
Translate this page into:
Arthroscopic treatment of isolated type 2 SLAP lesions in athletes: A systematic review
Address for correspondence: Dr. Atul Mahajan, Dr. Mahajan's Bone and Joint Clinic, New Delhi, China. E-mail: dratulmahajan84@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Mahajan A, Wong D. Arthroscopic treatment of isolated type 2 SLAP lesions in athletes: A systematic review. J Orthop Spine 2019;7:40-5.
Abstract
Superior Labrum From Anterior to Posterior (SLAP) lesions refer to a tear of the superior portion of the glenoid labrum that begins posteriorly and extends anteriorly to the mid-glenoid notch. Patients who sustain traumatic injuries to the shoulder girdle and also who undergo repetitive, overhead motions are at risk for SLAP lesions. Among the various types of SLAP lesions, type 2 lesion is the most common lesion encountered and is defined by 'superior labral fraying with stripping of the superior part of the labrum and attached biceps tendon from the underlying glenoid cartilage”. In superior labrum anterior and posterior (SLAP) tears, a common concern for patients is being able to return to their previous levels of activity after surgery, whereas clinicians are concerned with providing a consistent prognosis of successful return to participation after surgery. Thus, return to play (RTP) and patient satisfaction can be used as a vital measure of treatment success which has been evaluated by significantly fewer studies, especially in isolated type 2 SLAP repairs. The published outcomes of surgical treatment are inconsistent, with variable and suboptimal patient satisfaction rates and RTP. Thus, we wanted to address and reevaluate the current treatment, rehabilitation protocols, and outcome following arthroscopic repairs in order to expand the knowledge and give further insight into providing better management plan in these patients. This study used a systematic review of papers reporting arthroscopic treatment of isolated type 2 SLAP lesions with the main objective in trying to assess the effectiveness of arthroscopic repair, to determine patient satisfaction and RTP at previous level of activity, and to analyze the rehabilitation protocols being followed among all athletes who underwent repair of type 2 SLAP tears using various types of fixation.
Keywords
Arthroscopic
labrum
peel-back phenomenon
superior labrum anterior to posterior

Introduction
Superior labrum from anterior to posterior (SLAP) lesions, first described by Andrews et al. and Snyder et al.,[1,2] refer to a tear of the superior portion of the glenoid labrum that begins posteriorly and extends anteriorly to the mid-glenoid notch. Patients who sustain traumatic injuries to the shoulder girdle and also who undergo repetitive, overhead motions are at risk for SLAP lesions.
Impaction of the humeral head against the superior labrum and the biceps anchor due to fall onto an outstretched arm with the shoulder positioned in abduction and flexion is the most common mechanism in acute traumatic episodes, whereas a “peel-back” mechanism in overhead athletes has been proposed by Burkhart and Morgan,[3,4] which requires repetitive minor trauma to the superior labrum.
Patients usually present with pain, especially with overhead activity, and experience a popping sensation in the shoulder. Conservative management, consisting of rest and activity modification, anti-inflammatory medications, and physical therapy, should be initially attempted in most SLAP injuries. If conservative therapy is unsuccessful, surgical options involving arthroscopic management of the tears can be tried. A classification system including four SLAP lesions [2] has been described which has been expanded by Maffet et al.[5] to include seven defined types.
Among the various types of SLAP lesions, type 2 lesion is the most common lesion encountered and is defined by 'superior labral fraying with stripping of the superior part of the labrum and attached biceps tendon from the underlying glenoid cartilage”.[6,7] Morgan et al.[8] have further identified three distinct subtypes of type 2 SLAP lesions (type 2A, 2B, and 2C). In particular, type 2A, 2B, and 2C represent anterosuperior labral lesion, posterosuperior lesion, and superior lesion with both anterior and posterior components, respectively.
In superior labrum anterior and posterior (SLAP) tears, a common concern for patients is being able to return to their previous levels of activity after surgery, whereas clinicians are concerned with providing a consistent prognosis of successful return to participation after surgery. Thus, return to play (RTP) and patient satisfaction can be used as a vital measure of treatment success which has been evaluated by significantly fewer studies, especially in isolated type 2 SLAP repairs.
The published outcomes of surgical treatment are inconsistent, with variable and suboptimal patient satisfaction rates and RTP. Thus, we wanted to address and reevaluate the current treatment, rehabilitation protocols, and outcome following arthroscopic repairs in order to expand the knowledge and give further insight into providing better management plan in these patients.
