
Translate this page into:
A randomized controlled comparative study of functional outcome of chronic refractory plantar fasciitis treated with platelet-rich plasma injection and corticosteroid injection
Address for correspondence: Prof. Dr. M. Vijayashankar, Department of Orthopaedics, Chettinad Hospital and Research Institute, Kelambakkam, Chennai 600126, Tamil Nadu, India. E-mail: vijayashankar.m@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Balashanmugam AN, Kothimbakkam PK, Bharath V, Guhan RK, Ganesh A, Vijayashankar M. A randomized controlled comparative study of functional outcome of chronic refractory plantar fasciitis treated with platelet-rich plasma injection and corticosteroid injection. J Orthop Spine 2023;11:19-23.
Abstract
BACKGROUND:
Chronic refractory plantar fasciitis is one of the common causes for long-standing pain in the heel region, which has to be intervened with minimally invasive intralesional injections. The aim of this randomized controlled study was done to compare the functional outcome of patients who have not responded to 6 weeks of conservative treatment for chronic plantar fasciitis (6 months), treated with platelet-rich plasma (PRP) injection and corticosteroid injection.
PATIENTS AND METHODS:
All patients diagnosed with chronic plantar fasciitis, who did not respond to 6 weeks of conservative trial who came to the orthopedic department of this institute from September 2019 to March 2021, were added in this research. Thirty patients in each group were randomly assigned as per inclusion and exclusion criteria.
RESULTS:
The mean age receiving PRP (group 1) was 42 and corticosteroid (group 2) was 39.87, respectively. This study comprising of 60 patients had 13 males and 47 females, respectively. Among them, 7 males and 23 females received PRP injection and 6 males and 24 females received corticosteroid injection. At the conclusion of 6 months, the PRP group had a sustained surge in foot and ankle outcome score (FAOS) score (87.23), on the other hand, the corticosteroid group (77.5) had a fall in the FAOS score after three months. At the completion of 6 months, the PRP group had a decrease in visual anolog score (VAS) score (1.93), and the corticosteroid group (3.33) had a raise in the VAS score after 3 months.
CONCLUSION:
Our research has concluded that PRP injection is efficacious in a long run. At the same time, corticosteroid injection efficacy started to decline after three months.
Keywords
A randomized controlled study
chronic plantar fasciitis
corticosteroid
FAOS score
platelet-rich plasma
VAS score

Introduction
Plantar fasciitis is considered to be one of the common causes for long standing pain in the heel region. Plantar fasciitis is commonly seen both in the younger age group who are physically active believed to result from repetitive overloading in the heel and in older age group with a more sedentary lifestyle. Current literature proposes that plantar fasciitis is better termed fasciosis for longevity of the condition with findings of degeneration rather than inflammation.[1,2]
It might take months or years to resolve, posing a difficulty to treating professionals. In roughly 85% of instances, the underlying etiology of the condition is unclear.[3]
This study has been performed to witness how does the functional outcome of chronic refractory plantar fasciitis patients managed with platelet-rich plasma (PRP) injection and corticosteroid injection differ over the period of 6 months in terms of the onset, duration, and weaning off of its effect.
Patients and Methods
This study was performed in the Department of Orthopaedics in a Tertiary Care Hospital. This is a randomized controlled study (single blinded study—investigator blinded). All patients with chronic plantar fasciitis, both clinically and radiologically (local ultrasonographic examination), who had tried at least 6 weeks of conservative treatment (without any injections locally) for chronic plantar fasciitis (6 months) and were not relieved of heel pain, who came to the orthopaedic department of this institute from September 2019 to March 2021 were added in this study after clearly explaining about the process and obtaining the informed consent. Simple randomization using the lottery method was used to randomize the sample. All the patients were randomized into Group 1 (30 subjects managed with PRP injection) and Group 2 (30 subjects managed with corticosteroid injection). Patients were selected based of clinical and radiological evaluation. Clinically, patients with history of early morning heel pain aggravated in the first few steps after prolonged recumbency in the night and with an examination finding of tenderness in the anterior border of medial calcaneal tuberosity and radiologically, calcaneal spur in the X ray of the affected heel and facial thickness (>4.5 mm)[4] in ultrasonogram of affected heel were included in the study.
