
Translate this page into:
A computed tomography-guided analysis of pedicle morphology of the lower thoracic and lumbar spine in the Indian population: An observational study
Address for correspondence: Dr. Santosh Kumar Mishra, Department of Orthopaedics, Gandhi Medical College, Bhopal - 462 001, Madhya Pradesh, India. E-mail: doctorskmishra@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Singh V, Mishra SK, Trivedi A, Tandon S, Rajpoot MS. A computed tomography-guided analysis of pedicle morphology of the lower thoracic and lumbar spine in the Indian population: An observational study. J Orthop Spine 2021;9:25-30.
Abstract
BACKGROUND:
The knowledge of morphometric characteristics of the pedicle is crucial for successful transpedicular screw fixation. Since differences are reported across various ethnic populations; hence, this study was conducted to analyze the morphometry of pedicle from D6-S1 vertebrae among the population of central India.
MATERIALS AND METHODS:
The prospective cross-sectional observational, study was conducted on 102 patients between January 2018 and March 2019 at a tertiary center in central India with spinal pathology. After the initial workup of each patient, computed tomography scan images of the dorso-lumbosacral spine were obtained. Morphometric characteristics from D6-S1 vertebrae studied in three parameters including transverse pedicle isthmus width (TPIW), pedicle length (PL), and transverse pedicle angle (TPA).
RESULTS:
In this study, the highest TPIW was observed at S1 and narrowest at T6. In the lumbar region, the widest pedicle was at L5 while in the thoracic region widest TPIW was at T12. The highest PL was observed at S1 with the minimum at T7 level. In the lumbar region, the longest mean PL was found at L2 and shortest at L5. In the thoracic region longest PL was observed at the T12 level. The mean of TPA at thoracic level was <10° except at T7 level at which its value was slightly higher. At the lumbar region, value of TPA increased gradually. There was no statistically significant association of gender with morphometric measures.
CONCLUSION:
The study includes morphometric analysis of thoracolumbar vertebrae including S1. Hence, giving a rational approach for transpedicular screw fixation taking into consideration of racial variations.
Keywords
Morphometry
pedicle length
transverse pedicle angle
transverse pedicle isthmus width
vertebrae

Introduction
Vertebrae is the set of 33 individual and interlocking bones which forms the spinal column. The dorso-lumbar part of the spine is the area of transfer of biomechanical movement in the spine, therefore, it is the area where most often pathologies are seen. These pathologies may include fracture and dislocations, degenerative diseases, osteoporotic compression fractures, neoplastic diseases, and infections. The pedicle is thick, dorsal projections from the superior part of the vertebral body and it is the strongest part of the vertebra. They are made of entirely cortical bone with a small core of cancellous bone. Pedicle screw fixation has become an increasingly popular technique of instrumentation to treat these spinal disorders by providing stable fixation.[1,2]
Pedicle screw fixation was first described by Boucher.[3] The technique for pedicle screw instrumentation of the spine has gone through significant progress over the last two decades.[2] It has several advantages over traditional hook and rod constructs, it allows the stability necessary for spinal arthrodesis and improves deformity correction due to its three-column control over the spinal elements. Pedicle screw instrumentation also obviates the need to place instrumentation within the spinal canal thus lessens the risk of neural injury.[4] The success of this technique mainly depends on the ability of the screw to maintain purchase within the body of the vertebra. Knowledge of morphometric characteristics of the pedicle is very important for the surgeon to prevent injuries to the pedicle cortex, meninges, nerve roots, joint facets, viscera, or adjacent vascular structures due to misplacement or improper orientation of the screws.[5] There are various methods for calculating morphometry of pedicle includes direct measurement in cadavers, the measurement of dry vertebrae, radiography, fluoroscopy, three-dimensional reconstruction, and magnetic resonance imaging and computed tomography (CT).[6]
As regards the morphometrical data, it is well established that same varies with different age, sex, race, ethnic, and regional group. It is observed that very few citations of morphometry of pedicles in the central Indian context are available. The current observational study is to measure the surgically relevant parameters such as transverse pedicle isthmus width (TPIW), transverse pedicle angle (TPA), and the pedicle length (PL) from D6-S1 vertebrae.
