
Translate this page into:
A novel economical approach to gait analysis using locally available digital tools in a tertiary care hospital setting
Address for correspondence: Prof. Vetrivel Chezian Sengodan, Institute of Orthopaedics and Traumatology, Coimbatore Medical College Hospital (Affiliated to The Tamil Nadu Dr. M.G.R. Medical University), 16H, Housing Unit, Mettupalayam, Coimbatore 641301, Tamil Nadu, India. E-mail: svcortho@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Sengodan VC, Ramakrishnan K, Balakumaran A, Mohammed Batcha FA. A novel economical approach to gait analysis using locally available digital tools in a tertiary care hospital setting. J Orthop Spine 2023;11:14-8.
Abstract
BACKGROUND:
Analysis of gait parameters is an essential component of diagnosing musculoskeletal/neuromuscular conditions. A standard approach to gait analysis involves sophisticated commercially available digital technologies, which are expensive and not affordable by under-resourced tertiary care hospitals. We aimed here to test the validity of a low-cost digital tool for gait analysis in a tertiary care hospital setting.
MATERIALS AND METHODS:
This study used a smartphone with a 12-megapixel camera mounted on a tripod with Kinovea software (version 0.9.5, Free Software Foundation, Inc., Boston, MA, USA, distributed under a GPL v2 license) for gait analysis in our tertiary care hospital. This novel indigenous tool was validated in 502 healthy individuals by comparing standard gait parameters evaluated between younger and healthy cohorts.
RESULTS:
Overall, the recording and analysis process was simple, quick, and easy to use. The validity of our novel indigenous gait analysis tool was established by observation of reduced stride length, foot clearance, and knee goniometry among elderly subjects compared to the younger cohorts. Our observation of the elderly subjects showing altered gait parameters compared to the younger age group was consistent with previous studies measuring the same parameters using commercially available standard gait analysis tools.
CONCLUSION:
The novel indigenous approach validated in this study offers a low-cost and effective tool for routine gait analysis in any under-resourced tertiary or primary care hospital setting.
Keywords
Digital tools
foot clearance
gait analysis
locomotion
stride length

Introduction
Gait is facilitated by complex musculoskeletal and neuromuscular physiology.[1] Gait cycle is the movement from a one-foot strike to a successive foot strike on the same side [Figure 1].[2] Gait analysis measures various parameters during stance and swing phase.[3] Dedicated gait analysis facility establishment is expensive.[4] Gait pattern assessment in tertiary or primary care hospitals may help detect musculoskeletal/neuromuscular conditions early. In this study, we aimed to assess the feasibility of gait analysis in a tertiary care hospital using widely available digital tools and open-access software.
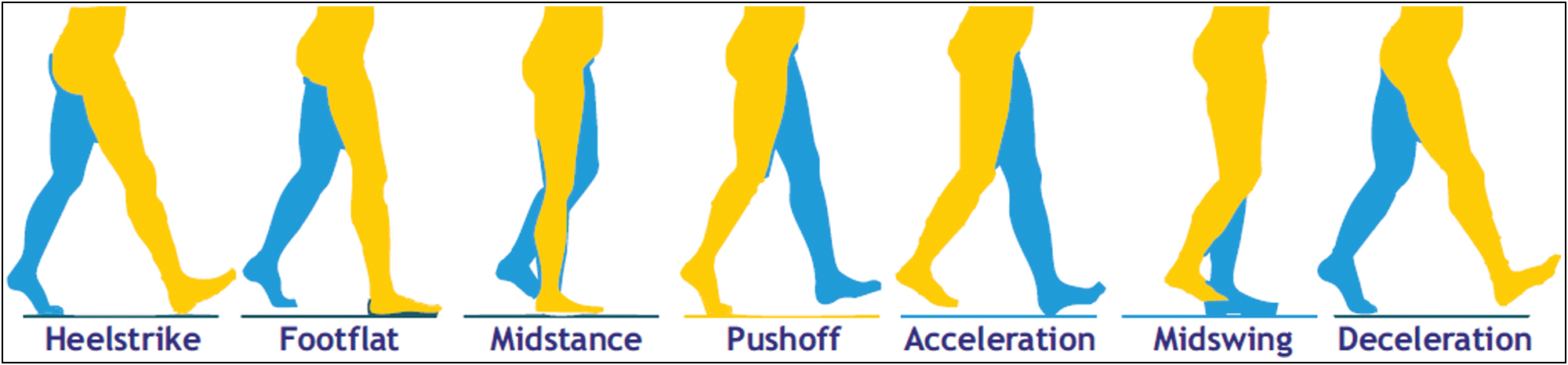
- Various steps in a normal gait cycle of humans (reproduction size at column width)
Material and Methods
The study was conducted from December 2020 to September 2021 after obtaining approval from the Institutional Ethics Review Committee. Gait analysis was performed on 502 healthy individuals attending the outpatient clinic. Among the 502 subjects in our study, 202 were males and 300 were females. The 502 subjects were categorized into younger (age 50 years and below) and elderly (age more than 50 years) age groups, which included 205 individuals in the younger group and 297 individuals in the elderly group.
