
Translate this page into:
Association of neck strength with upper femoral geometry and bone mineral density in postmenopausal women
Address for correspondence: Dr. Monika Gupta, Department of Pathology, Sree Balaji Medical College and Hospital, Chrompet, Chennai - 600 044, Tamil Nadu, India. E-mail: Monikagupta0703@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gupta M, Prabhu K, Ramesh M, Venketsh V. Association of neck strength with upper femoral geometry and bone mineral density in postmenopausal women. J Orthop Allied Sci 2016;4:65-8.
Abstract
Background:
Hip fracture is a severe health burden in the elderly population. In order to prevent, it is to evaluate the bone strength by establishing the relation between bone mineral density (BMD), neck strength, and geometry.
Materials and Methods:
The subjects under study were 100 postmenopausal women who visited bone clinic of Bharat Scan Centre. After recording general profile such as age, body mass index (BMI), geometric measures such as hip axis length (HAL), neck shaft angle (NSA), and neck width (NW) were measured from digital X-ray. For the same individuals, BMD was measured using dual energy X-ray absorptiometry (DXA) scan. From the DXA print out neck strength was calculated using the formula = sectional modulus/HAL.
Results:
The correlation test was analyzed among BMD, neck strength, anthropometric, and geometric factors using Statistical packages for social services (SPSS) software. BMD is inversely related with age and positively correlated with height, weight, and BMI. HAL, NSA, and NW had a weaker association with BMD. Age, BMD, and NSA had a negative relation with neck strength. HAL and NW had a positive relation with neck strength.
Conclusion:
Noninvasive means of associating neck strength with BMD and geometry will provide improved estimates for fracture risk beyond any other invasive method of assessing bone mineral properties.
Keywords
Bone mineral density
dual energy X-ray absorptiometry scan
neck strength
upper femoral geometry

Introduction
Hip fracture is the most serious age-related osteoporotic fracture. It is a severe health problem in the elderly population and in order to prevent it, is to evaluate the bone strength and establish the fracture risks.[1,2,3] The relation between bone mineral density (BMD) value and bone strength may show differences with structural properties, which is related with bone geometry.[4] Hence, several reports have suggested that the dimensions of proximal femoral geometry and anthropometric factors influence hip fracture risk.[5,6] From other studies hip axis length (HAL), neck shaft angle (NSA), and neck width (NW) are the most frequently cited to predict fracture risk.[5,6,7]
Bone mass, expressed as bone mineral content and BMD, has been shown to correlate with breaking strength of bone.[8] Hence, BMD is commonly equated with bone strength in the clinical prediction of fracture risk. The ability of the hip to bear functional loads is determined not only by the bone mass represented by BMD but also by material quality and distribution. Because BMD only partially discriminates individuals who will or will not fracture, we need to understand the geometry of the hip and its contribution to withstand the load.[9] The adult skeletal form is the product of an exquisite growth and developmental process, so understanding the strength of femoral neck structure will provide insights into adult pathologies and treatment.
Mechanical influences have been suggested to play a role in bone density than hormonal factors.[10] BMD and geometric properties determine bone mechanical strength and resistance to failure (fracture). Geometric properties and sectional modulus reflect both the amount and distribution of tissue in cancelous bone and correlate better with breaking strength than bone mineral properties alone. Geometry may be an overriding factor in determining bone strength. Thus, while bone mass alone does not fully discriminate those who will fracture from those who will not, incorporation of geometry and sectional modulus in clinical evaluation of skeletal status has been shown to enhance prediction of fracture risk.[7] In this study, an index of neck strength was formulated based on the bone strength index proposed by Selker and Carter by dividing the section modulus by the HAL (Z/HAL, cm2).[11] The section modulus Z, cm3 geometry-based indicator representing the strength of a section was calculated from the moment of inertia divided by half the bone width and association among BMD, neck strength, and geometric factors is established in this study.
Materials and Methods
This study was conducted on 100 postmenopausal women in the age group 50-60 years, who visited the bone clinic for screening of osteoporosis. The experimental procedure was approved by the Local Ethics Committee, and informed consent was obtained from all the participants. Exclusion criteria for the study were a hip fracture, any metabolic bone disease, or treatment with sex hormones, calcitonin. After recording general profile such as age, height, weight, and body mass index (BMI), geometric measures were taken from the digital X-ray, and BMD noticed from the dual energy X-ray absorptiometry (DXA) scan.
Proximal femur geometric measurements were performed directly on the X-rays manually in all the subjects. The evaluation was done on the left side of the hip in all the subjects. All the X-rays were taken when the hip joint was on neutral abduction and extension with foot rotated inside with 15 angles by knee or thesis. The following geometric measurements were taken.