Materials and Methods
This prospective cross-sectional observational study was conducted between January 2018 and March 2019 at the Department of Orthopaedics, Tertiary Health care Center in central India. Ethical clearance was taken from the institutional ethical committee. A total of 102 patients were included in this study as per the inclusion criteria after the evaluation of all patients attending orthopedics outpatient department or Emergency during this period. All 20-70-year-old patients with fractures of lower thoracic and lumbar vertebrae, i.e., D6-S1 and those to be managed by spinal pedicle fixation were included in this study. Patients excluded were aged <20 years and more than 70 years. Nonconsenting and grave prognosis patients. Patients previously operated for spine surgeries, patients those having growth disorders, systemic bone disease, and renal disease. Furthermore, those individuals having congenital and acquired anomalies of spine, tumor, and tuberculosis of spine were excluded from the study.
After taking informed consent CT scan images of dorso-lumbosacral spine were obtained by using 128 slice CT scan machine in the supine position. Three mm cut sections or “slices” were taken in the transverse plane. The axial section of the CT image was used to measure all the parameters. The distances and angles were measured by lines drawn on the CT scan images using the option provided in the DICOM software. Measured values were directly noted from the monitor screen. Data were collected according to the patient on pretested-pro forma and master chart prepared using MS EXCEL 2016. Statistical significance was set at level P < 0.05. The mean score and standard deviation of TPIW (mm), PL (mm), and TPA (°) were calculated using Epi Info™ 7.1 software by Centre for disease control Atlanta (US). Morphometric characteristics of D6-S1 vertebrae studied in three parameters including TPIW, PL and TPA.
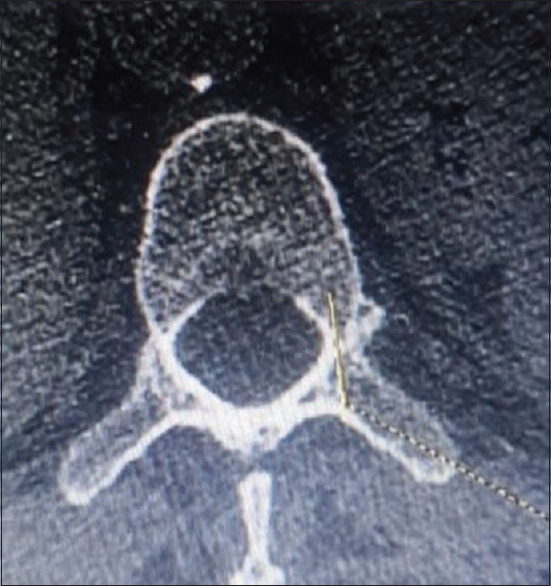
TPIW: To measure TPIW a line was drawn perpendicular to the long axis of the pedicle, at the level of its narrowest part, i.e. isthmus [Figure 1]
PL: To measure the length of the pedicle, a line was drawn along the long axis of pedicle from the posterior border of the articular facet posteriorly to the posterior border of the vertebral body anteriorly [Figure 2]
TPA: To measure TPA, a line was drawn along the long axis of pedicle and second line was drawn along the median transverse plane of vertebrae. The angle formed by the long axis of the pedicle with that of the median transverse plane was noted [Figure 3].

