
Translate this page into:
Arthroscopic reconstruction of anterior cruciate ligament: 4-strand versus 5-strand hamstring autograft
Address for correspondence: Dr. Bhuwan Sharma, Department of Community Medicine, PIMS Medical College, Garah Road, Near Bust Stand, Jalandhar 144001, India. E-mail: dr.bhuwansharma@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Goyal C, Ajrawat SS, Mal JJ, Sharma B. Arthroscopic reconstruction of anterior cruciate ligament: 4-strand versus 5-strand hamstring autograft. J Orthop Spine 2022;10:73-7.
Abstract
INTRODUCTION:
In present study, we aimed to compare the functional outcome after 4-strand versus 5-strand hamstring autograft for anterior crucial ligament reconstruction using Tegner Lysholm score.
MATERIALS AND METHODS:
Study included 70 cases (35 in each group) of complete anterior cruciate ligament tear confirmed radiologically on MRI. After doing anterior cruciate ligament reconstruction with 4- and 5-strand hamstrings autograft, the patients were assessed for the functional outcome using Tegner Lysholm score at post-operative interval of 3, 6 and 9 months. Data were analyzed using SPSS software version 21.
RESULTS:
Tegner Lysholm score at baseline was 41.63 and 42.01 in 4- and 5-strand group which increased progressively to 93.45 and 85.13 at the end of 9 months. The improvement was significantly more in 5-strand group (P < 0.05). Overall, at the end of follow-up, excellent results were seen in 71.4% versus 60% patients while good to fair results were seen in 20% versus 28.6% and 8.6% versus 8.6% patients in 4- and 5-strand groups, respectively. Poor outcome in terms of revision surgery was required in one case (2.9%) of 4-strand group.
CONCLUSION:
Study concluded that single 5-strand graft offers good functional outcome in cases of anterior crucial ligament reconstruction. A 5-strand hamstring graft provides an increase in diameter than 4-strand graft, which leads to stronger graft and reduced revision rate. It is especially useful in the cases of undersized hamstring graft or stability issues.
Keywords
Anterior cruciate ligament
arthroscopic repair
hamstring 4-strand graft
hamstring 5-strand graft
hamstring autograft
tegner lysholm score

Introduction
Anterior cruciate ligament (ACL) is a ligament of knee joint. It is major stabilizer of knee joint and prevents anterior tibial displacement. The ligament passes from medial part of intercondylar area of tibia upward, backward, and laterally to insert into the posterior part of medial surface of the lateral femoral condyle. Anterior cruciate ligament injury remains a common orthopedic problem and is often associated with meniscal pathology.[1] These tears can occur during the initial traumatic event, or subsequently over time due to altered biomechanics and the ongoing instability it causes. It has been established that standard of care for ACL injury is ligament reconstruction aiming to halt or minimize the number of instability episodes.[2]
The ultimate goal of ACL reconstruction is to restore normal knee kinematics in patients with functionally unstable ACL deficient knees. ACL reconstructions fail at a rate which is small but not insignificant. Despite advances, failure rate after ACLR ranges from 0.7% to 10%.[3]
Four-strand hamstring autograft is a common choice for anterior cruciate ligament (ACL) reconstruction. Advocates for its use cite a decreased potential for catastrophic extensor mechanism complications and a decreased incidence of anterior knee pain associated with central-third bone–patellar tendon–bone (BPTB) autograft. In addition, biomechanical testing of 4-strand gracilis and semitendinosus autograft has shown a higher load to failure than that with BPTB autograft.[4,5] Most importantly, clinical outcomes have been equivalent using 4-strand hamstring autograft and using BPTB autograft.[6]
A potential disadvantage of hamstring autograft for ACL reconstruction is the inherent variability in graft diameter. Biomechanical testing has shown a correlation between graft cross-sectional area and maximum load to failure. Even in the highest stability four-strand hamstring (4HS) ACL reconstruction series side-to-side differences of >2 mm are generally seen in at least a third of all knees. Historically, authors have recommended the use of grafts at least 7 mm in diameter, although limited evidence supports this recommendation.[4,7,8]
Prodromos et al.[9] hypothesized that a stronger, stiffer 5-strand HS graft would result in higher stability rates than 4HS graft. Their study concluded that 5HS ACL reconstruction had higher stability than a high stability 4HS cohort. Thus, 5HS is preferable to 4HS for ACL reconstruction, especially for double bundle techniques. Later similar results were also obtained by Lavery et al.[10]
However not much literature is available in our country regarding the functional outcome after 5-stranded hamstring graft. The present study was thus conducted to evaluate and compare the functional outcome of single bundle 4- versus 5-strand hamstring autograft for anterior crucial ligament repair, using Lysholm Tegner score.[11]
Materials and Methods
A prospective, observational study was conducted at the Department of Orthopedics of a tertiary care center. Study included a total of 70 cases of complete anterior cruciate ligament tear confirmed radiologically on MRI after informed consent. Cases with infections or any lesion over the skin, multi-ligament injury, revision surgery of ACL and associated lower limb fractures were excluded. Cases were randomly allocated using computer-generated random numbers to undergo either 4- or 5-strand grafting.