Hip axial length (HAL) was measured as the linear distance from the base of trochanter to the apex of the ace tabular rim by aligning the ruler manually during the analysis procedure with the software provided and with the device as shown in Figure 1
Femoral NW was measured as the shortest distance within the femoral neck perpendicular to the femoral neck axis as shown in Figure 1
The angle between the HAL and shaft axis gives NSA as shown in Figure 1.
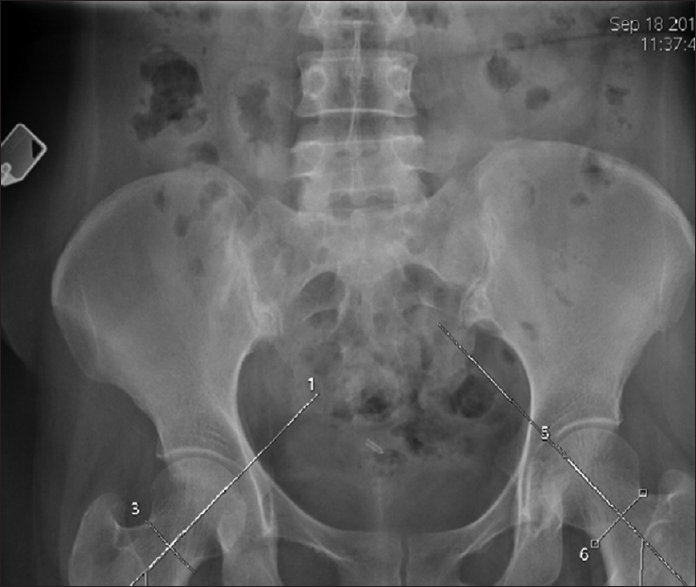
- The measurements of femoral geometry from digital X-ray
Proximal femur bone mineral density measurements
Lunar DXA was used for BMD measurements in the left side for the subjects. Total BMD were noticed from the DXA print out.
From the DXA print, the neck strength is calculated as follows. First, considering the neck of the femur as the rectangular lamina, a moment of inertia is calculated by using the formula. Moment of inertia (MI) MI = b (h3)/12, where b = breath of the neck, and h = length of the neck and moment of inertia of the curved lamina around the neck was MI = 0.11r4, where r = radius. As the neck is not true rectangle lamina, the value from the second equation should subtract from the value of second equation, and sectional modulus was calculated by using the formula, sectional modulus = 2 MI/W, where W = width of the neck. Therefore, the neck strength = sectional modulus/HAL. This value is representative of the bending force required to fracture the neck.
Results
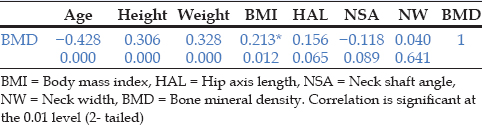
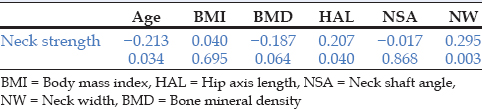
From the Table 1, the following results were inferred. BMD is inversely related with age and NSA and positively related with height, weight, BMI, and HAL. Table 2 shows that neck strength was inversely related with age and NSA and positively correlated with BMD HAL and NW.
Discussion
The occurrence of hip fracture may also be influenced by anthropometric factors.[12] Aging is one of the important reasons for hip fracture. It increases exponentially with age.[13,14] Another reason for hip fracture is low BMI because low BMI is related to lowered bone mass resulting in increased risk.
Although BMD correlates with geometric factors in our study, however, the literature on this topic does present a clear consensus. Controversies exist with the association of proximal femoral geometry such as HAL and NSA with the prediction of hip fracture risk. There is also finding that challenges the significance of HAL and even reported shorter HAL in fracture group. The HAL has been found to be correlated with BMD of control group rather in fracture group.[15] However, other results showed that each standard deviation increase in the HAL, it corresponds to a 2.3-fold increase in hip fracture risk. The precise physical mechanism in the relationship of HAL with fracture risk is unknown and but data from ex vivo biomechanical tests confirms positive correlation between HAL and femoral neck strength as in our study.[16] The relation of NSA with fracture risk is also debatable. The value varies among the published studies on fracture risk. In all studies except those of Cody et al.[17] computed tomography study in 1993 and Ferris et al. in 1989[18] (where hips were held in maximum internal rotation), the NSA is larger in the fracture - prone group as in our study. This is consistent with the hypothesis that generally these patients were imaged in a relatively externally rotated position given that external rotation increases apparent NSA.