- Calculation of transverse pedicle isthmus width
- Calculation of pedicle length
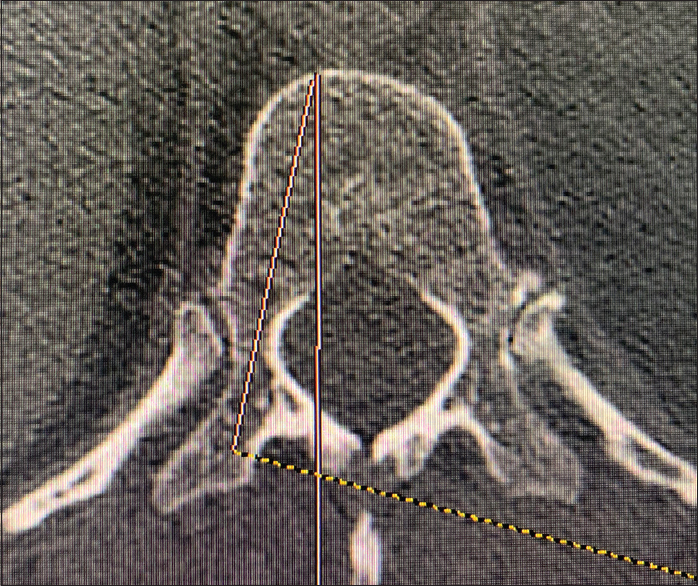
- Calculation of transverse pedicle angle
Results
In our observation, a total of 102 patients were included in the study in which 54.9% were male, with mean age of all patients was 47 years. Majority of them, i.e. 28.43% of the study population belonged to 40–50 years.
Pooled data of TPIW are shown in Table 1. In this study, the highest TPIW was observed at S1 (19.26 ± 4.36 mm) and the narrowest width was observed at T6, i.e. 4.20 ± 1.17 mm. In the lumbar region (L), the widest pedicle was at L5 while in the thoracic region (T) widest TPIW was observed at T12. The mean TPIW of T12 was higher in comparison to L1 and L2 vertebrae. In this study, the mean score comparison of TPIW (mm) in S1 was found to be more in females. The mean score comparison of TPIW in T6, T10 and T11 was found to be higher in males, whereas at T7, T8, T9 and T12 measures were higher in females. Furthermore, the mean score of TPIW in L2 and L5 was found to be higher in males. However, there was nonsignificant association of TPIW with sex was observed.
| Range | Total mean±SD | Male | Female | |
|---|---|---|---|---|
| T6 | 2.8-7.10 | 4.20±1.17 | 4.21±1.21 | 4.17±1.12 |
| T7 | 2.8-7.20 | 4.47±1.08 | 4.40±1.10 | 4.56±1.07 |
| T8 | 2.8-7.20 | 4.46±1.11 | 4.35±1.08 | 4.61±1.14 |
| T9 | 2.30-7.20 | 5.21±1.32 | 5.17±1.34 | 5.27±1.31 |
| T10 | 3.90-9.20 | 6.21±1.12 | 6.23±1.09 | 6.18±1.15 |
| T11 | 3.90-9.10 | 6.45±1.27 | 6.48±1.32 | 6.41±1.20 |
| T12 | 5.20-9.20 | 7.46±1.12 | 7.41±1.09 | 7.52±1.17 |
| L1 | 4.80-9.10 | 6.70±1.09 | 6.67±1.17 | 6.73±0.99 |
| L2 | 3.90-9.40 | 7.19±1.37 | 7.20±1.34 | 7.17±1.43 |
| L3 | 3.90-11.60 | 8.38±1.76 | 8.31±1.96 | 8.47±1.49 |
| L4 | 6.30-15.50 | 10.86±2.62 | 10.78±2.64 | 10.95±2.63 |
| L5 | 6.50-18.50 | 13.88±2.92 | 14.31±2.79 | 13.35±3.01 |
| S1 | 10.60-24.50 | 19.26±4.36 | 19.02±4.45 | 19.56±4.27 |
SD: Standard deviation
As shown in Table 2, the highest PL was observed in S1 with a mean of 19.13 mm ± 4 and minimum at T7 with a mean of 10.70 mm ± 2.23. In the lumbar region (L), the longest mean PL was found at L2 and shortest at L5. In the thoracic region, longest PL was observed at T12 level. The mean score of PL from L1-S1 was found to be higher in females. The mean PL at T7-T12 was found to be higher in males. Nonsignificant association of PL with sex was observed.