Following the results and thorough conversation with the patient about the therapeutic intervention, the treatment process was carried out. During the conversation, all of the patients’ questions were answered, and if the patient is still ready to pursue the planned course of treatment and participate in our study, the treatment procedure was carried out. After the injection, the patient was kept under observation with vital signs monitoring for 15 min immediately following injection. They are discharged on the same day and asked to avoid strenuous activities for the next 2 weeks. They were followed up by VAS & FAOS scores. Assessment was done just prior to the injection and at 4, 8, 12 weeks and at 6 months.
Results
Mean age of subjects receiving PRP (group 1) was 42 and corticosteroid (group 2) was 39.87, respectively. This study comprising of 60 patients—13 males and 47 females. Among them 7 males and 23 females got PRP injection and 6 males and 24 females received corticosteroid injection [Figure 1].
- Bar diagram showing percentage of sex distribution in PRP and corticosteroid groups
Bar diagram shows percentage of sex distribution in the PRP and corticosteroid groups [Figure 1].
In this study of 60 patients, 60% (36) had right heel affection and 40% (24) had left heel affection.
Foot and ankle outcome score
Shows mean FAOS score of PRP and corticosteroid group [Figure 2].
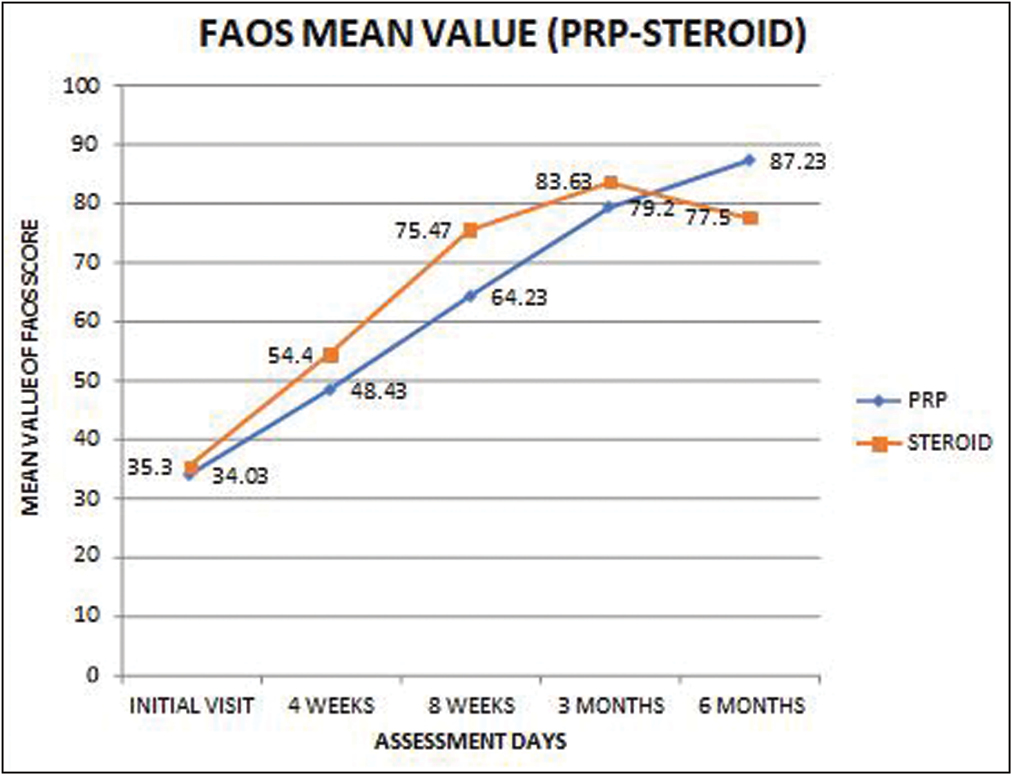
- Mean FAOS score of PRP and corticosteroid group
On assessing the patients who have undergone PRP and corticosteroid injection, at first follow-up, had a mean FAOS score of 34.03 and 35.3. On further follow-up, at 4 weeks, FAOS score exhibited a rise in the corticosteroid group (54.4) when compared to the PRP group (48. 43). At 8 weeks of follow-up, the FAOS score improved in corticosteroid group (75.47) when compared to PRP group (64.23). At the conclusion of 3 months, the FAOS score improved in corticosteroid group (83.63) when compared to the PRP group (79.2). At the conclusion of 6 months, the PRP group had a sustained surge in FAOS score (87.23), on the other hand, the corticosteroid group (77.5) had a fall in the FAOS score after three months. Hence, corticosteroid injection is more efficacious for a short run, and PRP is taking some time to act but is having a sustained and a steady response and effective in a long run [Table 1 and Figure 2].
