
Translate this page into:
“Black disc” Tandem Spinal Stenosis in Ochronotic Arthropathy
Address for correspondence: Dr. Pradhyumn Rathi, Department of Spine, Sancheti Institute of Orthopedics and Rehabilitation, Pune - 411 005, Maharashtra, India. E-mail: pradhyumnrathi@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Hadgaonkar S, Rathi P, Shyam A, Sancheti P. “Black disc” tandem spinal stenosis in ochronotic arthropathy. J Orthop Spine 2020;8:41-5.
Abstract
Alkaptonuria (AKU) is a rare hereditary autosomal recessive disorder characterized by a defect in the gene for enzyme homogentisate 1,2-dioxygenase resulting in the metabolic disorder of phenylalanine and tyrosine. Tandem spinal stenosis refers to spinal canal diameter narrowing in at least 2 distinct regions of the spine, most commonly the lumbar and cervical regions. This entity can be an asymptomatic radiographic finding, or it can present with severe myelopathy and lower-extremity symptoms. On review of literature, in PubMed and Google Scholar, there were no cases of ochronotic tandem spinal stenosis. This is the first case to be reported in the world literature of ochronotic tandem spinal stenosis operated surgically. We report a rare case of a patient suffering from ochronosis with tandem spinal stenosis who was diagnosed during the late course of disease once the myelopathy had set in resulting in increased neck and back pain and associated with walking trouble and clumsiness in hands. A 60-year-old hypertensive farmer suffering from late-stage ochronotic arthropathy with tandem spinal stenosis with cervical spondylotic myelopathy with lumbar disc protrusion with radiculopathy was surgically treated with single-stage simultaneous decompression surgery. His early follow-up showed marked improvement. AKU is a rare metabolic genetic disorder that is caused by the deficiency of homogentisic acid oxidase, affecting multiple organ systems in the body. Detailed history can help diagnose it early and accurately. Ochronotic arthropathy can cause tandem spinal stenosis by ligamentum flavum thickening and disc protrusions, which if overlooked can lead to serious complications. Meticulous preoperative and intraoperative planning with expeditious implementation helps to achieve a successful outcome after a single simultaneous procedure.
Keywords
Alkaptonuria
decompression surgical
ochronosis
spinal cord diseases
spinal stenosis

Introduction
Alkaptonuria (AKU) is a rare hereditary autosomal recessive disorder characterized by a defect in the gene for enzyme homogentisate 1,2-dioxygenase resulting in the metabolic disorder of phenylalanine and tyrosine.[1] This enzyme catalyzes the conversion of homogentisic acid (HGA) to maleylacetoacetic acid, and its absence leads to an increase in HGA accumulation in the body. The excess HGA excreted through urine turns dark on exposure to oxygen or alkalization called AKU. Accumulated HGA oxidizes within the connective tissue irreversibly and turns into melanin-like pigment, especially in the cartilage of the joints and in the intervertebral discs, which is named as ochronosis.[2,3]
Ochronosis affects the cardiovascular, genitourinary, and respiratory systems and musculoskeletal system. The disease progresses from AKU to alkaptonuric ochronosis, leading to ochronotic arthropathy.[4] Numerous reports on the successful management of ochronotic arthropathy of the peripheral joints such as the knee and hip joints using total joint replacement are available.[3,5,6] However, there is a paucity of reports on successful surgical intervention for tandem spinal stenosis in ochronosis.
Tandem spinal stenosis refers to spinal canal diameter narrowing in at least 2 distinct regions of the spine, most commonly the lumbar and cervical regions. This entity can be an asymptomatic radiographic finding, or it can present with severe myelopathy and lower-extremity symptoms. On review of literature, in PubMed and Google Scholar, there were no cases of ochronotic tandem spinal stenosis.[7] This is the first case to be reported in the world literature of ochronotic tandem spinal stenosis operated surgically. We report a rare case of a patient suffering from ochronosis with tandem spinal stenosis who was diagnosed during the late course of disease once the myelopathy had set in resulting in increased neck and back pain and associated with walking trouble and clumsiness in hands.
Case Report
A 60 years old farmer came to the outpatient with complaints of pain in his lower back. He also complained of difficulty walking, instability in gait, and clumsiness in hands. He was apparently alright 4 years back when he noticed difficulty to perform fine motor activities. He also felt stiffness in all large joints with difficulty to maintain balance while walking. It has progressed till presently he has severe right leg pain with associated tingling and numbness and a feeling of heaviness in legs. His claudication distance gradually reduced from 100 m to few steps. He had to be assisted by a walker for ambulation since the past 2 years. He had received conservative treatment for the same but in vain. There was no family history of similar illnesses.
