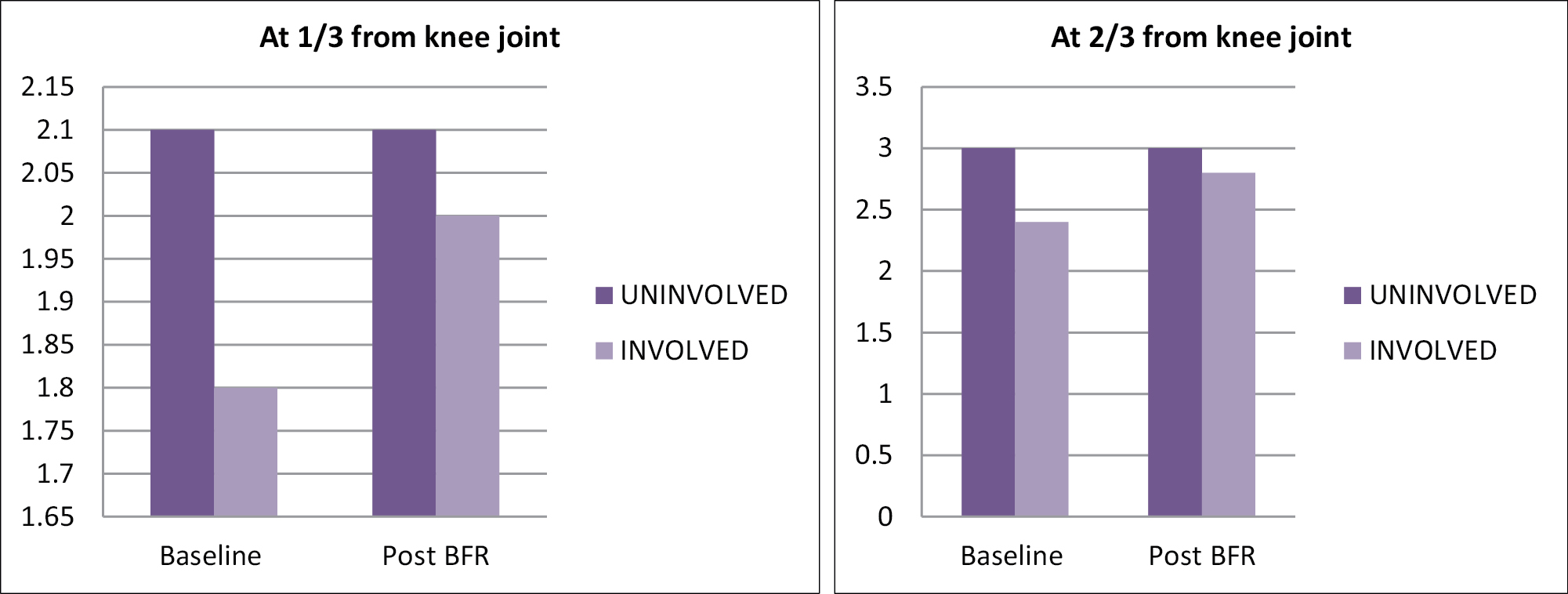
- Quadriceps thickness before and after BFR therapy
Post-training quadriceps femoris symmetry index [Figure 3] also increased in the involved extremity compared to the baseline (87 ± 5% pre-procedure to 96 ± 4% post-procedure, P < 0.01).
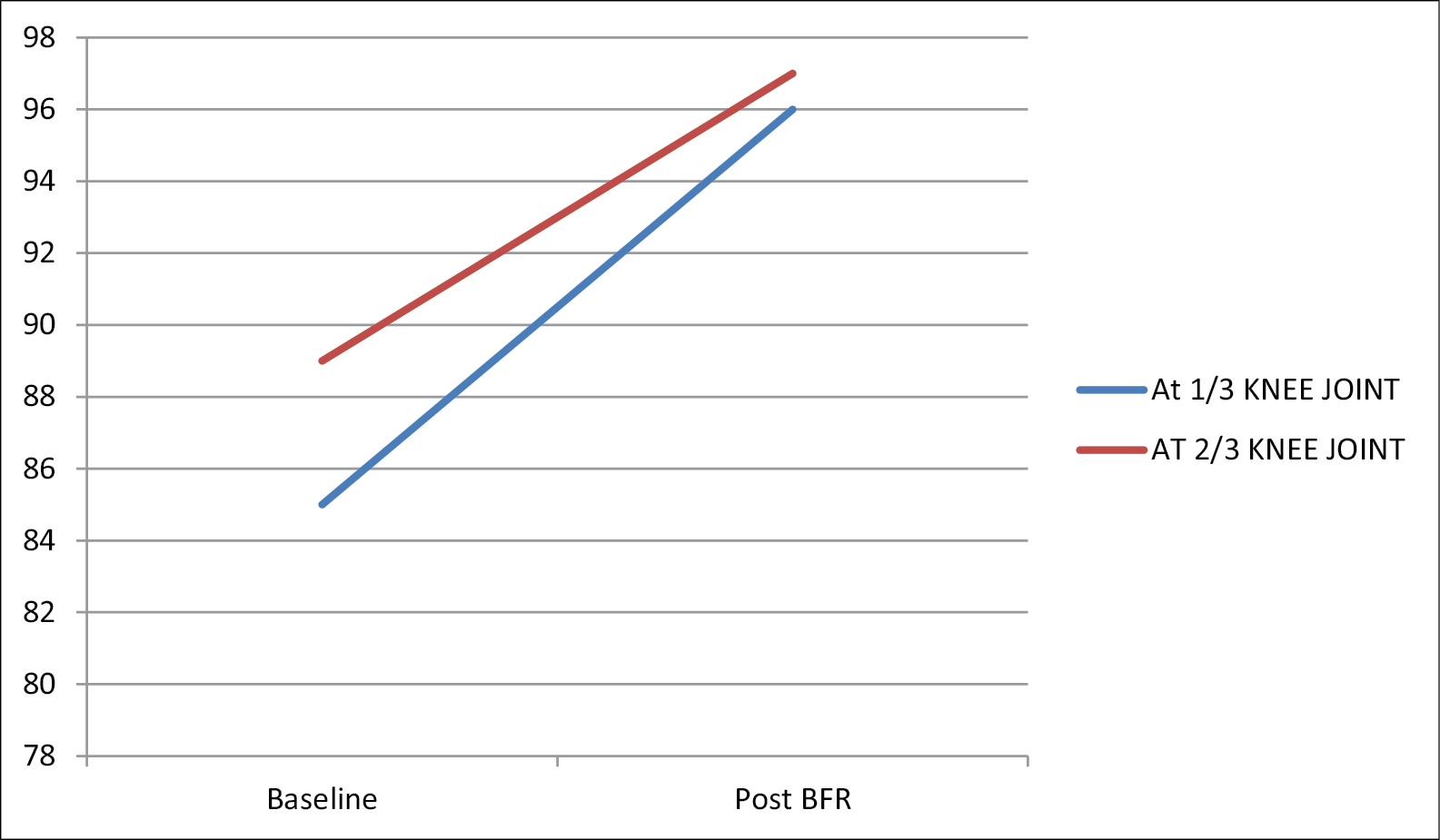
- Quadriceps symmetry index before and after BFR therapy
Discussion
In this study, it was observed that 64% of the participants had persistent quadriceps muscle atrophy even after 1 year of completing standard post-rehabilitation protocol after ACL reconstruction. These patients had >10% difference in quadriceps thickness and asymmetry between the involved and uninvolved limb. This asymmetry long after ACLR has been previously reported by various authors in the past.[9,10,11] As quadriceps is responsible to maintain extensor mechanism of knee joint, its reduction leads to weak extensor strength. Also, the chances of re-injury increases due to altered gait imbalances and weight mechanics.[12,13,14]
In this study, we implemented a 6 week, observed BFR program in the physiotherapy clinic for 3 days a week, consisting of bodyweight and strengthening exercises to increase the bulk as well as strength of muscle. We found that BFR therapy lead to an increase of quadriceps thickness by 10 ± 7% at one-third of femur length from knee joint and 16.6 ± 4% at two-thirds of femur length in the involved extremity but did not show any change in uninvolved extremity. This also leads to an increase in post-training quadriceps femoris symmetry index. Hence, BFR therapy after ACLR can be used for resisting the effects of disuse atrophy as well as building the strength and bulk to regain the levels equal to un-involved extremity.