Adults who could walk without physical support were included in this study. Patients with neurological pathology, stroke patients, and the pediatric age group were excluded from this study. Written informed consent was obtained from all the individuals enrolled in the study. Participants were instructed to walk without footwear during the video recording.
The gait pattern of the individuals was recorded in sagittal plane with two mobile phone cameras. The walkway was set at five meters long. The sagittal plane video was recorded by a mobile phone held on a tripod stand three meters away from the subject [Figure 2]. Three to five gait cycles were captured. Videos were recorded with a standard regular smartphone (12-megapixel rear camera, f/1.8 aperture). Videos were recorded in slow motion mode at 240 frames per second in 1080-p high definition.

- Video recording setup used in this study. The pathway length was 5 m with the recording camera placed at a distance of 3 m from the subject (reproduction size at column width)
All videos were examined, and the best clips (at the discretion of assessing orthopedic specialists) were chosen for analysis. Kinovea software (version 0.9.3), a free software distributed under a GPL v2 license, was used in this study. The following parameters were measured and compared between younger (≤50 years) and elderly (>50 years) age groups: (1) foot clearance, (2) stride length, (3) range of motion at the knee joint, and (4) range of motion at the ankle joint.
The data captured was summarized in an Excel sheet and is represented as the mean of the study cohort. The data between young and elderly subjects were statistically analyzed using t test for equality of means and Mann–Whitney test (since the sample is nonrandom) to assess statistical significance.
Results
The gait pattern of 502 individuals was recorded using our novel digital recording setup, and parameters, such as stride length, foot clearance, knee, and ankle range of motion, were analyzed. Overall, the recording and analysis process was simple, quick, and easy to use.
Stride length
Stride length is defined as the distance measured parallel to the line of progression, including two consecutive steps [Figure 3].[5] The average stride length among the younger and elderly age groups was observed to be 127.01 and 112.60 cm, respectively [Table 1]. The stride length in younger cohorts was significantly (P < 0.01) higher than in the elderly subjects. This finding, although not unexpected, is consistent with several other studies assessing gait patterns using commercially available expensive gait analysis tools.
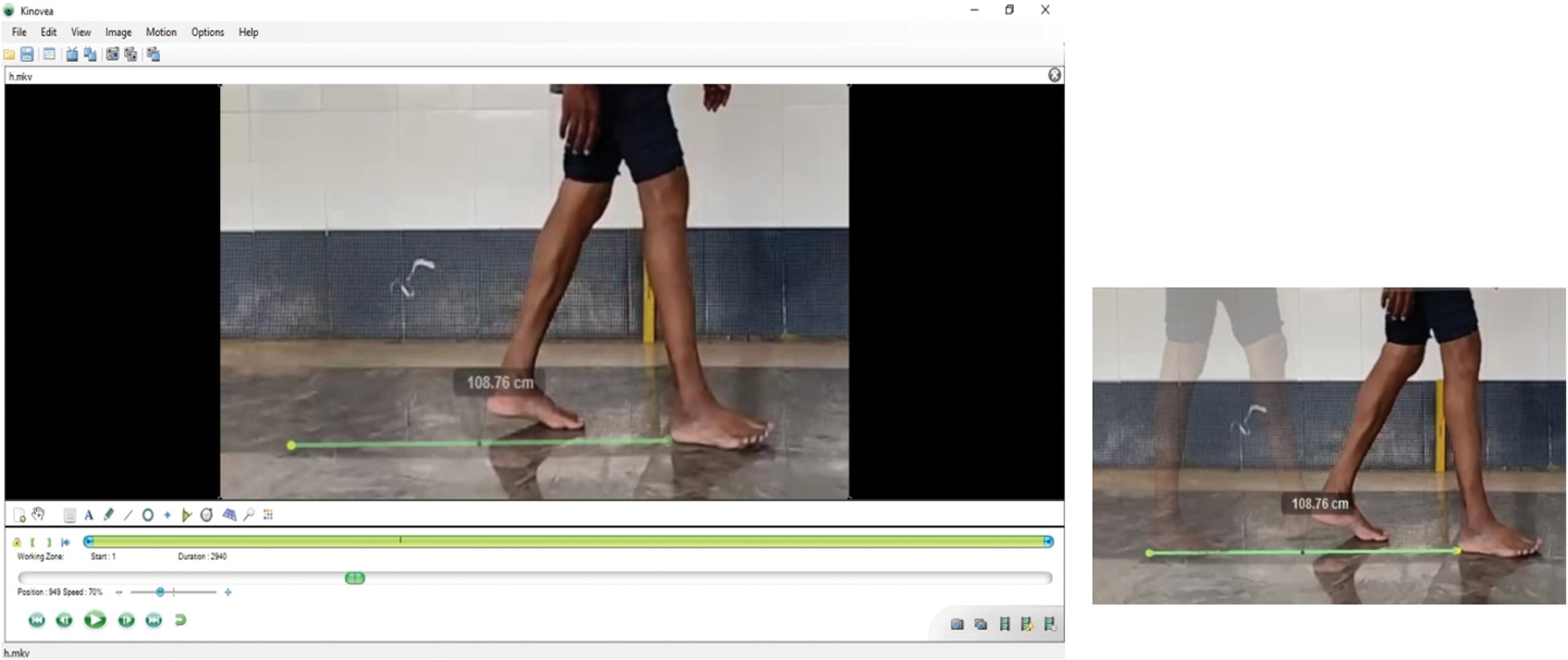
- A process of measuring the stride length using Kinovea software (reproduction size at column width)
| Number of individual | Mean stride length (cm) | Mean foot clearance (cm) | Mean knee range of motion (°) | Mean ankle range of motion (°) | |
|---|---|---|---|---|---|
| Young (<50 years) | 205 | 12701 ± 21.03 | 3.68 ± 1.41 | 48.91 ± 13.44 | 20.20 ± 8.36 |
| Elderly (>50 years) | 297 | 112.60 ± 21.76 | 2.98 ± 0.95 | 44.44 ± 13.99 | 19.59 ± 8.55 |
Foot clearance