| Range | Total mean±SD | Male | Female | |
|---|---|---|---|---|
| T6 | 6.5-16.7 | 10.79±3.01 | 10.74±2.95 | 10.87±3.12 |
| T7 | 6.4-14.6 | 10.70±2.23 | 10.72±2.29 | 10.69±2.18 |
| T8 | 6.5-16.7 | 10.89±2.03 | 10.99±2.17 | 10.76±1.85 |
| T9 | 8.2-17.6 | 12.33±2.96 | 12.49±3.11 | 12.13±2.79 |
| T10 | 8.9-18.9 | 13.52±2.90 | 13.63±2.88 | 13.39±2.96 |
| T11 | 11.5-19.5 | 14.68±2.74 | 15.04±2.77 | 14.24±2.67 |
| T12 | 10.5-20.5 | 15.34±2.76 | 15.47±2.82 | 15.19±2.72 |
| L1 | 8.2-19.5 | 13.40±2.01 | 12.96±1.69 | 13.94±2.24 |
| L2 | 9.1-18.5 | 14.08±2.18 | 13.99±2.04 | 14.20±2.36 |
| L3 | 9.3-18.5 | 13.61±1.87 | 13.61±1.78 | 13.62±2.01 |
| L4 | 8.2-17.6 | 12.33±2.32 | 12.32±2.44 | 12.36±2.18 |
| L5 | 9.1-17.5 | 12.04±2.27 | 11.86±2.25 | 12.26±2.31 |
| S1 | 10.6-25.2 | 19.13±4.00 | 18.98±4.11 | 19.31±3.89 |
SD: Standard deviation
As shown in Table 3, the highest mean score of TPA° was observed at S1 (39.73°±1.90°), and narrowest at T11 (2.88°±1.35°). In the lumbar region, the widest pedicle angle was at L5 and narrowest at L1. In the thoracic region highest mean value of TPA was observed at T7. The mean score of TPA in S1 was found to be higher in females when compared to males. In the thoracic region the mean score of TPA (°) in T6, T8-T11 was found to be higher in males, while in the lumbar region the mean TPA was observed to be higher in males. However, there was nonsignificant association of TPA with sex was observed.
| Range | Total mean±SD | Male | Female | |
|---|---|---|---|---|
| T6 | 5.3-15.6 | 7.41±1.89 | 7.62±1.96 | 7.16±1.79 |
| T7 | 8.3-13.5 | 10.62±1.33 | 10.56±1.39 | 10.68±1.26 |
| T8 | 6.2-14.2 | 8.45±1.69 | 8.56±1.69 | 8.31±1.69 |
| T9 | 2.50-10.9 | 4.97±1.86 | 5.07±1.86 | 4.86±1.86 |
| T10 | 2.50-8.4 | 5.23±1.35 | 5.28±1.45 | 5.17±1.24 |
| T11 | 1.20-8.1 | 2.88±1.35 | 2.95±1.44 | 2.79±1.24 |
| T12 | 1.8-7.4 | 3.81±1.34 | 3.70±1.31 | 3.93±1.38 |
| L1 | 6.20-11.3 | 8.76±1.37 | 8.68±1.27 | 8.67±1.50 |
| L2 | 6.90-13.6 | 10.05±1.49 | 10.04±1.30 | 10.01±1.70 |
| L3 | 9.50-15.2 | 12.48±1.34 | 12.53±1.30 | 12.41±1.40 |
| L4 | 11.30-19.7 | 15.39±2.11 | 15.12±2.06 | 14.98±2.19 |
| L5 | 18.60-29.5 | 24.60±2.54 | 24.54±2.49 | 24.67±2.63 |
| S1 | 35.40-42.8 | 39.73±1.90 | 39.67±1.91 | 39.79±1.91 |
SD: Standard deviation
Discussion
In the present study, the mean TPIW of the thoracic segment (T6-T12) was found to be of a similar range as that of Singh et al.,[7] The pedicle width of the thoracic segment increased gradually from T6 to T12. They observed minimum mean TPIW at T6 level (4.33 ± 0.97 mm) and highest TPIW at T12 level, i.e. 7.43 ± 1.63 mm. As also found in the study by Lien et al.,[8] with minimum mean TPIW at T6 level (3.9 ± 0.9 mm) and maximum TPIW at T12 level, i.e.,7.7 ± 1.5 mm. Similar result was found in the study by Gangadhara[9] (T6-4.28 ± 1.04, T12–7.88 ± 1.38 mm). In another recent Indian study by Verma et al.[10] concluded that at the T6 level the mean TPIW was observed to be 3.88 mm and at T12 was 7.89 mm. This finding is similar to our observations. In another Singapore-based study by Soh et al.,[11] it was found that at T6 level the TPIW was observed to be 3.33 ± 1.1 mm and at T12 was 5.6 ± 1.4 mm. This finding is slightly dissimilar to our observations and could be due to racial differences between their population of study and the indigenous population. In the present study, TPIW of the lumbar segment increased gradually from L1 to L5 similar to the finding of the study by Tall et al.[12] They observed the minimum value of mean TPIW at L1 level, i.e. 6.9 mm and maximum value at L5 level, i.e. 15.1 mm. Similar finding was observed with the study by Sreevidya et al.,[13] Zindrick et al.,[14] and Sunny et al.[15] The findings of the study are similar to those observed by Dzierżanowski et al.,[16] they found that pedicle width increased from L1 to L5, extending from 6.1 to 13.2 mm.