This study used a systematic review of papers reporting arthroscopic treatment of isolated type 2 SLAP lesions with the main objective in trying to assess the effectiveness of arthroscopic repair, to determine patient satisfaction and RTP at previous level of activity, and to analyze the rehabilitation protocols being followed among all athletes who underwent repair of type 2 SLAP tears using various types of fixation.
Materials and Methods
Articles were retrieved by an electronic search of Medical Subject Headings and keyword terms and their respective combinations. We conducted a systematic Internet search of PubMed, Ovid, and Cochrane Library databases for type 2 SLAP repairs between January 1, 1950, and March 31, 2018. Database search terms included “SLAP” OR “superior labrum anterior and posterior” OR “type 2 SLAP” OR “SLAP outcome.”
Inclusion criteria included outcome studies of repair of type 2 SLAP lesions with minimum 2-year follow-up and patient population with a mean age of <40 years. Additional inclusion criteria included English language studies with Level IV or higher evidence. We excluded articles if the type of labral lesion repaired was not identified. We excluded animal, biomechanical, cadaveric studies, studies reporting outcomes on only combined lesions, and studies that took into account salvage options for failed SLAP repair.
The initial title search yielded a subset of possible articles that were then further included or excluded according to the contents of the article's abstract, and articles were chosen based on the set inclusion and exclusion criteria. The full text was reviewed of articles selected in both the title and abstract phases. In addition, the reference sections from articles undergoing full-text review were scanned to identify any additional studies that were not identified from the original literature search. Studies for the final inclusion were then selected at this stage. All selected studies [Figure 1] were analyzed for inclusion or exclusion by consensus and discussion with the senior author. For some studies, individual patients were excluded based on exclusion criteria, whereas the remaining patients were included in the analysis.

- Flowchart illustrating the method for selection of articles for review
Several parameters were collected from the final selected studies. These included level of evidence, number of patients, mean patient age, gender, shoulder dominance, follow-up time, type of SLAP tear, traumatic or atraumatic onset, complications following surgery, postoperative outcomes, or patient satisfaction details. Data extraction also included type of fixation, patient's activity levels, patient satisfaction (graded as “good to excellent,” “fair,” or “poor” based on specific outcome scale used), and return to the previous level of play.
The description of the surgical technique was also analyzed for multiple aspects that are integral to the surgery and can affect the technical completeness of the repair. Furthermore, analyzed were the details of the followed rehabilitation protocols. We specifically looked for details of immobilization in a sling, shoulder range of motion (ROM) exercises, strengthening exercises, and return to activity following surgery.
Results
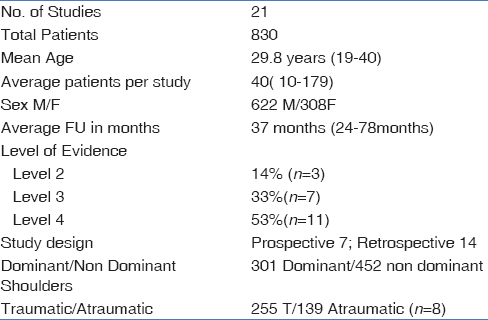
The systemic review included 21 studies [Table 1]. The mean number of patients in each study was 40 (range: 10–179) at baseline. The mean age at surgery was 29.8 years (range: 19–40 years), and the mean follow-up period was 37 months (range: 24–78 months). In total, 830 patients underwent arthroscopic repair for isolated type 2 SLAP injury. The levels of evidence of the 21 studies included 14% (n = 3) of Level II studies, 33% (n = 7) of Level III studies, and 53% (n = 11) of Level IV studies. Seven studies were prospective, whereas 14 studies were retrospective in design. Eleven studies had overhead athletes as their study group and 320 patients were confirmed involved in overhead activity before injury. Seventy-five percent of the population were male, whereas the rest were female (gender split M/F = 622/308). Dominant shoulders were involved in 40% of patients (n = 11 studies; dominant/nondominant shoulder = 301/452).