BFR therapy is hypothesized to promote muscle bulk as it induces local hypoxia. The type 1 muscle fibers cannot function in the hypoxic environment and this leads to activation of type 2 muscle fibers, thus promoting the hypertrophy of muscle.[15] It leads to the accumulation of metabolic bi-products that result in various hormonal and metabolic responses.[16] Increase in blood pooling and concentration of adrenaline and Growth hormone also leads to muscle growth.[17]
Here we observed the quadriceps thickness at two levels, one at one-third of the femur length from knee joint line and the other at two-third from the knee joint line to rule out bias at a single level. Various other authors have used other methods for the same. Iversen et al.[18] used landmarks at 40% and 50% of femur length to record quadriceps CSA, whereas Takarada et al.[19] measured the CSA at mid-portion of femur and at the point just distal to BFR tourniquet.
Various authors have previously reported the results of BFR therapy after knee surgery but the results are still controversial. Ohta et al.[20] in a randomized controlled trial over 16 weeks of BFR therapy and observed significant improvements in CSA of the quadriceps and extensor strength of knee. Kilgas et al.[21] in their study in 2019 implemented home-based BFR therapy several years after ACLR and reported an increase in quadriceps muscle thickness and reduced asymmetry. In a 13-day low resistance training using BFR therapy by Iverson[18] there was no difference observed in CSA of quadriceps when compared to low-resistance muscular training alone.
Thus, BFR therapy after knee surgery may be a viable modality for the treatment of residual atrophy of quadriceps after years of ACLR. This can be used in patients who require extra assistance in resisting muscle atrophy or building muscle strength. However, due to various controversies, this is not a regular intervention in post-operative knee rehabilitation thus leading to chronic wasting of quadriceps.