For all the patients, detailed clinical history, complete general, systemic examination, local examination, and preoperative investigation findings were noted in a pre-designed proforma. After doing anterior cruciate ligament reconstruction with 4- or 5-strand hamstrings autograft, the patients were assessed for the functional outcome using Lysholm Tegner score at post-operative interval of 3, 6, and 9 months.
To study the post-operative complications of procedure the patients were assessed immediately after surgery at 24 h, 48 h, and 5th day and on subsequent schedule follow-up. The study participants were informed to report to health facility as and when required apart from scheduled visit.
The quantitative data were represented as their mean ± SD. Categorical and nominal data were expressed in percentage. All analysis were carried out by using SPSS software version 21.
Operative procedure
5-strand graft
First, one end of the semitendinosus tendon is tied to the EndoButton loop using the free tails from its running, locking stitch by non-absorbable ultrabraid sutures [Figure 1a]. These suture tails are left intact because they will be used later to suture two of the semitendinosus strands together. The opposite, free end of the semitendinosus is then brought through the EndoButton loop to create three equal-length tendon strands [Figure 1b]. The preserved suture limbs previously used to secure the end of semitendinosus to the EndoButton loop are used to secure the two gracilis graft strands connected by a tendon loop distally away from the EndoButton [Figure 1c]. The gracilis tendon is brought through the EndoButtonloop, bisecting this in standard fashion, and the 5-strand graft is completed [Figure 1d].
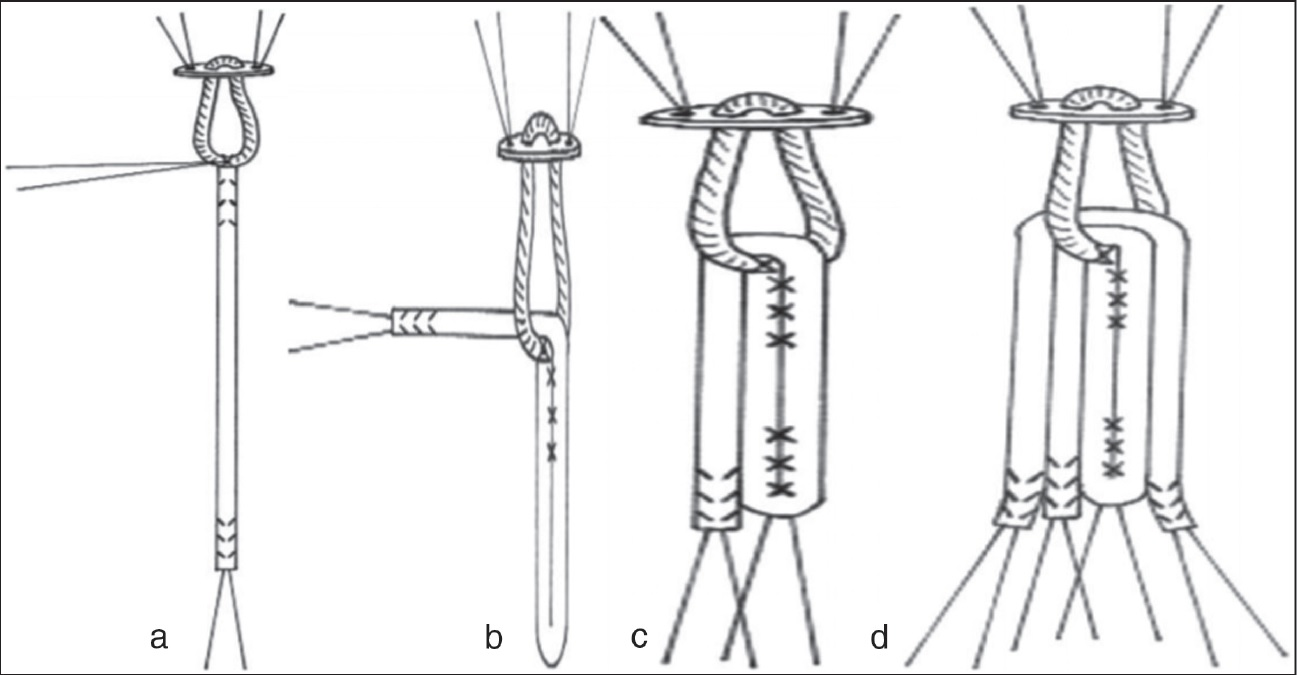
- (a–d) Preparation of 5-strand hamstring graft
Four-strand graft
A whipstitch was placed at both ends of each tendon with nonabsorbable ultrabraid sutures. The gracilis and semitendinosus (two each) tendons were then looped around the suture to form the 4-strand hamstring graft.
Results
Mean age of the study cases was 34.12 ± 4.7 years with 85.7% males. Most common mechanism of injury for ACL tear was sports injury (40%) followed by RTA (34.3%) and domestic injuries due to fall (25.7%). Mean graft size was 9.12 ± 0.60 mm in 5-strand group while it was 8.17 ± 0.41 mm in 4-strand group (P < 0.01). Tegner Lysholm score at baseline was 41.63 and 42.01 in 4- and 5-strand groups which increased progressively to 93.45 and 85.13 at the end of 9 months. The improvement was significantly more in 5-strand group (P < 0.05) [Figure 2]. Prior to treatment, all the cases were in poor grade as per Lysholm score (i.e., having significant knee problems). Overall, at the end