Return to play
Of the 21 studies, 57% (n = 12) reported whether patients returned to play or activity after SLAP repair. The proportion of athletes who returned to their preinjury levels of participation after isolated type 2 superior labral repair was reported to range from 48% to 100% for the 12 studies reviewed. The mean percent RTP of reviewed studies was 75%. Six studies analyzed overhead athletes and RTP for these patients was 70% (range = 22%–100%).
Function-related outcome scores
Each study was assessed for the inclusion of functional outcomes scores with respect to frequency of reporting. Of the validated functional outcomes, the American Shoulder and Elbow Surgeons (ASES) score was most often used and reported in 57% (n = 12) of studies. University of California Los Angeles shoulder score (UCLA) in 29% (n = 6). The Western Ontario Shoulder Instability Index (WOSI), Kerlan-Jobe Orthopaedic Clinic score (KJOC), and constant scores were used in 14% (n = 3) of studies. L'Insalata and Rowe scores were used in 10% (n = 2) of studies. The mean ASES score at the final follow-up was 90.6, whereas the mean UCLA scores were 31.5. The mean KJOC scores at the final follow-up were 76.55. Patient satisfaction was specifically documented in 71% (n = 15) of studies. Good–excellent outcomes were reported in 82.4% of the patients [Figure 2].
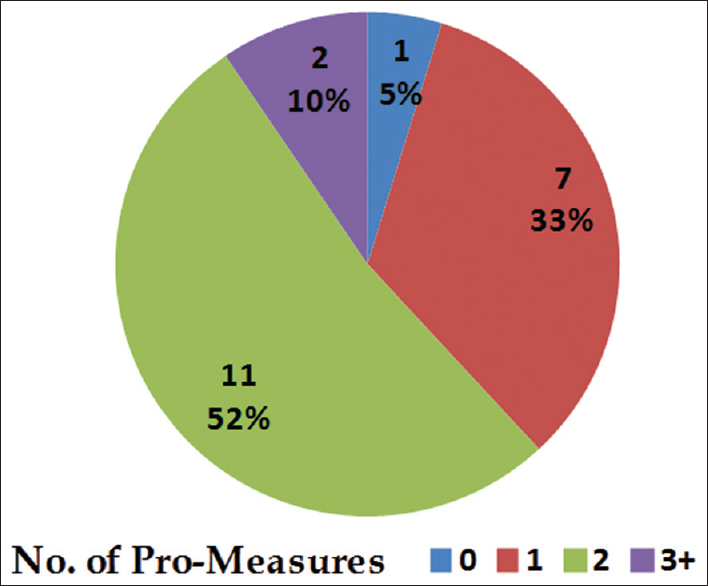
- Number of Patient related outcomes (PROs) reported in the included studies in the review
Comparison between overhead and nonoverhead athletes
Subset analysis between overhead and nonoverhead athletes [Table 2] revealed some interesting findings. Six studies analyzed overhead athletes and RTP for these patients was 70% (range = 22%–100%) The mean RTP for nonover head athletes was higher (75.6%) compared to overhead athletes. Good–excellent outcomes were reported in 87.8% of the overhead athletes, whereas it was 79% for nonoverhead athletes.

Comparison between different methods of fixation
Seventeen studies used suture anchors as method of fixation, whereas three studies used tacks as method of fixation [Table 3]. One study used both suture anchors and tacks as method of fixation. Six studies reported on number of anchors used. The mean number of anchors used was 1.96. Subset analysis revealed that the “good-to-excellent” satisfaction rates were higher for anchor fixation (84.5%) than for tack fixation (76%, P < 0.05). However, anchor repair in athletes resulted in a comparable percentage of RTP (78% versus 77.25%) compared with tack repair.

Rehabilitation protocols
Eightone percent of studies (n = 17) had followed a specific rehabilitation protocol for their subset of patients. [Figure 3] Most of the studies immobilized in arm sling following surgery, whereas three studies allowed their patients' passive- and active-assisted ROM exercises from day 1 onward. RTP for most of the studies was at 6 months onward, whereas three studies allowed RTP from 4 months onward.
