
Translate this page into:
A comparative study of functional and radiological outcome on aperture versus suspensory femoral fixation in Arthroscopic ACL reconstruction
*Corresponding author: Varrdhaman H Dhariwal, Department of Orthopaedics, Stanley Medical College, Old Washarmanpet, Chennai, Tamil Nadu, India varrdh@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dhariwal VH, Mohan Kumar K, Rajagopal N, T. Tholgapiyan. A comparative study of functional and radiological outcome on aperture versus suspensory femoral fixation in Arthroscopic ACL reconstruction. J Orthop Spine. 2025;12:1. doi: 10.25259/Joasp_44_23
Abstract
Objectives
To compare and find the superiority between aperture and suspensory of femoral fixation in ACL reconstruction.
Material and Methods
A comparative study with a study population with 30 in each group with Tengner Lyscholm and International Knee Documentation Committee (IKDC) subjective scoring between each group for a followup of 3 years.
Results
No statistically significant difference between two groups functionally and radiologically.
Conclusion
Both methods are equally good if correct surgical techniques are followed in both groups.
Keywords
Arthroscopic ACL reconstruction
Comparison
Endo button femoral fixation
Interference screw

INTRODUCTION
Arthroscopic ACL reconstruction is a commonly done procedure with various modalities of femoral fixation. Various modalities of femoral fixations are interference screw, Endo button, and trans condylar fixation. Among these modalities, we compared the functional outcome between aperture (interference screw) and suspensory fixation (Endo button).
MATERIAL AND METHODS
Retrospective study 78 patients, out of which 18 were lost in follow-up, accounting for 30 in each group done by a single author over the period of five years between interference screw and Endo button at an interval of three months, six months, one year, two years, and three years at Government Stanley Medical College.
Inclusion criteria
Complete ACL tear clinically and radiologically
Age: 15–60 years
Examined by a single surgeon
Beighton's score is <6
Exclusion criteria
Beighton's score is >6
Chondral lesion
Infection
Multi-ligament injury
Previous knee surgery
All the included patients were clinically assessed, diagnosed, and confirmed with magnetic resonance imaging (MRI). They had Positive Lachmann and Anterior drawer test positive. Our data sheet contains pre-op and intra-op and anaesthesia and Lachhman and anterior drawer test positive for all patients. All underwent diagnostic arthroscopy with the standard anterolateral portal.
Surgical technique
Hamstring graft was harvested (semi T and Gracilis) for all patients and quadrupled and sutured with five Ethibond proximally and distally for the interference screw. For the Endo button group, proximally Endo button was placed and distal sutured with Ethibond no. 5. A femoral tunnel was made with a femoral zig of 6 mm offset at 130° of knee flexion. The tibial tunnel was made with an outside-in technique in standard fashion and all patients received a tibial titanium interference screw.
Post-op rehab
Both groups had the same rehab program with a long knee brace. Quadriceps and ankle foot exercises were done on the second day. Closed chain exercises and focusing on achieving full extension in the initial two weeks. Weight-bearing was allowed at three weeks post-op for both groups.
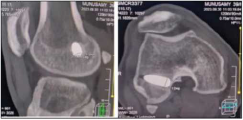
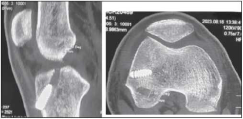
Knee flexion up to 90° was allowed for up to an initial four weeks, and later deep flexion was allowed after six weeks when the strength had regained, and the international knee documentation committee (IKDC) subjective score, Tegner Lyscholm score, radiograph, and computed tomography (CT) scan were done at three months, six months, one year, two years, and three years.
RESULTS
The choice of the implant between suspensory fixation and aperture fixation does not have any significant difference in the functional outcome even after five years. No statistically significant difference is in mean post-op Lyshome Tegnar at three-month, six-month, one-year, two-year, and three-year intervals between the two groups by independent t-test statistics. No statistically significant difference is in mean post-op IKDC between the two groups by independent t-test statistics. No statistically significant difference is in mean femoral tunnel diameter in the third year between the two groups by independent t-test statistics. This study implies usage of both in ACL reconstruction has produced equivocal results in both groups suggesting the use of both implants for the management of arthroscopic ACL reconstruction.
DISCUSSION
ACL injury is usually treated with a hamstring, quadriceps tendon, or bone patella tendon graft. The hamstring graft since its harvesting is relatively easier; it is commonly done. Since the quadrupled hamstring graft has a strength of 4,108N and a stiffness of 807N, it is now more preferred. As there is less chance of patellar fracture, extensor apparatus weakness and anterior knee pain are present in the bone patellar tendon bone graft (BPTB) graft less with a hamstring. Gobbi A et al. showed that the BPTB graft is 3.76 times stiffer than the native ACL.1,2 Hence hamstring is the preferred choice due to its strength and closer to liner stiffness.