Physical examination showed cyan pigmentation on the nose, sclera, and the ear auricle. The neck and back movements were restricted. Positive Romberg and tandem gait signs and the finger-escape sign were observed. The grip-and-release test was 8 movements at both hands in 10 s, which was obviously inferior to the normal criterion of above 20 movements. Paresthesia was seen in both upper extremities, but no motor weakness was observed. Bilateral Hoffmann reflex and inverted radial reflex were present. Bilateral tendo-achilles reflex demonstrated ill-sustained clonus. There was no sensory–motor involvement in all four limbs. The preoperative modified Japanese Orthopedic Association (mJOA) myelopathy score for him was 13.
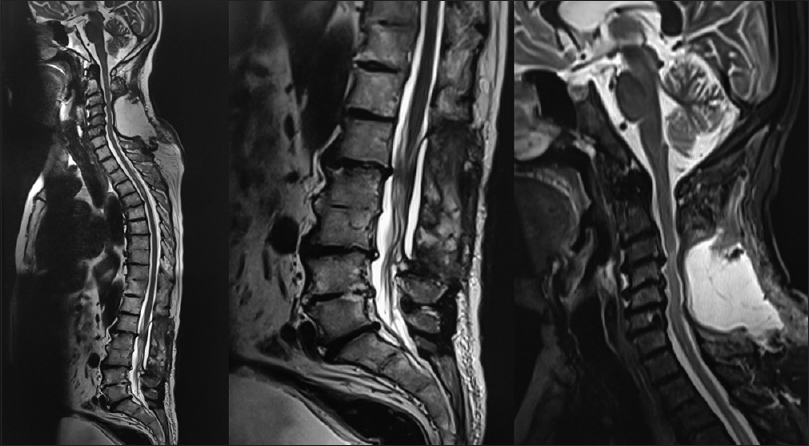
X-rays of the neck [Figure 1] revealed advanced arthritic changes with gross reduction in disc spaces at C2–3, C3–4, C4–5, and C5–6 levels but no loss of lordosis, while that of the lumbar spine [Figure 2] showed bony ankylosis at D12–L1, L2–3, and L4–5 levels with loss of lordosis and sclerosis at the end plates of L1–2, L3–4, and L5–S1 levels. Magnetic resonance imaging (MRI) [Figures 3 and 4] showed C3–4, C4–5, C5–6, and C6–7 disc protrusions with cervical spinal cord compression with signal changes suggestive of myelomalacia at C6–7 level due to additional ligamentum flavum thickening/calcification. Furthermore, there was L1–2, L3–4 lumbar canal stenosis due to hypertrophy of the ligamentum flavum and facet arthropathy.

- X-rays of the neck revealed advanced arthritic changes with gross reduction in disc spaces at C2–3, C3–4, C4–5, and C5–6 levels but no loss of lordosis

- X-rays of the lumbar spine showed bony ankylosis at D12–L1, L2–3, and L4–5 levels with loss of lordosis and sclerosis at the end plates of L1–2, L3–4, and L5–S1 levels

- Magnetic resonance imaging showed C3–4, C4–5, C5–6, and C6–7 disc protrusions with cervical spinal cord compression with signal changes suggestive of myelomalacia at C6–7 level due to additional ligamentum flavum thickening/calcification
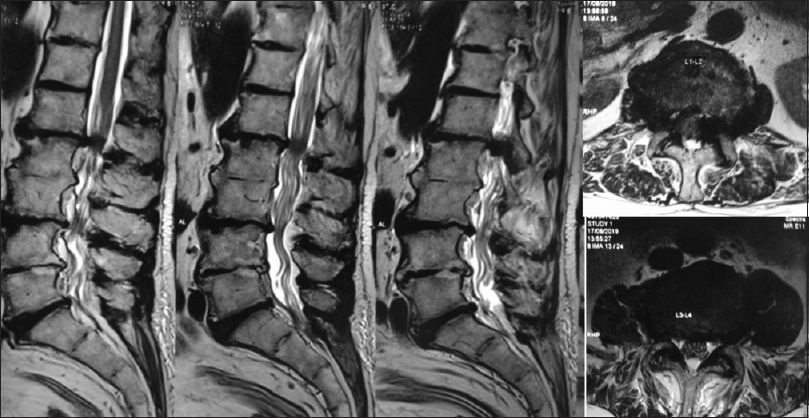
- Magnetic resonance imaging showed L1–2 and L3–4 lumbar canal stenosis due to hypertrophy of the ligamentum flavum and facet arthropathy
As the color of the patient's urine turned dark after exposure to air after 2 h [Figure 5], the patient's urine sample was screened for metabolic disorder. The measured value for HGA was 1120.04, while the normal value should be 0. Hence, we confirmed the presence of AKU.