| Type of injection | N | Mean | Std. deviation | Std. error mean | P value (T-test) | |
|---|---|---|---|---|---|---|
| FAOS-initial visit | PRP | 30 | 34.03 | 2.46 | 0.4485 | 0.04031 (not Significant) |
| Corticosteroid | 30 | 35.3 | 2.22 | 0.4044 | ||
| FAOS—4 weeks | PRP | 30 | 48.43 | 2.98 | 0.5439 | 0.00001 (significant) |
| Corticosteroid | 30 | 54.4 | 2.54 | 0.4639 | ||
| FAOS—8 weeks | PRP | 30 | 64.23 | 2.21 | 0.4031 | 0.00001 (significant) |
| Corticosteroid | 30 | 75.47 | 2.89 | 0.5268 | ||
| FAOS—3 months | PRP | 30 | 79.2 | 2.34 | 0.4272 | 0.00042 (significant) |
| Corticosteroid | 30 | 83.63 | 6.05 | 1.1054 | ||
| FAOS—6 months | PRP | 30 | 87.23 | 2.70 | 0.4929 | 0.00001 (significant) |
| Corticosteroid | 30 | 775 | 5.40 | 0.9858 |
Visual anolog score
Shows mean VAS score of PRP and corticosteroid group [Figure 3].
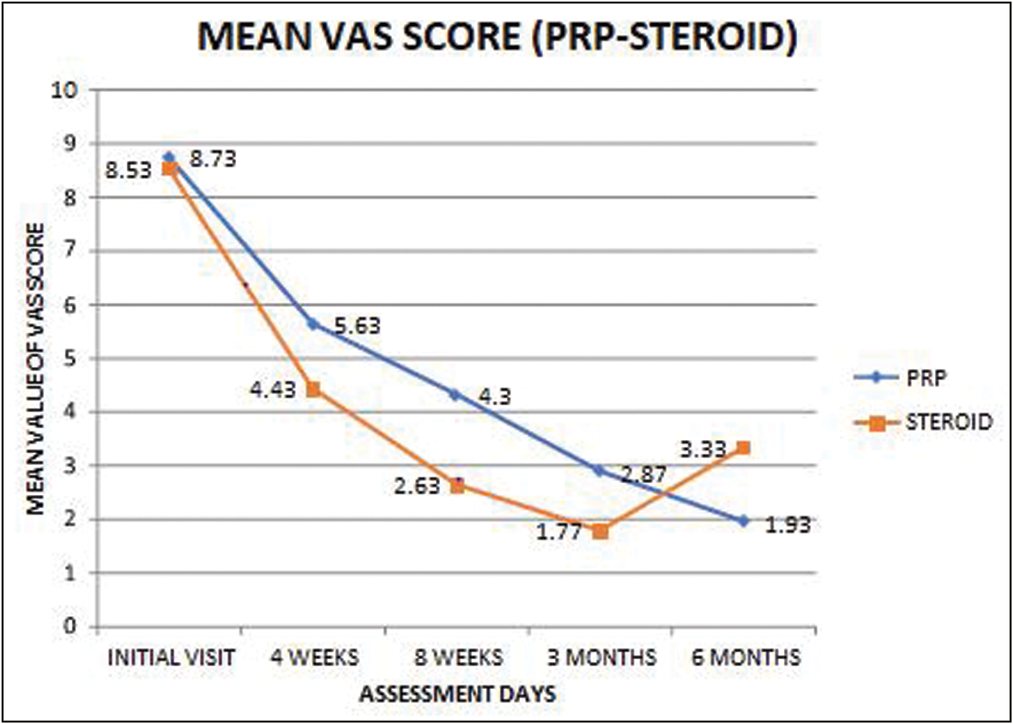
- Mean VAS score of PRP and corticosteroid group
On assessing the patients who have undergone PRP, corticosteroid injection, at the first follow-up, had a mean VAS score of 8.73 and 8.53. On further follow-up, at 4 weeks, VAS score showed a significant fall in the corticosteroid group (4.43) when compared to the PRP group (5.63). At 8 weeks of follow-up, the VAS score further decreased in the corticosteroid group (2.6) when compared to the PRP group (4.3). At the end of 3 months, the VAS score declined in the corticosteroid group (1.77) compared to the PRP group (2. 87). At the completion of 6 months, the PRP group had a decrease in VAS score (1.93), and the corticosteroid group (3.33) had a raise in the VAS score after 3 months. Hence, corticosteroid injection is more efficacious for a short run and PRP is taking a substantial time period to show its effectiveness in the long run [Table 2 and Figure 3].
| VAS scoring | Type of injection | N | Mean | Standard deviation | Std. error mean | P value (T-test) |
|---|---|---|---|---|---|---|
| VAS initial visit | PRP | 30 | 8.73 | 0.69 | 0.1263 | 0.2269 (not significant) |
| Steroid | 30 | 8.53 | 0.57 | 0.1263 | ||
| VAS 4 weeks | PRP | 30 | 5.63 | 0.81 | 0.1477 | 0.00001 (significant) |
| Steroid | 30 | 4.43 | 0.50 | 0.0920 | ||