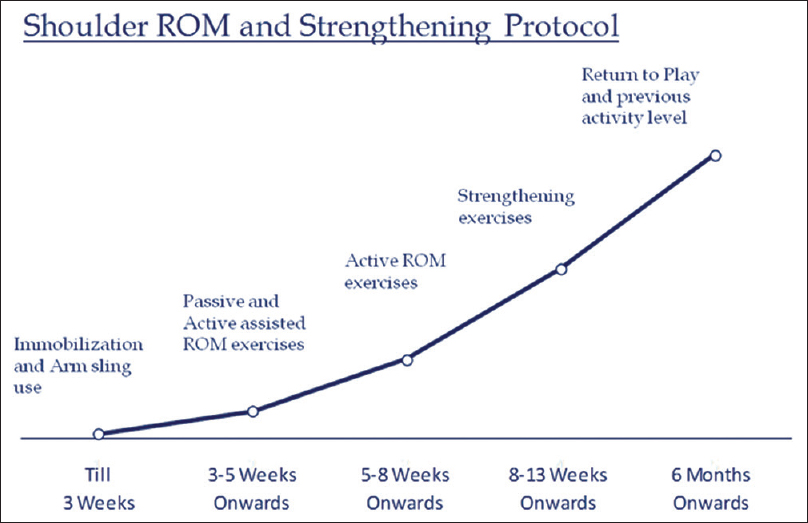
- Shoulder Rehabilitation Protocol Followed following Surgery
Complications reported
Ten studies reported pain at the final follow-up and 18% of patients had pain at the final follow-up. Six studies reported incidence of revision surgery and 12% of patients had to undergo revision surgery related to SLAP repair. Four studies reported incidence of stiffness and 9% of patients had stiffness at the final follow-up.
Discussion
Type 2 SLAP lesions are characterized by the combined detachment of the superior labrum and biceps tendon from the peripheral edge of the glenoid. In SLAP tears, a common concern for patients is being able to return to their previous levels of activity after surgery, whereas clinicians are concerned with providing a consistent prognosis of successful return to participation after surgery. Thus, RTP and patient satisfaction can be used as a vital measure of treatment success which has been evaluated by significantly fewer studies, especially in isolated type 2 SLAP repairs.
Most of the studies that have been done are from single institutions and lack the power necessary to definitively draw conclusions. Furthermore, there exists variation in patient populations, diagnostic techniques, and measurement of outcomes following surgery, Also, there is little information provided on the criteria to determine the outcome following the repair. Rehabiliatation protocols followed are minimally reported as well. The lack of reported information, and lack of consensus reflect an underlying imprecision in the treatment of SLAP lesions and have adverse implications. Thus, pooling data from multiple studies is important to evaluate and determine the appropriateness of treatment currently being offered and also to assess the outcomes following repair of these injuries.
This study used a systematic review of papers reporting arthroscopic treatment of isolated type 2 SLAP lesions with the main objective in trying to assess the effectiveness of arthroscopic repair, to determine patient satisfaction and RTP at previous level of activity, and to analyze the rehabilitation protocols being followed among all athletes who underwent repair of type 2 SLAP tears using various types of fixation.
We included 21 studies in this study, with a mean age of patients being 30 years with a range from 19 to 40 years. This range of ages indicated that the reported return-to-participation rates cannot be extrapolated to younger age groups, which is a concern because younger athletes have a greater chance of advancing to competitive sports participation than older athletes. If operative intervention is recommended for a younger athlete, supplying preoperative return-to-participation prognoses may be helpful in determining if undergoing the corrective procedure will allow return to the current level of activity and advancement to higher stages of participation. However, it is possible that factors beyond patient age, such as variations in healing rates, skill levels, financial considerations, and internal or external motivators, can influence the decision to have surgery.[9-11]
The average follow-up period was around 37 months. This was because we believe that a minimum 2-year follow-up is necessary for this injury to allow adequate time for return to a full season of sports and that shorter follow-up may not represent true outcome of repair.
Seven studies were prospective, whereas majority (14 studies) were retrospective in nature. Thus, the majority of studies lacked a high level of evidence, making it difficult to determine the true outcome and most effective options.
Of the 21 studies, 12 studies reported whether patients returned to play or activity after SLAP repair. The proportion of athletes who returned to their preinjury levels of participation after isolated type 2 superior labral repair was reported to range from 48% to 100% for the 12 studies reviewed. The mean percent RTP of reviewed studies was 75%. Six studies analyzed overhead athletes and RTP for these patients was 70% (range = 22%–100%).