However, in our study, DXA measurement was made in the neutral abduction and extension with foot rotated inside with 15 angles by knee or thesis. Hence, we conclude that a careful repositioning of the foot and leg is essential in monitoring changes in BMD longitudinally. In the present research, we also prepared a careful experimental design in measuring NSA. So our method of femoral NSA measurement is also reliable and measurements were précised. The precision is similar in the studies by Qureshi et al., 200 and Faulkner et al., and 1995.[7,19]
However, ex vivo biomechanical tests show that NSA does not correlate with femoral neck strength.[16] Hence, it correlation to fracture risk may involve other mechanism. It may be hypothesized that NSA or the anteversion angles interact with the direction of the fall, thus affecting the femoral neck loading angle. This angle, according to Pinilla et al., 1996 is inversely related to fracture load and its variation may, therefore, be associated with the different fracture.[20]
BMD alone cannot account for differences in mineral distribution and load bearing ability and is known to be insufficient for predicting fracture risk. BMD measurements do not specifically reflect attributes to three-dimensional geometry, trabecular microarchitecture, or intrinsic properties of the bone matrix, and appear to be only modest predictor's hip fractures. Hence, we suggested that structural parameters such as the cross-sectional moment of inertia and sectional modulus provide insight into the response of the femoral neck when a force is applied. In our study, it is inferred that HAL was correlated with sectional modulus, which determines the strength of the material.
Conclusion
We examined the series of normal adult subjects and found relationship between age and cross-sectional moment of inertia but did not fully examine other possible explanatory characteristics such as body mass and height. The difference observed in geometric properties of the femoral neck (reduction in moment of inertia and sectional modulus) demonstrate the importance of considering bone and shape as well as bone mass in evaluating bone strength. In addition, noninvasive means of measuring trabecular bone architecture may soon provide an additional level of insight for screening although the methodology is currently insufficient. There are likely to be additional attributes that are discovered from ongoing basic science research that correlate with fracture risk. However, it is unclear whether these methods provide improved estimates for risk assessment beyond that of BMD and geometry.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Hip fracture risk and proximal femur geometry from DXA scans. Osteoporos Int. 2002;13:542-50.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term prediction of incident hip frahcture risk in elderly white women: Study of osteoporotic fractures. J Am Geriatr Soc. 2004;52:1479-86.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal history of osteoporosis and femur geometry. Calcif Tissue Int. 2004;75:277-85.
- [CrossRef] [PubMed] [Google Scholar]
- Measurement of femoral geometry in type I and type II osteoporosis: Differences in hip axis length consistent with heterogeneity in the pathogenesis of osteoporotic fractures. J Bone Miner Res. 1995;10:1908-12.
- [CrossRef] [PubMed] [Google Scholar]
- Simple measurement of femoral geometry predicts hip fracture: The study of osteoporotic fractures. J Bone Miner Res. 1993;8:1211-7.
- [CrossRef] [PubMed] [Google Scholar]
- Better discrimination of hip fracture using bone density, geometry and architecture. Osteoporos Int. 1995;5:167-73.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical competence of vertebral trabecular bone in relation to ash density and age in normal individuals. Bone. 1987;8:79-85.
- [CrossRef] [PubMed] [Google Scholar]
- Curved beam model of the proximal femur for estimating stress using dual-energy X-ray absorptiometry derived structural geometry. J Orthop Res. 1996;14:483-92.
- [CrossRef] [PubMed] [Google Scholar]
- Age-related changes in cortical and cancellous vertebral bone density in girls: Assessment with quantitative CT. AJR Am J Roentgenol. 1994;162:405-9.
- [CrossRef] [PubMed] [Google Scholar]
- Scaling of long bone fracture strength with animal mass. J Biomech. 1989;22:1175-83.
- [CrossRef] [PubMed] [Google Scholar]
- Anthropometric indicators and hip fracture. The NHANES I epidemiologic follow-up study. J Am Geriatr Soc. 1989;37:9-16.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of hip fractures: Implications of the exponential increase with age. Bone. 1996;18(3 Suppl):121S-5S.
- [CrossRef] [PubMed] [Google Scholar]
- The association of proximal femur geometry with hip fracture risk. Clin Anat. 2008;21:575-80.
- [CrossRef] [PubMed] [Google Scholar]
- International variation in the incidence of hip fractures: Cross-national project on osteoporosis for the World Health Organization Program for Research on Aging. Osteoporos Int. 1999;9:242-53.
- [CrossRef] [PubMed] [Google Scholar]
- Does bone density or bone shape discriminate between subjects at high and low risk of hip fracture? Proceedings of the Thirty - Ninth Annual Meeting of the Orthopaedic Research Society, San Francisco, CA; 1993. :19.
- [Google Scholar]
- Morphology of the femur in proximal femoral fractures. J Bone Joint Surg Br. 1989;71:475-7.
- [CrossRef] [PubMed] [Google Scholar]
- Association between COLIA1 Sp1 alleles and femoral neck geometry. Calcif Tissue Int. 2001;69:67-72.
- [CrossRef] [PubMed] [Google Scholar]
- Impact direction from a fall influences the failure load of the proximal femur as much as age-related bone loss. Calcif Tissue Int. 1996;58:231-5.
- [CrossRef] [PubMed] [Google Scholar]