Foot clearance was defined as the foot’s height during the swing phase, it is an important gait parameter used to assess the risk of falling [Figure 4].[4] The mean foot clearance in the younger and elderly cohorts was observed to be 3.68 cm and 2.98 cm, respectively [Table 1]. Similar to the stride length, the foot clearance distance was significantly (P < 0.01) higher in the younger age group compared to the elderly subjects.
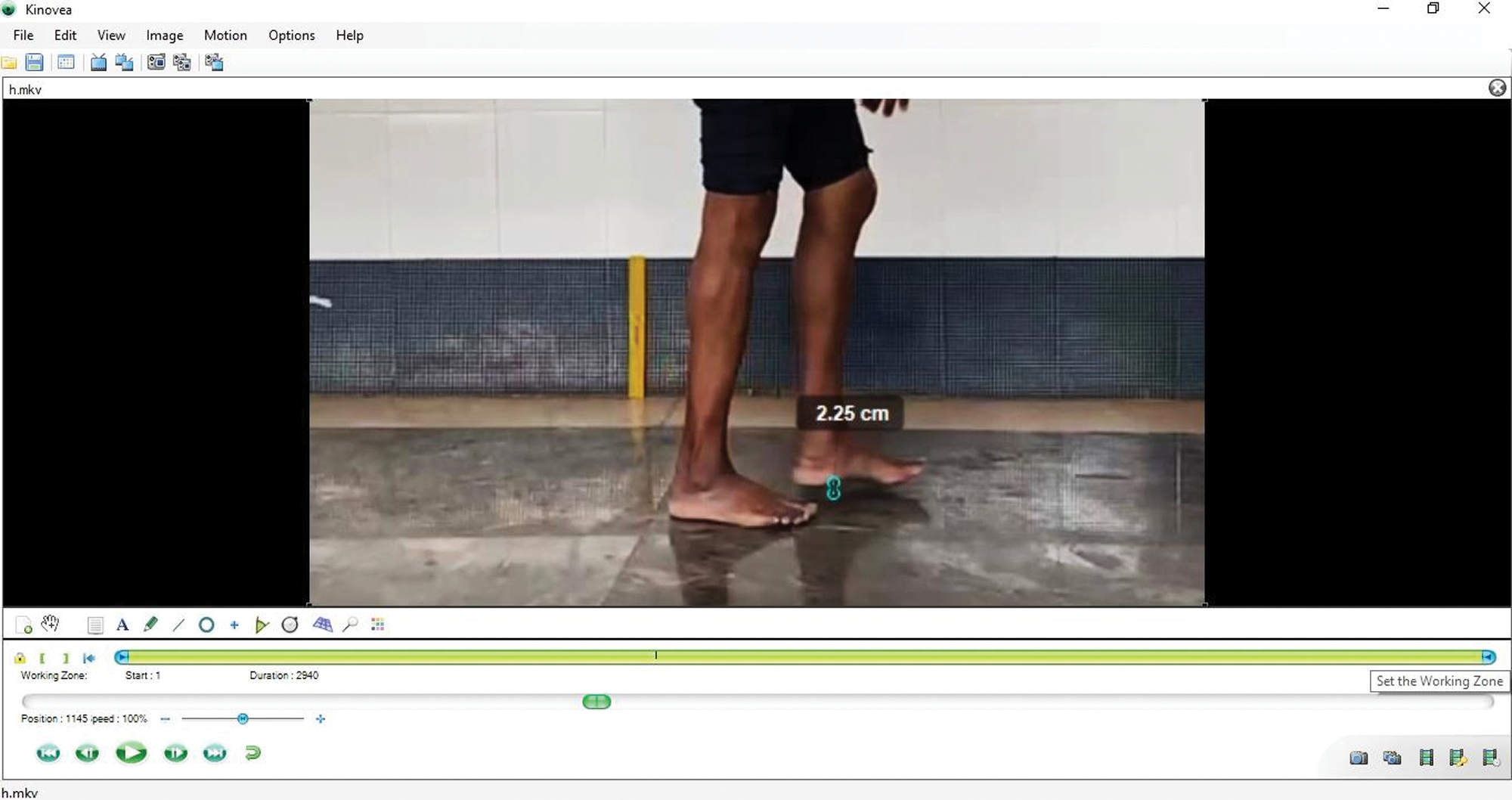
- A process for measuring foot clearance using Kinovea software (reproduction size at column width)
Knee and ankle range of motion
The knee and ankle goniometry was analyzed using the standard approach [Figure 5]. The mean knee range of motion among the younger age group was 48.91°, while in the elderly group, it was 44.44° [Table 1]. These are statistically significant, which indicates that the knee joint range of motion among the elderly is reduced when compared with the younger age group.
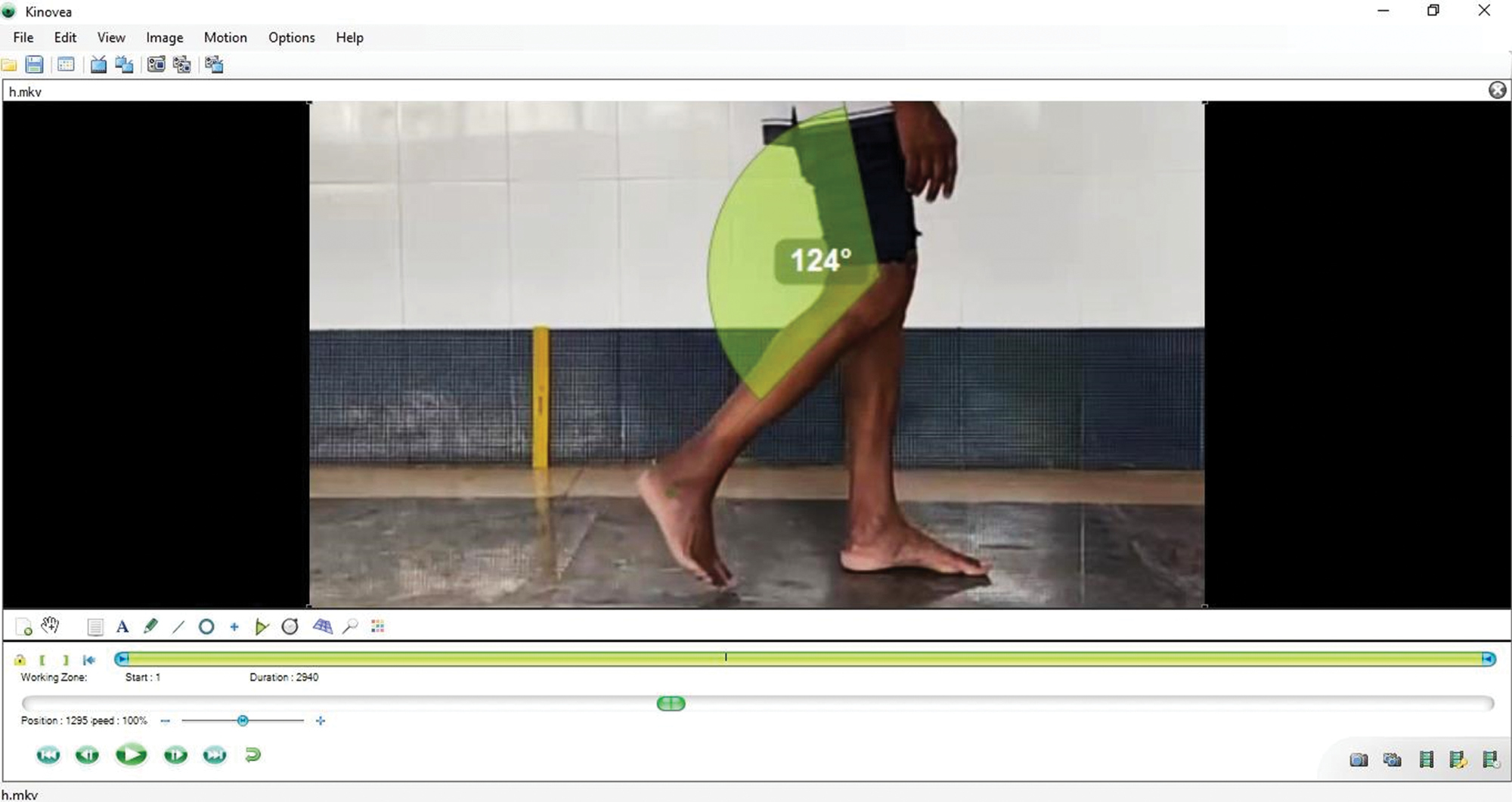
- A process for measuring knee goniometry using Kinovea software (reproduction size at column width)
The mean ankle range of motion among the younger age group was 20.20° and in the elderly group, it was 19.59° [Table 1]. However, unlike the knee joint, the movement of the ankle joint wasn’t statistically significant between elderly and younger cohorts (P > 0.05). The interobserver reliability was calculated by a team of four orthopedic specialists, and the average agreement to scores using Kappa analysis ranged from 78.4 to 94.8.
Our study results showed that elderly people had an altered gait pattern compared to the younger age group. Specifically, the elderly cohorts showed reduced stride length, foot clearance, and knee goniometry.
Discussion
Routine gait analysis, in our view, is essential for the early detection of musculoskeletal/neuromuscular diseases. However, due to the cost factor, commercially available gait analysis tools cannot be adopted for use in under-resourced tertiary care hospitals. We report here a practical and economical approach to implementing gait analysis using universally available digital tools and free access software systems. In our view, the feasibility of these indigenously adopted digital tools allows for implementing routine gait analysis practices in not only under-resourced tertiary care hospitals but also can be adopted in primary care facilities to improve the early detection of potential musculoskeletal/neuromuscular diseases.
Our indigenous approach to gait analysis demonstrated in this study is suitable for detecting all aspects of the sequence of events in a normal gait cycle, that is, the heel strike (which indicates the beginning of stance), followed by the foot flat and heel rise, until the toe-off event (which indicates the beginning of the swing phase), and the end of next heel strike.[6] In addition to the digital analysis tools, in a clinical setting, gait and mobility assessments also involve the use of standard set questionnaires, observations, and simple functional performance assessments adopted to fit for purpose to suit the local circumstances.[7] Although we didn’t test the merit of supplementing these additional clinical approaches with the digital assessments in this study, it is reasonable to foresee whether such a multidimensional approach will further refine the clinical best practice.