of follow-up, excellent results were seen in 71.4% versus 60% patients while good to fair results were seen in 20% versus 28.6% and 8.6% versus 8.6% patients in 4- and 5-strand groups, respectively. Poor outcome in terms of revision surgery was required in one case (2.9%) of 4-strand group [Figure 3]. Superficial infections were seen in three cases each (8.6%) while complaint of knee pain was given by 1 (2.9%) case of 4-strand group and none in 5-strand group.
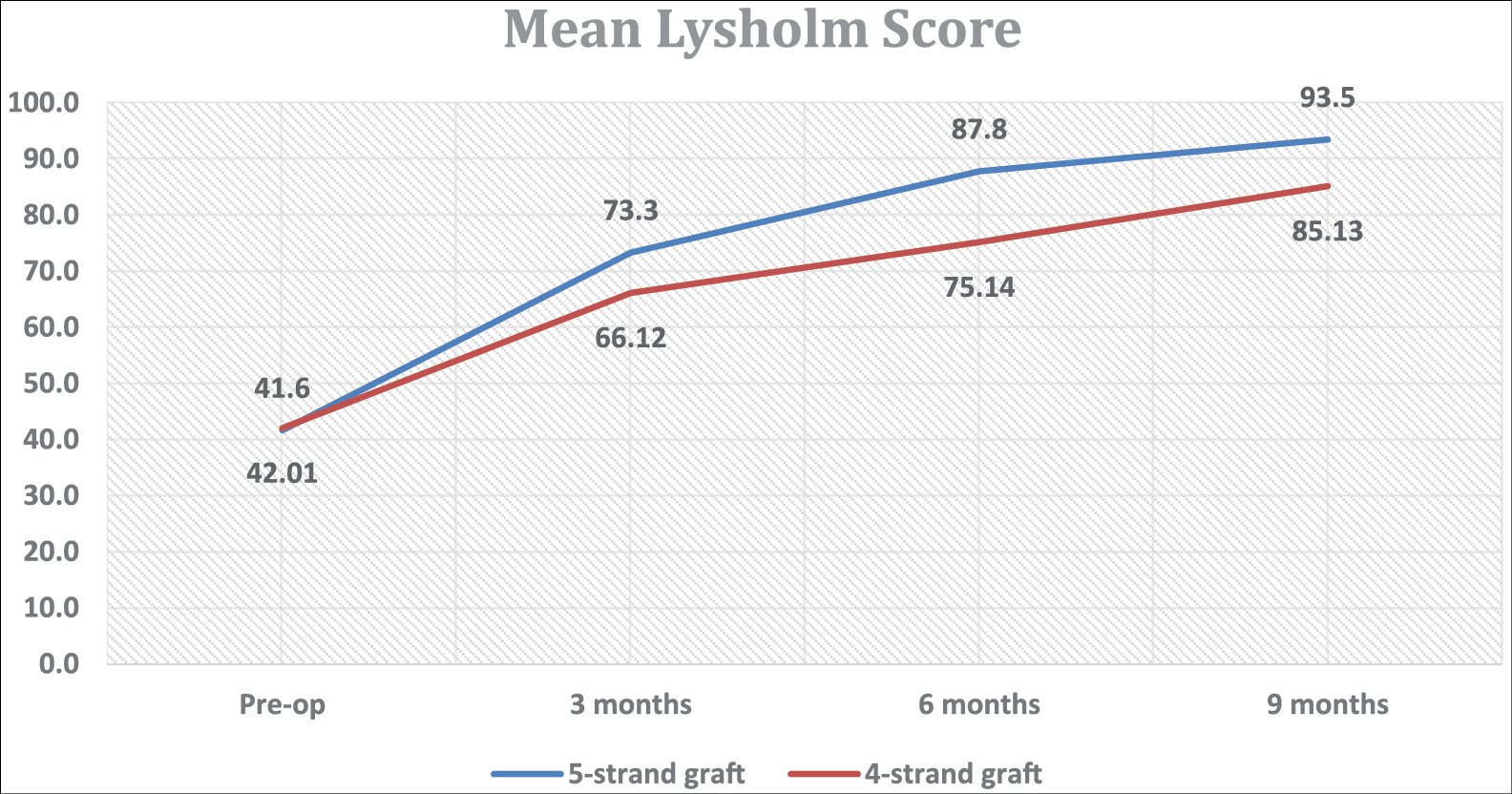
- Mean Lysholm score during follow-up period
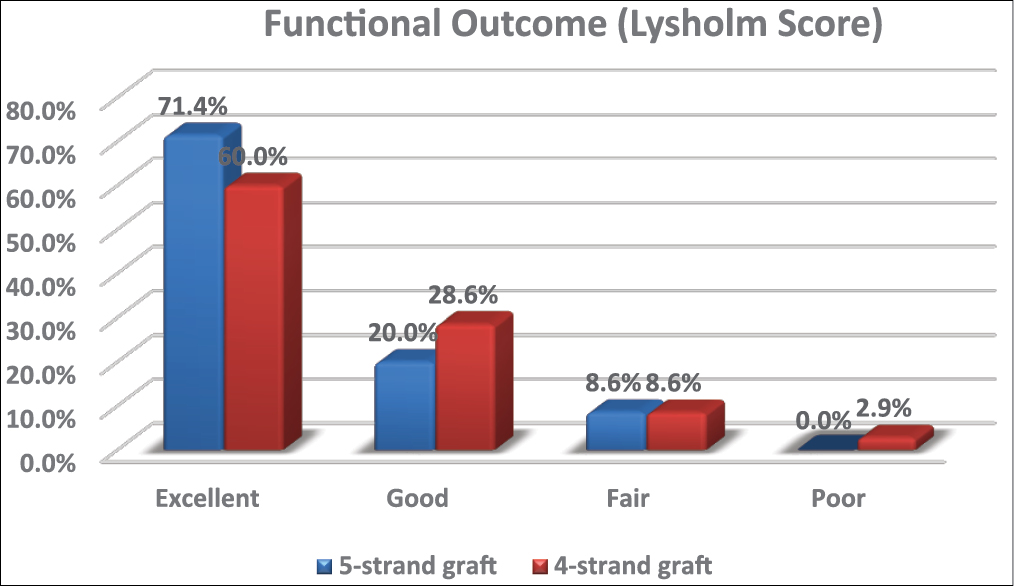
- Functional outcome as per Lysholm score at 9 months
Discussion
Anterior cruciate ligament injuries are significant when they involve a complete intra-substance tearing of the ACL in the knee. The injury is characterized by joint instability that leads to pain, decreased activity and function, poor-knee-related quality of life, and an increased risk of osteoarthritis of the knee. The ultimate goal of for the reconstruction of ACL is the restoration of normal knee kinematics. Various options for the graft are available for the treatment, and each option has its own set of advantages and limitations. The present study was conducted to evaluate and compare the functional outcome after 4-strand versus 5-strand hamstring autograft for anterior crucial ligament reconstruction.