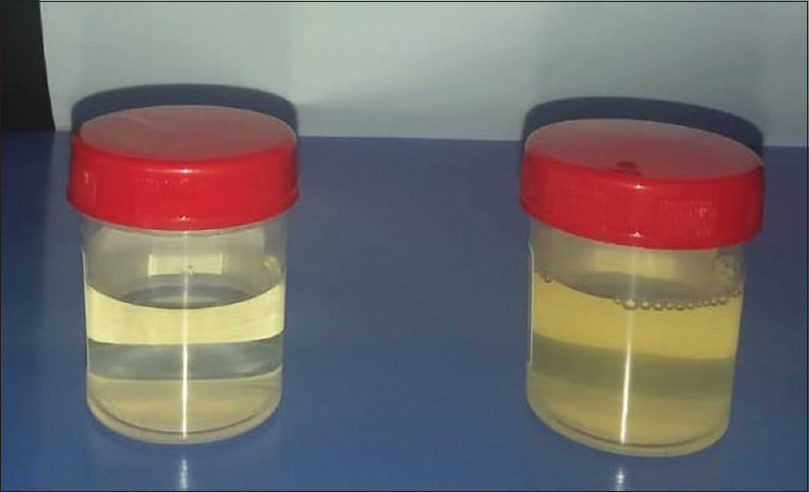
- The color of the patient's urine turned dark after exposure to air after 2 h
The patient underwent a single-stage tandem decompression surgery in the form of C3–C7 laminectomy and L1–L3 laminectomy. The arterial line was taken. Hypotension with mean arterial pressure between 85 and 95 mmHg was maintained. Both sites were painted draped and separately prepared, but simultaneous skin incision and exposure was started by the spine surgeons. Adequate hemostasis was achieved using electrocautery. On cervical spine exposure, black ligamentum nuchae were identified easily which helped us to be in the avascular plane. Interspinous ligaments also turned black on exposure to air. Two tracts were burred along the lamina-lateral mass junction from C3–C7. The thinned bone was removed with Kerrison rongeurs. On exposure to air, the flavum blackened and hardened, so it was imperative to perform a prompt flavectomy at the proximal C2–3 and distal C7–C8 levels. The posterior elements were detached in toto. Undercutting was done at C2–3 level, and all flavum was removed. Decompression and epidural bleeding along the gutters were controlled using Gelfoam and manual compression for a few minutes.
At the lumbar levels, similar findings were noted. Flavum on hardening was difficult to cut with rongeurs and had to be removed along with the bone fragments of the laminae. Expeditious canal decompression was one, and lateral recess was decompressed by partial medial facetectomy. Bilateral L1, L2, L3, and L4 nerve roots were identified. No discectomy was done. Closure was done in layers over a Romo Vac drain, and anesthesia was reversed. The operative duration was 136 min and estimated blood loss was 850 cc. On extubation, the patient was monitored in the high dependency unit and was subsequently shifted toward on the 1st postoperative day (POD) when he was mobilized out of bed. He was made to stand on POD2 and walked with walker on POD3. His spasticity persisted, and on POD5, the patient was discharged home.
The postoperative X-rays [Figure 6] showed the C3–C7 and L1–L3 laminectomy defects.

- Postoperative X-rays showed the C3–C7 and L1–L3 laminectomy defects
At the 6 week follow-up, the patient was walking better with support. His clumsiness in grip had reduced, and standing and walking times were improved to 20 min and 40 m, respectively. His mJOA score improved to 16 which correlated with his MRI [Figure 7].
- Magnetic resonance imaging showing adequate decompression
Discussion
Tandem spinal stenosis refers to spinal canal diameter narrowing in at least 2 distinct regions of the spine, most commonly the lumbar and cervical regions. It is a common condition present in up to 60% of patients with spinal stenosis. This entity can be an asymptomatic radiographic finding, or it can present with severe myelopathy and lower-extremity symptoms. There were only 10 clinical studies of patients with symptomatic tandem spinal stenosis, but none were due to ochronosis.[7]
Cervical spondylotic myelopathy follows a protracted clinical course consisting of a longer period of relatively stable symptoms punctuated by exacerbation of variable duration. It is usually due to degenerative changes in the spine with the osteophytes from the posterior part of the vertebral body and an uncinate process encroaching upon the neural canal.