Each study was assessed for the inclusion of functional outcomes scores with respect to frequency of reporting. ASES score was most often used in 57% (n = 12), followed by the UCLA score in 29% (n = 6). WOSI, KJOC, and Constant Scores were used in 14% (n = 3) of studies. L'Insalata and Rowe scores were used in 10% (n = 2) of studies. The mean ASES score at the final follow-up was 90.6, whereas the mean UCLA score was 31.5. The mean KJOC score at the final follow-up was 76.55. Patient satisfaction was specifically documented in 71% (n = 15) of studies. Good–excellent outcomes were reported in 82.4% of the patients.
Neuman et al.[12] analyzed 30 overhead athletes, who underwent type 2 SLAP repair, finding that 84% of patients were able to return to their previous level of play after <12 months with 93% of good-to-excellent results. The authors also showed that KJOC score is a more specific scoring system for throwing athletes and better correlates to return to the previous level of play in overhead athletes.
These relatively high and similar mean scores show the importance of including several types of outcome measure, including activity measures and RTP data. The shoulder score results reflected better outcomes than the RTP data, thus emphasizing this point.
Comparison between overhead and nonoverhead athletes
Overhead athletes are the most challenging to return to the previous level of performance for this diagnosis, and their return rate reflects this. Subset analysis between overhead and nonoverhead athletes revealed some interesting findings. Six studies analyzed overhead athletes and RTP for these patients was 70% (range = 22%–100%). The mean RTP for nonover head athletes was higher (75.6%) compared to overhead athletes. However, good–excellent outcomes were reported in 87.8% of the overhead athletes, whereas it was 79% for nonoverhead athletes.
Kim et al.[13] in a retrospective case series examined the results of arthroscopic repair of isolated type 2 SLAP lesions using metal suture anchors. The study group consists of 34 patients with 18 of them overhead athletes. Patients' postoperative UCLA scores significantly increased to 33.4, but overhead athletes showed lower results (32.6 on average). Good-to-excellent results and return to sports were found in 89% of overhead sports athletes, and 76% of whom were able to perform their previous sports without limitations.
Cohen et al.[14] retrospectively examined the results of arthroscopic repair of isolated type 2 SLAP tears using bioabsorbable tacks in 37 males with 29 athletes, and the mean age was 34 years. ASES and L'Insalata scores were used to evaluate outcomes at the final follow-up. That surgical treatment led to 69% of excellent-to-good results, but overhead athletes had a worse L'Insalata score than other patients, and only 38% of them could RTP.
Rhee et al.,[15] conversely, found that athletes had higher results than nonathletes and throwing ones scored better than nonthrowing. The authors noted that the low outcome scores of the nonthrowers might be attributed to the fact that gymnasts, who have a higher rate of repetitive injuries, represented more than a half of their nonthrowing study group.
In the study by Friel et al.,[16] the subgroup analysis of overhead athletes versus nonathletes showed preoperative to postoperative improvements in both the groups, with overhead laborers achieving better functional outcomes and nonlaborers achieving greater reduction of pain, suggesting that SLAP type 2 repair is successful independent of the patient's vocation or sports.
Yung et al.[17] suggested that overhead athletes who return to their preinjury level of play may need a longer course of rehabilitation than other patients before returning to competition. These results show the necessity of reporting baseball players' and throwing athletes' results as a separate subset when describing the outcome for type 2 SLAP repairs.
Comparison between different methods of fixation
Seventeen studies used suture anchors as method of fixation, whereas three studies used tacks as method of fixation. One study used both suture anchors and tacks as method of fixation. Only 28% (n = 6) of studies reported on number of anchors used. The mean number of anchors used was 1.96. The number of anchors used is known to be an important technical component. Multipoint fixation achieved using multiple individual anchors is known to improve labral stability,[18] and a double-loaded anchor still only results in single-point fixation of bony attachment. An inadequate attachment footprint on the glenoid will not generate adequate healing.
Cohen et al.[14] found that the outcomes of bioabsorbable tack fixation in throwing athletes were significantly inferior to those in nonthrowing athletes (38% vs. 71% of good-to-excellent results). This likely depends on the lack of strength of this device, which completely loses its mechanical role after a month, providing no more fixation for the healing of labrum, especially in the posterior superior glenoid where bone may be less dense.