Mean TPIW was higher in males at all thoracic levels in the study conducted by Singh et al.[7] This is dissimilar to the current study that has a higher mean of TPIW in males at T6, T9, and T10 levels. The results are variable as the study by Singh et al.,[7] was done on cadavers using digital Vernier calipers. Mean TPIW was found higher in females at, L1, L3, L4, and S1 levels. The current study is similar to findings observed by Alam et al.,[17] in which they found that TPIW at lumbar vertebrae were comparable except slight variation of values in the male population, but that was statistically insignificant. It was observed that the S1 level measurement had limited citation. This is comparable to a study conducted by Singel et al.[18] As compared to African studies done by Tall et al.,[12] observed higher TPIW at the lumbar region in males.
In the present study, PL of the thoracic vertebrae gradually increased from T7 to T12 vertebrae, then showed a dip from T12 to L1. The values found in the thoracic segment in our study followed similar trends as in the study by Liau et al.,[19] among Malaysian population but the values of PL observed in our study were lower, maybe due to racial variations. In the present study, the longest PL of the lumbar region was observed was at the L2 level while shortest at L5. Similar observations were made by Mughir et al.[20] They studied lumbar vertebrae morphometry among the Malaysian population and found that PL increases from L1 to L3 then decreases till L5, however values in their study were much higher than our study, which may be due to racial variation. They observed the longest pedicle at the level of L2 and L3 and the shortest at L5.
The present study has observed that PL of T7-T12 was more in males which is contrary to the study by Singh et al.,[7] although the result of both studies were statistically insignificant. The PL of lumbar vertebrae was higher in females as also seen by Tall et al.[12] However, gender was insignificantly related to PL in both the studies.
In the present study, we observed the pedicles were angulated more medially initially and faced laterally at T11 and T12 region. Mean TPA of T9 to T12 vertebrae was less than T6, T7, and T8 vertebrae. Similar observation was found in the study by Pai et al.,[21] Zindrick et al.,[14] and Liau et al.[19] Mean TPA are comparable in all the studies and it is <10° from T6-T12. From T11 to T12, there is minimum TPA in all the studies including the current one. In the study conducted by Zindrick et al.,[14] and Liau et al.,[19] TPA value of lower thoracic vertebrae (T11, T12) were found to approaching zero and negative in some patients. But no negative value of TPA was observed in our study. In our study mean TPA at the lumbar region gradually increased from L1 (8.76° ±1.37°) to L5 (24.60° ±2.54°). The findings are similar to these observed by Mohanty et al.,[22] mean TPA gradually increased from L1 through L5 from 8.5° to 30°. In the study by Grivas et al.,[23] mean TPA increased from thoracic vertebrae to L5 vertebrae. The widest TPA was found at the L5 vertebrae with a mean angle of 26.23° ±2.65° for males and 23.63° ±4.59° for females. The narrowest TPA in males was at T12, while in females was at T9.
