
Translate this page into:
Acute tarsal tunnel syndrome in a pregnant woman following surgical repair of bimalleolar fracture: A case report and review of the literature
Address for correspondence: Dr. Jerry Grimes, 3601 4th Street, 4th Floor, Lubbock, TX 79430, USA. E-mail: jerry.grimes@ttuhsc.edu
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Ratra A, Grimes J. Acute tarsal tunnel syndrome in a pregnant woman following surgical repair of bimalleolar fracture: A case report and review of the literature. J Orthop Allied Sci 2016;4:49-51.
Abstract
Tarsal tunnel syndrome is generally a subacute condition that gradually develops and worsens with time. Urgent tarsal tunnel release to treat an acute onset of symptomatic neurocompression within the tarsal tunnel following a fracture repair has not been previously reported. We present a case of a pregnant woman who developed an acute tarsal tunnel syndrome following an open reduction internal fixation of an ankle fracture. The urgent release of the tarsal tunnel resulted in resolution of her symptoms.
Keywords
Acute tarsal tunnel syndrome
bimalleolar fracture
urgent tarsal tunnel release

Introduction
Tarsal tunnel syndrome is a compressive neuropathy in the lower extremity.[1] It is well- described in the literature and is typically a subacute condition. Trauma, varicosities, edema from pregnancy, diabetes, inflammatory arthropathies, and space occupying lesions are described etiologies.[2,3,4] The underlying common factor in all such cases is a compression of the posterior tibial nerve and/or its terminal branches in the posterior tibial neurovascular tunnel. We report a case of an acute tarsal tunnel syndrome in a pregnant woman developing after open reduction internal fixation of a bimalleolar fracture successfully treated with an urgent tarsal tunnel release. To our knowledge, this is the first reported case of an urgent tarsal tunnel release performed after open reduction-internal fixation of an ankle fracture.
Case Report
A 22-year-old gravida 3, para 2 female 8 weeks pregnant was involved in a motor vehicle accident where she was the restrained driver. The patient was hemodynamically stable. Musculoskeletal injuries included diastasis of the pubic symphysis without sacroiliac joint widening, a laceration to the anterior leg, and a right closed bimalleolar fracture. The patient underwent a closed right ankle reduction in the emergency department. The patient had intact sensation in the foot both before and after the reduction. Later the same day the patient was treated by an open reduction and internal fixation of the right bimalleolar ankle fracture. The patient was splinted in neutral position postoperatively. Figures 1 and 2 show the postoperative radiographs.
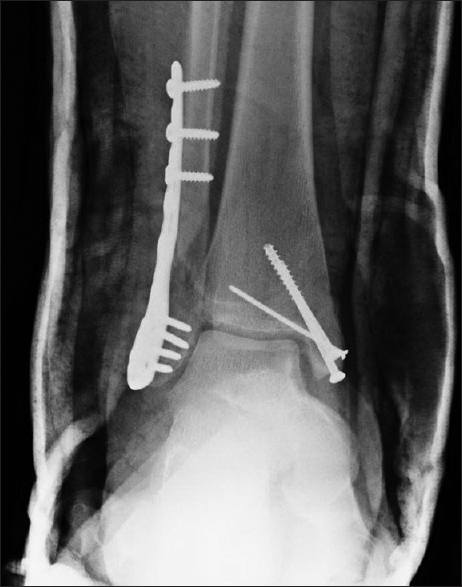
- Plain radiograph of the ankle-anteroposterior view

- Plain radiograph of the ankle lateral view
Twenty-four hours after the surgical fixation of the ankle, the patient reported onset of severe pain in the plantar aspect of the right foot. The pain was not responsive to typical opiate dosages. The splint was initially loosened and eventually removed without improvement of symptoms. The swelling and ecchymosis noted were typical of a postoperative bimalleolar ankle fracture. There was no swelling at the arch of the foot. Any dorsiflexion of the hallux caused the pain to become markedly severe. Palpation over the tarsal tunnel resulted in severe pain in the plantar aspect of the foot. Tapping over the tarsal tunnel produced radiation of the pain both proximal and distal along the anatomical course of the posterior tibial nerve, a positive Valleix phenomenon.[1] The dorsiflexion-eversion test was positive.[5] Based on these findings, a diagnosis of an acute tarsal tunnel syndrome was made.
We treated the patient with an urgent tarsal tunnel release. A curvilinear incision, 4 cm posterior to the incision used to address the medial malleolus, was used to expose the tarsal tunnel and maximize the skin bridge. The flexor retinaculum was incised releasing a large hematoma. The nerve and its branches were found to be intact. The posterior tibial artery was found to be intact and pulsatile with no active bleeding. A freer was used to palpate the tissue proximal to the incision, and there appeared to be no restrictions.
In order to ensure that there was no compartment syndrome in the foot, a Synthes compartment measurement probe was inserted through an 18-gauge angiocath into the medial compartment. The pressures measured were normal, and no compartment release was necessary. The patient was placed back into a splint. Two hours after the procedure, the patient reported that her pain had significantly improved. A sensory exam of the plantar foot showed intact sensation and dorsiflexion of the hallux did not cause excessive discomfort.
The patient was followed regularly for a year postoperatively. The parallel medial incisions healed routinely. The patient reported no complications and the examination of the tarsal tunnel did not produce any continued symptoms. The plantar foot sensation remained intact.