The 3ST/2Gr 5-strand graft offers high strength and more length than the 4ST. Hence it is useful in patients with ligamentous laxity, small tendons, or other stability risk factors. In present study too, mean graft size was significantly more with 5-strand group (9.12 ± 0.60 mm versus 8.17 ± 0.41 mm; P < 0.01).
The functional outcome was measured by Lysholm knee scoring scale.[11] Lysholm knee scoring scale gives information as to how the knee problems have affected the patient’s ability to manage things in everyday life. After ACL reconstruction, function score was significantly more in 5-strand group (P < 0.05) [Figure 2]. Overall, excellent results were seen in 71.4% patients of 5-strand group as compared to 60% in 4-strand graft group, respectively. Poor outcome in terms of revision surgery was required in one case (2.9%) of 4-strand group and none in 5-strand group.
In a similar study by Wagh et al.,[12] 40 patients having ACL injury were treated using a 5-strand hamstring graft. A total of 30 patients had excellent outcome (75%), 7 (17.5%) persons had good outcome, and three persons (7.5%) had fair outcome but none had poor outcome as per Tegner Lysholm score. Figueroa et al.[13] observed an average post-operative Lysholm score as 93.3 in group A (quadruple ST-G graft) and 97.1 in group B (5-strand graft). Mean postoperative IKDC: 91 points in group A and 96.8 in group B (P = 0.18). The score was higher in 5-strand hamstring graft technique, suggesting that it is a valid option when there is an insufficient diameter graft. Lavery et al.[10] in their observation study concluded that use of 5-strand hamstring autograft for anterior cruciate ligament reconstruction significantly reduces revision rates. Prodromos et al.[9] treated 20 consecutive patients with 5HS ACL reconstruction using 3ST/2Gr. Study concluded that 5HS ACLR had higher stability than a high stability 4HS cohort. Authors recommended that 5HS is preferable to 4HS for ACL reconstruction, especially for double bundle techniques. Lee et al.[14] in their series also used 5-string hamstring graft with success and observed less revision rates.
Sideris et al.[15] in their study, however, observed no benefit of using a 5-strand hamstring tendon autograft when compared to the gold standard four-strand repair, specifically with regards to anterior stability of the knee in the first 12 weeks post-operatively. Krishna et al.[16] in another similar study observed no statistically significant difference between groups on postoperative Lysholm scores.
In present study, superficial infections were seen in three (8.6%) cases each while complaint of knee pain was given by one (2.9%) case of 4-strand group and none in 5-strand group. None of the cases developed deep infections. Cases with superficial infections were managed by course of antibiotics while NSAIDs were given as and when required for cases with knee pain.
Similar observations were also made by Wagh et al.,[12] Lee et al.[14] and Prodromos et al.[9] who observed no major complications in ACL reconstruction cases managed by 5-string hamstring graft.