| VAS 8 weeks | PRP | 30 | 4.30 | 0.53 | 0.0977 | 0.00001 (significant) |
| Steroid | 30 | 2.63 | 0.49 | 0.0894 | ||
| VAS 3 months | PRP | 30 | 2.87 | 0.57 | 0.1043 | 0.00001 (significant) |
| Steroid | 30 | 1.77 | 0.68 | 0.1240 | ||
| VAS 6 months | PRP | 30 | 1.93 | 0.94 | 0.1724 | 0.00001 (significant) |
| Steroid | 30 | 3.33 | 1.06 | 0.1938 |
Three patients (10%) in the PRP group (in 30 patients) and 5 patients (16.6%) in the corticosteroid group (in 30 patients) had persistent heel pain with certain functional loss at 6 months of follow-up. Total of 8 (13.33%) had persistent heel pain out of 60 patients in the trial.
However, all the patients in the trial did not have any other complications.
Discussion
Plantar fasciitis is a highly prevalent disease that, in most cases, resolves on its own. A targeted history, physical examination is performed as part of the evaluation. Conservative management is efficacious in more than 90% of the subjects. Weight-bearing X-rays are utilized for radiological diagnosis though not specific. magnetic resonance imaging or ultrasonography is employed for atypical presentations or cases that are refractory to first-line of treatment. If symptoms persist, less invasive techniques or operative procedures are used. The less invasive treatments, which includes corticosteroid injection, botulinum toxin injection, platelet-rich plasma injection, and extracorporeal shockwave therapy, aim to alleviate pain or boost the body’s healing response (steroid injection). Partial plantar fasciotomy and lengthening of the gastrocnemius muscle are operative procedures that can be considered for recalcitrant chronic plantar fasciitis. There is no unanimous preference for one operative procedure over another.[1]
Martinelli et al.[5] administered 3 (once a week) injections for chronic plantar fasciitis and found that mean VAS fell from 7.1 to 2. 1 at the end of 12 months with great outcomes in the final follow-up in 9 patients, moderate results in 4, and bad results in 1. But our study showed reduction in VAS from 8.73 to 1. 93 with just one PRP injection and has shown a faster response in 6 months.