Discussion
The posterior tibial neurovascular tunnel, the tarsal tunnel, is a fibro-osseous tunnel in the medial ankle, behind and inferior to the medial malleolus in the lower leg.[3,6] The floor of the tunnel is formed by the medial wall of the distal tibia, talus, and calcaneus.[1] The flexor retinaculum forms the roof of the tunnel. Contents of the tunnel from lateral to medial include: Flexor hallucis longus tendon, posterior tibial nerve, posterior tibial artery, posterior tibial vein, flexor digitorum longus tendon, and tibialis posterior tendon. Inside the tunnel, the posterior tibial nerve branches into calcaneal, medial plantar and lateral plantar nerves. Compression of these nerves within the tunnel results in symptomatic neuropathy known as the tarsal tunnel syndrome.[1,3,6,7,8]
Entrapment neuropathy of the posterior tibial nerve and/or its branches in the tarsal tunnel was first described by Kopell and Thompson in 1960.[1,9] This was subsequently named as tarsal tunnel syndrome by Keck in his case report published in 1962.[7] Tarsal tunnel syndrome is typically a chronic condition with a gradual onset that becomes symptomatic over an extended period of time. It is often treated with surgery performed on a nonemergent basis. Surgical decompression to treat tarsal tunnel syndrome was first described by Lam in 1967 with good outcomes in all 10 cases.[8] Numerous studies have reported different success rates, ranging from as low as 44% to as high as 91%.[2,3,10,11,12]
Ankle fractures involving the floor of the tarsal tunnel and medial distal tibia are common. The development of a hematoma adjacent to the fracture is not unexpected. However, the paucity of reports of associated tarsal tunnel indicates that this injury does not typically result in a space occupying lesion of the tarsal canal. Whether the patient's pregnancy increased, the risk of the condition is certainly worth considering. There was no edema noted in the contralateral limb or during the postoperative course.
The acute distress of the patient, in this case, prompted consideration for urgent treatment. Review of the literature failed to indicate a preferred treatment course. While much less common, tarsal tunnel shares some of the characteristics of carpal tunnel.[1] The general recommendation for acute carpal tunnel syndrome associated with a distal radius fracture that fails to resolve with a reduction is to perform an open release.[13,14] Based on the common characteristics, we followed a similar treatment approach in this case.
There is little literature indicating the appropriate timing of a tarsal tunnel release for an acute onset of symptoms.[1,6,15,16] In one reported a case of acute traumatic tarsal tunnel syndrome, an avulsion of the flexor hallucis longus resulted in a space occupying mass.[17] The patient had a profound sensory loss on the plantar foot. The surgical release was performed 2 days after the injury with good results and full recovery of the neurologic function. This indicates that the posterior tibial nerve is resilient to injury following short periods of acute compression. The effect of longer periods of compression is not available.
Ahmad et al., in their review article, emphasize that early decompression of the tarsal tunnel is important to prevent the development of intraneural fibrosis and myopathy which would result in less favorable surgical outcomes.[3] Similarly, Takakura et al. found that surgical success and recovery of nerve function was time dependent. Surgeries performed more than 10 months from the onset of symptoms were associated with poorer recovery of nerve function.[18] While these studies do not deal with the traumatic acute tarsal syndrome, they support the concept that early surgical treatment improves outcomes.
This case illustrates that tarsal tunnel syndrome can occur after surgical fixation of an ankle fracture. Treatment with an urgent surgical release resulted in resolution of symptoms and complete recovery of neurologic function. Based on surgical findings, in this case, it is likely the original surgical incision could have been utilized to drain the hematoma. Without knowledge of the etiology of the nerve compression, we chose to explore the tarsal tunnel. We propose that carefully placed incision that allows access to contents of the tarsal tunnel can be performed in an uncompromised host with good results.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Tarsal tunnel syndrome: Review of the literature. Foot Ankle. 1990;11:47-52.
- [CrossRef] [PubMed] [Google Scholar]
- Traumatic tarsal tunnel syndrome: The outcome of surgical decompression. Foot Ankle Surg. 2002;8:41-4.
- [CrossRef] [Google Scholar]
- Tarsal tunnel syndrome: A literature review. Foot Ankle Surg. 2012;18:149-52.
- [CrossRef] [PubMed] [Google Scholar]
- Tarsal tunnel syndrome after non-dislocated fracture of the outer ankle joint (case report with review of the literature) Wien Klin Wochenschr. 1993;105:89-91.
- [Google Scholar]
- Tarsal-tunnel syndrome. Review of the literature and two case reports. Clin Orthop Relat Res. 1972;88:76-9.
- [CrossRef] [PubMed] [Google Scholar]
- Peripheral entrapment neuropathies of the lower extremity. N Engl J Med. 1960;262:56-60.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical results after tarsal tunnel decompression. J Bone Joint Surg Am. 1994;76:1222-30.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior tarsal tunnel syndrome: Diagnosis and treatment. Dtsch Arztebl Int. 2008;105:776-81.
- [CrossRef] [PubMed] [Google Scholar]
- Entrapment neuropathy: The etiology of intractable chronic heel pain syndrome. J Foot Ankle Surg. 1998;37:273-9.
- [CrossRef] [PubMed] [Google Scholar]
- Carpal tunnel syndrome after distal radius fracture. Orthop Clin North Am. 2012;43:521-7.
- [CrossRef] [PubMed] [Google Scholar]
- Avoiding and treating perioperative complications of distal radius fractures. Hand Clin. 2012;28:185-98.
- [CrossRef] [PubMed] [Google Scholar]
- Acute tarsal tunnel syndrome following partial avulsion of the flexor hallucis longus muscle: A case report. J Foot Ankle Surg. 2002;41:243-6.
- [CrossRef] [PubMed] [Google Scholar]
- Tarsal tunnel syndrome. Causes and results of operative treatment. J Bone Joint Surg Br. 1991;73:125-8.
- [CrossRef] [PubMed] [Google Scholar]