On comparing the data with the study by Stockton et al.,[24] it was observed that mean TPA from L1 to L5 was increasing. However, actual values were higher in above-mentioned study. This difference may be due to racial variation. However, in the case of L5 mean TPA was almost similar. Mean TPA of the lumbar region in our study from L1 to L5 was similar to the study conducted by Acharya et al.,[25] in the Indian population. Almost, similar finding was observed in the study Lien et al.[8]
In the present study, the mean score of TPA (°) in T6, T8, T9, T10, and T11 was found to be higher in males. In the study by Mistri[26] higher TPA was observed in male patients in T9 to T12 vertebrae only. In the lumbar region, the mean score of TPA in L1, L2, L3, and L4 was found to be higher in males, while for L5 it was found to be higher in females. Similar trend was found in the study by Tall et al.,[12] and Mughir et al.[20] This finding was slightly different from as observed by Chawla et al.,[27] in the Indian population the pedicle angles of L1, L4 and L5 were higher in males than females, while L3 has equal values in both males and females.
Conclusion
A key to a successful transpedicular screw insertion requires determination of length, size, and angle of insertion of pedicle screw which ensures correct placement of screw, hence avoiding intraoperative events and postoperative complications. As there are limited citation of morpho-metric analysis of pedicle of S1 vertebrae. This study helps to overcome this lacuna. It also helps in assessing morphometry of thoracolumbar vertebrae of residents of central India which had not been studied in past. It also gives spectrum of variation across various racial groups.
Limitations
The study could not establish any co-relation between variation in height and weight with the morphometric assessment of pedicle of thoraco-lumbar vertebrae. No correlation was established between the diameter of screw used, PL, angulation with preoperative findings. Furthermore, measurement of the pedicle was not analyzed separately for the right and left sides.
Financial support and sponsorship
Nil.
Acknowledgment
Personnel of Department of Radiodiagnosis, Gandhi Medical College Bhopal.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Osteosynthesis of thoraco-lumbar spine fractures with metal plates screwed through the vertebral pedicles. Reconstr Surg Traumatol. 1976;15:2-16.
- [Google Scholar]
- Plating of thoracic, thoracolumbar, and lumbar injuries with pedicle screw plates. Orthop Clin North Am. 1986;17:147-59.
- [CrossRef] [PubMed] [Google Scholar]
- A method of spinal fusion. J Bone Joint Surg Br. 1959;41-B:248-59.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy of pedicle screw placement in lumbar vertebrae. Spine (Phila Pa 1976). 1996;21:1320-4.
- [CrossRef] [PubMed] [Google Scholar]
- Determination of the length of anteromedial screw trajectory by measuring interforaminal distance in the first sacral vertebra. Spine (Phila Pa 1976). 2004;29:1608-11.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of radiographic and computed tomographic measurement of pedicle and vertebral body dimensions in Koreans: The ratio of pedicle transverse diameter to vertebral body transverse diameter. Eur Spine J. 2011;20:414-21.
- [CrossRef] [PubMed] [Google Scholar]
- Morphometric measurements of cadaveric thoracic spine in Indian population and its clinical applications. Asian Spine J. 2011;5:20-34.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of anatomic morphometry of the pedicles and the safe zone for through-pedicle procedures in the thoracic and lumbar spine. Eur Spine J. 2007;16:1215-22.