Rehabilitation protocols
Eighty-one percent of studies (n = 17) had followed a specific rehabilitation protocol for their subset of patients. Most of the studies immobilized in arm sling following surgery, whereas three studies allowed their patients' passive- and active-assisted ROM exercises from day 1 onward. RTP for most of the studies was at 6 months onward, whereas three studies allowed RTP from 4 months onward. The postoperative rehabilitation guidelines that were reported for each study were consistent in design where progressive strengthening and ROM exercises were used throughout the rehabilitation process.
However, the majority of studies failed to report the critical details of the rehabilitation program, including the specific exercises used for each component (kinetic chain, scapula, and shoulder), progression through the rehabilitation phases, patient compliance with the protocol, the duration (total number of visits) or frequency of rehabilitation, or use of a home program.
Ten studies reported pain at the final follow-up and 18% of patients had pain at the final follow-up. Six studies reported incidence of revision surgery and 12% of patients had to undergo revision surgery related to SLAP repair. Four studies reported incidence of stiffness and 9% of patients had stiffness at the final follow-up.
Conclusion
The current practice of treating SLAP lesions is controversial, some of which results from imprecision in the treatment. After this systematic review, We can conclude that arthroscopic repair of type 2 SLAP tears results in overall better outcome for individuals not involved in throwing or overhead sports. The results of type 2 SLAP repair in throwing or overhead athletes are much less predictable, especially when return to the previous level of performance is the criterion for success. Future studies should be prospective in nature to determine predictors of outcome. Reporting of outcomes at a minimum must include validated shoulder outcome measures, validated activity scales, and RTP data. The outcomes must be reported separately for throwing and nonthrowing athletes. Efforts should be directed toward improving consistency in documenting and reporting surgical indications, techniques, endpoints, and rehabilitation protocols to provide a basis for consensus regarding optimal treatment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13:337-41.
- [CrossRef] [PubMed] [Google Scholar]
- The peel-back mechanism: Its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair rehabilitation. Arthroscopy. 1998;14:637-40.
- [CrossRef] [PubMed] [Google Scholar]
- Superior labral strain during the throwing motion. A cadaveric study. Am J Sports Med. 2001;29:488-92.
- [CrossRef] [PubMed] [Google Scholar]
- Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med. 1995;23:93-8.
- [CrossRef] [PubMed] [Google Scholar]
- Foreign-body reaction to the bioabsorbable suretac device. Arthroscopy. 2000;16:91-5.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic repair of superior glenoid labral detachment (the SLAP lesion) J Shoulder Elbow Surg. 1993;2:147-55.
- [CrossRef] [PubMed] [Google Scholar]
- Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998;14:553-65.
- [CrossRef] [PubMed] [Google Scholar]
- Return-to-play in sport: A decision-based model. Clin J Sport Med. 2010;20:379-85.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic evaluation of meniscal repairs. Factors that effect healing. Am J Sports Med. 1994;22:797-802.
- [CrossRef] [PubMed] [Google Scholar]
- A radiographic assessment of pediatric fracture healing and time since injury. J Forensic Sci. 2011;56:1123-30.
- [CrossRef] [PubMed] [Google Scholar]
- Results of arthroscopic repair of type II superior labral anterior posterior lesions in overhead athletes: Assessment of return to preinjury playing level and satisfaction. Am J Sports Med. 2011;39:1883-8.
- [CrossRef] [PubMed] [Google Scholar]
- Results of arthroscopic treatment of superior labral lesions. J Bone Joint Surg Am. 2002;84:981-5.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes of isolated type II SLAP lesions treated with arthroscopic fixation using a bioabsorbable tack. Arthroscopy. 2006;22:136-42.
- [CrossRef] [PubMed] [Google Scholar]
- Unstable isolated SLAP lesion: Clinical presentation and outcome of arthroscopic fixation. Arthroscopy. 2005;21:1099.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes of type II superior labrum, anterior to posterior (SLAP) repair: Prospective evaluation at a minimum two-year follow-up. J Shoulder Elbow Surg. 2010;19:859-67.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic repair of isolated type II superior labrum anterior-posterior lesion. Knee Surg Sports Traumatol Arthrosc. 2008;16:1151-7.
- [CrossRef] [PubMed] [Google Scholar]
- Footprint contact restoration between the biceps-labrum complex and the glenoid rim in SLAP repair: A comparative cadaveric study using pressure-sensitive film. Arthroscopy. 2013;29:1005-11.
- [CrossRef] [PubMed] [Google Scholar]