Typical modern gait analysis laboratories have many electronic devices and advanced software technologies, which due to their commercial nature are expensive, and lack ease of accessibility for routine use in tertiary or primary care hospitals, especially in under-resourced circumstances. However, smartphones have previously been reported to be used for gait analysis together with sensors and accelerometers.[6,8,9] These additional electronic devices are not feasible to implement in remote and small clinical settings. Alternatively, a recent study has shown that smartphones and free access software can be integrated to perform gait analysis in a clinical setting.[10] Specially in-built slow-motion video capturing technology in newer models of smartphones with a split-screen application, zoom effects with high definition, and frame-by-frame analysis of the captured videos allow for much-refined application in gait analysis. Kinovea software (version 0.9.3) is a free software distributed under a GPL v2 license and is an easily accessible and reliable tool for the analysis of digital videos.[11] Hence, we attempted to develop a smartphone-based gait analysis in our clinical setting at Coimbatore Medical College, Coimbatore, Tamil Nadu, India. Based on our analysis of 502 individuals, we have demonstrated the validity of this novel indigenous cost-effective means of gait analysis in a clinical setting. In our view, this novel indigenous cost-effective gait analysis system can be easily implemented in any tertiary or primary care hospital for routine gait analysis.
The major gait parameters used in this study were in accordance with the previously reported studies. Our observations on stride length differences between younger and elderly cohorts are in concurrence with previous reports using established methods of gait analysis.[5,7,12] However, in contrast, Blanke et al.[13] reported no significant difference in stride length between younger and elderly cohorts, which could be due to geographical differences and the influence of confounding variables. In this study, foot clearance was observed to be less in the older age group compared to younger cohorts, which is consistent with our previous report[1] in contrast to reports from other geographical regions.[7,14] The knee and ankle goniometry measurements observed in this study were consistent with a previous study performed using a commercially available gait laboratory.[13]
This study has the following limitations. Since we did not have access to a 3D gait analysis laboratory, our results from this study cohort could not be concurrently validated by a direct comparison between each of the methods. However, the consistency of the observation from this study with previous studies[7,13,14] does provide reassurance on the indirect validity of the novel indigenous approach described in this study. Therefore, we propose that using a novel indigenous approach of using smartphones with free access software can open up a new pathway without compromising the precision and accuracy required for measuring gait parameters. Further studies involving various visual parameters can be planned using such simple equipment, thereby making it accessible even to the most remote healthcare institutions and hence refining the management of various gait-related ailments.
Conclusion
Considering the limitations and lack of accessibility to the standard sophisticated gait lab, the novel indigenous approach described in this study offers a valid and promising tool for routine gait analysis in any under-resourced tertiary or primary care hospital setting.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Merit of gait patterns for early detection of risk of falls among elderly participants: A comparative analysis from India. J Nat Sci Biol Med. 2021;12:203-6.
- [CrossRef] [Google Scholar]
- A practical guide to gait analysis. J Am Acad Orthop Surg. 2002;10:222-31.
- [CrossRef] [PubMed] [Google Scholar]
- A preliminary test of measurement of joint angles and stride length with wireless inertial sensors for wearable gait evaluation system. Comput Intell Neurosci. 2011;2011:975193.
- [CrossRef] [PubMed] [Google Scholar]
- Kinematics of gait: New method for angle estimation based on accelerometers. Sensors. 2011;11:10571-85.
- [CrossRef] [PubMed] [Google Scholar]
- Gait assessment of younger and older adults with portable motion-sensing methods: A user study. Mobile Inform Syst. 2019;2019:13.
- [CrossRef] [Google Scholar]
- The smart-insole dataset: Gait analysis using wearable sensors with a focus on elderly and Parkinson’s patients. Sensors (Basel). 2021;21:2821.
- [CrossRef] [PubMed] [Google Scholar]
- 3D gait assessment in young and elderly subjects using foot-worn inertial sensors. J Biomech. 2010;43:2999-3006.
- [CrossRef] [PubMed] [Google Scholar]
- Video movement analysis using smartphones (ViMAS): A pilot study. J Vis Exp. 2017;121:54659.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability and validity of gait analysis by android-based smartphone. Telemed J E Health. 2012;18:292-6.
- [CrossRef] [PubMed] [Google Scholar]
- Usability and reliability of the Edinburgh visual gait score in children with spastic cerebral palsy using smartphone slow-motion video technology and a motion analysis application: A pilot study. JOIO. 2021;55:931-8.
- [CrossRef] [PubMed] [Google Scholar]
- International Medical Device and Technology Conference 2017 International Medical Device and Technology Conference. Malaysia: Universiti Teknologi Malaysia; 2017. p. :247-250.
- Toe clearance variability during walking in young and elderly men. Gait Posture. 2008;28:101-7.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of gait of young men and elderly men. Phys Ther. 1989;69:144-8.
- [CrossRef] [PubMed] [Google Scholar]
- Minimum foot clearance during walking: Strategies for the minimisation of trip-related falls. Gait Posture. 2007;25:191-8.
- [CrossRef] [PubMed] [Google Scholar]