- [CrossRef] [PubMed] [Google Scholar]
- Determination of transpedicular screw parameters with the help of pedicle morphometry of thoracic vertebrae for safe transpedicular screw fxation - A cadaveric study. J Evol Med Dent Sci. 2013;36:6807-15.
- [CrossRef] [Google Scholar]
- Thoracic pedicle morphometry of dry vertebral columns in relation to trans-pedicular fixation: A cross-sectional study from central India. Cureus. 2020;12:e8148.
- [CrossRef] [Google Scholar]
- Morphological parameters of the thoracic pedicle in an asian population: A magnetic resonance imaging-based study of 3324 pedicles. Global Spine J. 2021;11:437-41. doi:10.1177/2192568220906137
- [CrossRef] [PubMed] [Google Scholar]
- Morphometric study of the lumbar spray in the African black west subject: Interest in surgery. About a CT scans of 170 cases in Ouagadougou (Burkina Faso) Open J Orthop. 2018;8:190-9.
- [CrossRef] [Google Scholar]
- Study of lumbar vertebrae with respect to the dimensions of the pedicle in South Indian population. Indian J Basic Appl Med Res. 2017;6:523-30.
- [Google Scholar]
- Analysis of the morphometric characteristics of the thoracic and lumbar pedicles. Spine (Phila Pa 1976). 1987;12:160-6.
- [CrossRef] [PubMed] [Google Scholar]
- Study of pedicle morphometry of the lumbar vertebrae. Int J Allied Med Sci Clin Res. 2016;4:284-8.
- [Google Scholar]
- Morphometric analysis of the lumbar vertebrae concerning the optimal screw selection for transpedicular stabilization. In: Pokorski M, ed. Advances in Medicine and Medical Research. Advances in Experimental Medicine and Biology. Vol 1133. Cham: Springer; 2019.
- [Google Scholar]
- Lumbar morphometry: A study of lumbar vertebrae from a pakistani population using computed tomography scans. Asian Spine J. 2014;8:421-6.
- [CrossRef] [PubMed] [Google Scholar]
- A study of width and height of lumbar pedicles in Saurashtra region J Anat Soc India. 2004;53:4-9.
- Computed tomographic morphometry of thoracic pedicles: Safety margin of transpedicular screw fixation in malaysian malay population. Spine (Phila Pa 1976). 2006;31:E545-50.
- [CrossRef] [PubMed] [Google Scholar]
- Morphological comparison between adolescent and adult lumbar pedicles using computerised tomography scanning. Surg Radiol Anat. 2010;32:587-92.
- [CrossRef] [PubMed] [Google Scholar]
- Morphometric analysis of the thoracic pedicle: An anatomico-radiological study. Neurol India. 2010;58:253-8.
- [CrossRef] [PubMed] [Google Scholar]
- Morphometry of the lower thoracic and lumbar pedicles and its relevance in pedicle fixation. Musculoskelet Surg. 2018;102:299-305.
- [CrossRef] [PubMed] [Google Scholar]
- Morphometric characteristics of the thoracοlumbar and lumbar vertebrae in the Greek population: A computed tomography-based study on 900 vertebrae-“Hellenic Spine Society (HSS) 2017 Award Winner”. Scoliosis Spinal Disord. 2019;14:2.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of lumbar transverse pedicle angles between ethnic groups: A retrospective review. BMC musculoskeletal disorders.. 2019;20:114.
- [CrossRef] [PubMed] [Google Scholar]
- Lower dorsal and lumbar pedicle morphometry in Indian population: A study of four hundred fifty vertebrae. Spine (Phila Pa 1976). 2010;35:E378-84.
- [CrossRef] [PubMed] [Google Scholar]
- Lower thoracic and lumbar pedicle morphometry using computerized tomography scan. Indian J Basic Appl Med Res. 2016;5:236-48.
- [Google Scholar]
- Importance of transverse pedicle angle and chord length of lumbar pedicle in screw placement: A CT scan study on North West Indian population. Eur J Anat. 2013;17:230-6.
- [Google Scholar]