Monto[6] carried out a prospective randomized comparative study. Forty patients (23 females17 males) with chronic plantar fasciitis (unilateral cases) who had not responded to at least 4 months of standardized conservative treatment regimens were randomized, managed with any one of solitary ultrasonogram-guided injection of 3 mL of PRP or 40 mg of Depo Medrol cortisone. The cortisone group assessed before injection had a mean American orthopaedic foot and ankle society score of 52 compared to 35.3 in our study, which rose to 81 at the end of 3 months compare to 83. 63 in our study, but declined to 74 at 6 months compared to 77.5 in our study, then regressed back to the range of 58 at 12 months, and finally to 56 at 24 months. The PRP group, on the other hand, started with a mean American orthopaedic foot and ankle society score of 37 when assessed before injection compared to 34.03 in our study, grew to 95 at 3 months compared to 79.2 in our study, sustained at 94 at 6 months compared to 87.23 in our study, sustained at 12 months of follow-up and finished with a concluding score of 92 at the end of 2 years of follow-up. Further studies need to be done with a longer period of follow-up in order to test the durability of PRP injection.
According to Carofino et al.[7] adding anesthetics or corticosteroids to PRP led to reductions in tendon cell replication and survival. These findings imply that combining anesthetics or corticosteroids with PRP injection, either alone or in combination, may undermine the possibly positive in vitro response of isolated PRP on tendon cells or affect cell survival at the point of tendon damage. But in our study, we are injecting PRP and corticosteroid mixed with 2% lidocaine and evaluated if there is any significant differences between our study and other similar studies. There is no significant difference in results. After extensive research, there are no similar in vivo studies where local anesthetics are mixed with PRP injections and corticosteroid injections, to assess its impact in PRP and corticosteroid outcome in vivo. On the other hand, it is easier to administer PRP and corticosteroid injections mixed with local anesthetic in a single shot procedure. Further comparative studies need to be performed to compare the efficacy of the above two drug modalities (PRP and corticosteroid) administered with or without local anesthetics.
Conclusion
Patients who underwent corticosteroid injections showed good amount of symptomatic relief quickly for the initial 3 months from the day of injection when compared to the patients who received PRP injection. Whereas patients who received PRP injections started showing good amount of symptomatic relief only after 3 months after the injection and the effect sustained for the next 3 months, which contributes to 6-month final follow-up of the study. However, the corticosteroid group started showing recurrence of symptoms after three months. Further study needs to be done with a larger sample size, long-term follow-up at least for a year, and to find out the true efficacy of the therapeutic PRP and corticosteroid injection.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Evaluation and treatment of chronic plantar fasciitis. Foot Ankle Orthop. 2020;5:247301141989676.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet rich plasma therapy: A comparative effective therapy with promising results in plantar fasciitis. J Clin Orthop Trauma. 2013;4:313. 1-35.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and management of plantar fasciitis in primary care. Br J Gen Pract. 2012;62:443-4.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich plasma (PRP) and platelet-rich fibrin (PRF): Surgical adjuvants, preparations for in situ regenerative medicine and tools for tissue engineering. Curr Pharm Biotechnol. 2012;13:1121-30.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet- rich plasma injections for chronic plantar fasciitis. Int Orthop. 2013;37:839-42.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich plasma efficacy versus corticosteroid injection treatment for chronic severe plantar fasciitis. Foot Ankle Int. 2014;35:313-8.
- [CrossRef] [PubMed] [Google Scholar]
- Corticosteroids and local anaesthetics decrease positive effects of platelet-rich plasma: An in vitro study on human tendon cells. Arthroscopy. 2012;28:711-9.
- [CrossRef] [PubMed] [Google Scholar]