For patients with moderate-to-severe symptoms, the surgical intervention should be considered as a possible procedure to prevent further neurologic deterioration and create a chance for recovery from myelopathy.[4,6,8]
AKU gives symptoms that may give an instant clue to the diagnosis like the urine turns to dark on exposure to air and discoloration on sclera, jowl, as well as in the underwear; the patients can often neglect the symptoms and appear at late in the course of the disease.[5,8] In few cases it may be neglected until the fourth or fifth decade when the symptoms secondary to ochronosis develop and the patients report to physicians. The disease affecting the spine follows a chronological sequence, the patient usually first suffers from ochronotic spondylosis which is accompanied with the peripheral joint arthropathy,[9] and it progresses to cervical spondylotic myelopathy which warrants surgical intervention. The initial complaints usually include low back or neck pain with stiffness and occasionally sciatica resulting from disc protrusion.[10] Involvement of large joints usually occurs several years after the spinal disorders.[11]
The characteristics of ochronotic spondylosis are multiple disc space narrowing, vacuum phenomenon, and calcification in a water-like pattern due to the sparing of the central nucleus pulposus.[12,13] In the present case report, findings from the MRI on the cervical region revealed that the thickened ligamentum flavum appeared to be the main cause behind the cord compression at C67 and lumbar disc protrusions. This could be secondary to the fact that the HGA could bind irreversibly by a process of polymerization and oxidation to connective tissue collagen. This prevents the collagen cross-link formation, which leads to the abnormality of the ligamentum flavum.[3,12,14] The thickening of the abnormal flavum could be attributed to instability being caused by repeated inflammation of the facet joints in AKU. This abnormal flavum when exposed to the atmosphere during surgery hardens and becomes difficult to remove.
There is no specific treatment for AKU. Nowadays, all the available methods are only symptomatic for the early stage, such as dietary restriction of tyrosine and more intake of Vitamin C by its antioxidant effect.[12,15] Although the ochronotic arthropathy can severely handicap the patient because of its involvement in the spine and other joints, this incidence is quite rare. Earlier surgical intervention is needed when the ochronosis results in spinal cord dysfunction.
Conclusion
Ochronotic arthropathy can cause tandem spinal stenosis by thickening of abnormal ligamentum flavum which if overlooked can lead to serious complications. Simultaneous decompression procedure can be effective with emphasis on addressing cervical myelopathy as a first priority. Meticulous preoperative and intraoperative planning with expeditious implementation helps to achieve a successful outcome after a single simultaneous procedure. However, the only limitation of our report is a long-term follow-up, and more number of cases are essential to help guide treatment in such cases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- A patient with ochronotic arthropathy and spondylopathy: A difficult differential diagnosis with spondylitis ankylosans. Clin Exp Rheumatol. 1995;13:259-61.
- [Google Scholar]
- Osteoarthritis? Ochronotic arthritis! A case study and review of the literature. Knee Surg Sports Traumatol Arthrosc. 2009;17:778-81.
- [CrossRef] [PubMed] [Google Scholar]
- The clinical manifestations of ochronosis: A review. Acta Clin Belg. 1995;50:358-62.
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral hip arthroplasty for ochronotic arthropathy. Clin Rheumatol. 2000;19:150-2.
- [CrossRef] [PubMed] [Google Scholar]
- Ochronotic arthropathy: The black hip. Case report and review of the literature. Acta Orthop Belg. 1997;63:122-5.
- [Google Scholar]
- Tandem spinal stenosis: A systematic review. JBJS Rev. 2017;5:e2.
- [CrossRef] [PubMed] [Google Scholar]
- Ochronotic arthropathy: Rapid destructive hip osteoarthritis associated with metabolic disease. Clin Rheumatol. 1995;14:474-7.
- [CrossRef] [PubMed] [Google Scholar]
- Nickel-Catalyzed Generation of Schiff base Aluminum Enolate initiators for controlled methacrylate polymerization this work was supported by the engineering and physical sciences research council (UK) and ICI Acrylics (now Ineos Acrylics) Angew Chem Int Ed Engl. 2000;39:2141-4.
- [CrossRef] [PubMed] [Google Scholar]
- Compression of the cervical cord due to alkaptonuria arthropathy of the atlanto-axial joint. A case report. J Bone Joint Surg Am. 1995;77:274-7.
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral spontaneous rupture of the quadriceps tendon as an initial presentation of alkaptonuria - A case report. Knee. 2006;13:408-10.
- [CrossRef] [PubMed] [Google Scholar]
- Radiologic manifestations in alkaptonuria. Skeletal Radiol. 1984;11:204-8.
- [CrossRef] [PubMed] [Google Scholar]
- The pathology of alkaptonuric ochronosis. Hum Pathol. 1989;20:40-6.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of ascorbic acid in alkaptonuria: Alterations in benzoquinone acetic acid and an ontogenetic effect in infancy. Pediatr Res. 1989;26:140-4.
- [CrossRef] [PubMed] [Google Scholar]