Conclusion
Present study concluded that 3ST/2Gr 5-strand graft offers better functional outcome after anterior crucial ligament reconstruction than 4-strand graft. Using a 5-strand hamstring graft by creating three equal strands of semitendinosus and double of gracilis gives an increase in diameter of approx. 1 mm than 4-strand graft, reaching a maximum of 10 mm diameter in some cases. This provides more strength to the graft resulting in reduction in revision rates. The 5-strand graft is especially useful in patients with undersized hamstring graft, ligamentous laxity, small tendons, or other stability risk factors.
Criteria for inclusion
Dr. Chetan Goyal—Project Design, Manuscript writing
Dr. Surinder Singh Ajrawat—Operating surgeon
Dr. Joseph J. B. Mal—Data collection & Compilation
Dr. Bhuwan Sharma—Project Design, Data Analysis & Results Preparation
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Anterior cruciate ligament injuries. In: Garrick JG, ed. Orthopaedic knowledge update sports medicine III. Rosemont: American Academy of Orthopaedic Surgeons; 2004. p. :169.
- [Google Scholar]
- Minimum 10-year results after anterior cruciate ligament reconstruction: How the loss of normal knee motion compounds other factors related to the development of osteoarthritis after surgery. Am J Sports Med. 2009;37:471-80.
- [CrossRef] [PubMed] [Google Scholar]
- Descriptive epidemiology of the Multicenter ACL Revision Study (MARS) cohort. Am J Sports Med. 2010;38:1979-86.
- [CrossRef] [PubMed] [Google Scholar]
- Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am. 1999;81:549-57.
- [CrossRef] [PubMed] [Google Scholar]
- A biomechanical analysis of matched bone-patellar tendon-bone and double-looped semitendinosus and gracilis tendon grafts. Am J Sports Med. 1999;27:202-7.
- [CrossRef] [PubMed] [Google Scholar]
- Quality of life and clinical outcome comparison of semitendinosus and gracilis tendon versus patellar tendon autografts for anterior cruciate ligament reconstruction: An 11-year follow-up of a randomized controlled trial. Am J Sports Med. 2011;39:2161-9.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior cruciate ligament reconstruction with multistranded autogenous semitendinosus tendon. Am J Sports Med. 1996;24:504-9.
- [CrossRef] [PubMed] [Google Scholar]
- Preoperative magnetic resonance imaging cross-sectional area for the measurement of hamstring autograft diameter for reconstruction of the adolescent anterior cruciate ligament. Arthroscopy. 2008;24:1336-41.
- [CrossRef] [PubMed] [Google Scholar]
- 5-strand hamstring ACL reconstruction: A new technique with better long-term stability versus 4-strand (SS-13) Arthroscopy. 2006;22:e7.
- [CrossRef] [Google Scholar]
- Five-strand hamstring autograft for anterior cruciate ligament reconstruction. Arthrosc Tech. 2014;3:e423-6.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med. 1982;10:150-4.
- [CrossRef] [PubMed] [Google Scholar]
- Functional outcome of Arthroscopic reconstruction of single bundle anterior cruciate ligament using 5 strand hamstring graft. IOSR J Dent Med Sci. 2015;14:59-62.
- [Google Scholar]
- Five-strand hamstrings autograft versus quadruple hamstrings autograft, with graft diameters 8.0 millimeters or more, in anterior cruciate ligament reconstruction: Clinical outcomes with a minimum two year follow-up. Arthroscopy. 2017;33:142.
- [CrossRef] [Google Scholar]
- The 5-strand hamstring graft in anterior cruciate ligament reconstruction. Arthrosc Tech. 2014;3:e627627-e631.
- [CrossRef] [PubMed] [Google Scholar]
- Five strand hamstring tendon autograft for anterior cruciate ligament reconstruction provides no benefit over the gold standard four strand repair for anterior stability of the knee: A prospective cohort study. Open J Orthopedics. 2017;7:156-72.
- [CrossRef] [Google Scholar]
- A 5-strand hamstring autograft achieves outcomes comparable to those of a 4-strand hamstring autograft with a graft diameter of 8 mm or more in anterior cruciate ligament reconstruction. Orthop J Sports Med. 2018;6:1-7.
- [CrossRef] [PubMed] [Google Scholar]