We noticed no significant side effects apart from some transient dull pain observed in the affected limb during the initial three to four therapies that settled after rest following therapy, with only 3 patients requiring nonsteroidal anti-inflammatory drug for pain relief on the day of therapy. Ohta et al.[20] reported discomfort in the participants affected extremity roughly 12 min after BFR therapy, whereas Kilgas[21] and Iversan[18] reported no significant side effects. However, in a study by Yasuda et al.[22] there were episodes of rhabdomyolysis, pulmonary emboli as well as venous thrombosis reported after BFR therapy. We did not observe any such side effects in any of the participants. Thus, Additional data are needed on the short- and long-term effects of BFR in patient populations.
Limitations
This study had a few limitations. In this study, we concluded short-term benefits on muscle hypertrophy after BFR therapy but did not follow up for long-term results. Also, we did not use MRI for evaluation of quadriceps thickness (standard technique for the same) as it is not affordable by the patients.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Not applicable.
Conflicts of interest
There are no conflicts of interest.
References
- Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br J Sports Med. 2017;51:1003-11.
- [CrossRef] [PubMed] [Google Scholar]
- Blood flow-restricted training for lower extremity muscle weakness due to knee pathology: A systematic review. Sports Health. 2019;11:69-83.
- [CrossRef] [PubMed] [Google Scholar]
- The role of blood flow restriction therapy following knee surgery: Expert opinion. Arthroscopy. 2018;34:2506-10.
- [CrossRef] [PubMed] [Google Scholar]
- Activation of mTORC1 signaling and protein synthesis in human muscle following blood flow restriction exercise is inhibited by rapamycin. Am J Physiol Endocrinol Metab. 2014;306:E1198-204.
- [CrossRef] [PubMed] [Google Scholar]
- Skeletal muscle protein balance and metabolism in the elderly. Curr Aging Sci. 2011;4:260-8.
- [CrossRef] [PubMed] [Google Scholar]
- Blood flow restriction: The metabolite/volume threshold theory. Med Hypotheses. 2011;77:748-52.
- [CrossRef] [PubMed] [Google Scholar]
- Oxygen availability and motor unit activity in humans. Eur J Appl Physiol Occup Physiol. 1992;64:552-6.
- [CrossRef] [PubMed] [Google Scholar]
- Ischemic strength training: A low-load alternative to heavy resistance exercise? Scand J Med Sci Sports. 2008;18:401-16.
- [CrossRef] [PubMed] [Google Scholar]
- Factors explaining chronic knee extensor strength deficits after ACL reconstruction. J Orthop Res. 2011;29:633-40.
- [CrossRef] [PubMed] [Google Scholar]
- The architecture of the ipsilateral quadriceps two years after successful anterior cruciate ligament reconstruction with bone-patellar tendon-bone autograft. Knee. 2014;21:721-5.
- [CrossRef] [PubMed] [Google Scholar]
- Persistent neuromuscular and corticomotor quadriceps asymmetry after anterior cruciate ligament reconstruction. J Athl Train. 2015;50:303-12.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between isokinetic strength and tibiofemoral joint space width changes after anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42:302-11.
- [CrossRef] [PubMed] [Google Scholar]
- Quadriceps muscle weakness after anterior cruciate ligament reconstruction: a risk factor for knee osteoarthritis? Arthritis Care Res (Hoboken). 2010;62:1706-14.
- [CrossRef] [PubMed] [Google Scholar]
- Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50:804-8.
- [CrossRef] [PubMed] [Google Scholar]
- The effects of endurance strength, and power training on muscle fiber type shifting. J Strength Cond Res. 2012;26:1724-9.
- [CrossRef] [PubMed] [Google Scholar]
- Role of metabolic stress for enhancing muscle adaptations: Practical applications. World J Methodol. 2017;7:46-54.
- [CrossRef] [PubMed] [Google Scholar]
- Studies on the regulation of the circulation in man, With special reference to the stroke volume and the effect of muscular work, body position and artificially induced variations of the heart rate. Acta Physiol Scand Suppl. 1962;57:1-36.
- [CrossRef] [PubMed] [Google Scholar]
- Intermittent blood flow restriction does not reduce atrophy following anterior cruciate ligament reconstruction. J Sport Health Sci. 2016;5:115-8.
- [CrossRef] [PubMed] [Google Scholar]
- Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles. Med Sci Sports Exerc. 2000;32:2035-9.
- [CrossRef] [PubMed] [Google Scholar]
- Low-load resistance muscular training with moderate restriction of blood flow after anterior cruciate ligament reconstruction. Acta Orthop Scand. 2003;74:62-8.
- [CrossRef] [PubMed] [Google Scholar]
- Exercise with blood flow restriction to improve quadriceps function long after ACL reconstruction. Int J Sports Med. 2019;40:650-6.
- [CrossRef] [PubMed] [Google Scholar]
- Combined effects of low-intensity blood flow restriction training and high-intensity resistance training on muscle strength and size. Eur J Appl Physiol. 2011;111:2525-33.
- [CrossRef] [PubMed] [Google Scholar]