There are mainly two types of fixations done in our institution with an interference screw (aperture) and another with suspensory (Endo button fixation). The main purpose of this fixation is for good healing of the graft in a bone tunnel. This transforms into early mobilization of the graft early weight bearing and aggressive rehab of the patient and return to sports. Aperture fixation (interference screw) is supposed to be superior fixation to suspensory fixation3 like Endo button or staples or transfix. The rate of success for various modalities ranges from 65% to 90%. The fixation choice is mainly surgeon-dependent and recently due to unleash of information by Google and AI it is becoming patient choice-dependent. In the Endo button, the point of fixation is away from the joint, which is prone to tunnel enlargement due to the bungee effect4 and windshield wiper effect5 the suspensory fixation has a high failure load and tunnel widening due to micromotion of the graft in the tunnel and anterior joint laxity. Similarly, interference screw also has problems6–12 like tunnel widening, graft rotation, abscess formation, abrasion, problems in imaging, and graft damage with soft tissue grafts yet, now recently the interference screws the bioabsorbable are used more but Drogset JO et al.13 has found not much difference between metal and bioabsorbable usage clinically. But tunnel widening is seen mostly in both groups on the femoral groups. In our study, we have used both aperture (interference screw) and suspensory (Endo button cl). Insw our study, both groups have improved function and improved patient satisfaction both in short-term and medium-term groups up to three years. Although there were reports of graft cutout in the interference screw group, we did not have even a single cutout because we used whip stitches with five ethibond, and inserted the same size of the screw in which the size the tunnel was drilled [Figures 1–6].



![(a) Quadruple hamstring graft technique. (b) Graft preparation [Quadreupled Hamstring graft with whip stitches (so that the interference screw doesn't cut out the graft) in the proximal and distal part]. (c) Femoral socket drilling using femoral offset guide.](/content/178/2025/12/1/img/JOASP-12-1-g004.png)
| Group | N | Mean | SD | Minimum | Maximum |
| IS | 30 | 93.2 | 0.9 | 91 | 95 |
| EB | 30 | 92.9 | 0.9 | 91 | 94 |
EB: Endobutton, IS: Interference screw, SD: Standard deviation
| Group | N | Mean | SD | Minimum | Maximum |
| IS | 30 | 93.7 | 0.9 | 92 | 95 |
| EB | 30 | 93.4 | 0.9 | 92 | 95 |
EB: Endobutton, IS: Interference screw, SD: Standard deviation
| Group | N | Mean | SD | Minimum | Maximum |
| IS | 30 | 94.4 | 0.9 | 92 | 96 |
| EB | 30 | 93.9 | 0.9 | 92 | 95 |
EB: Endobutton, IS: Interference screw, SD: Standard deviation
| Group | N | Mean | SD | Minimum | Maximum |
| IS | 30 | 8.01 | 0.03 | 8.0 | 8.1 |
| EB | 30 | 8.0 | 0.0 | 8.0 | 8.0 |
EB: Endobutton, IS: Interference screw, SD: Standard deviation
| Group | N | Mean | SD | Minimum | Maximum |
| IS | 30 | 80.7 | 1.2 | 79 | 83 |
| EB | 30 | 81.4 | 1.8 | 80 | 90 |
EB: Endobutton, IS: Interference screw, SD: Standard deviation
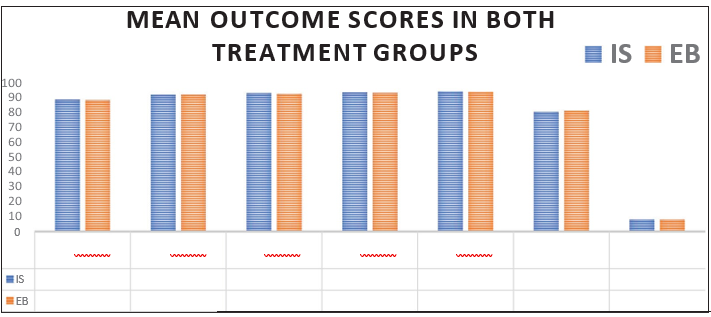
We need to study this with more detail with multicentric and large volume with longer follow-up to prove this analogy that both have no difference in outcome. Our study concludes that both treatment groups are similar with respect to age, gender, and mode of injury with no statistical differences between them. Post-operative follow-up with Tegnar and Lysholm scores at one, two, and three years find no statistically significant difference. Also, there is no significant difference in the mean femoral tunnel diameter in the third year between both groups.
CONCLUSION
In our study, we retrospectively compared radiological and functional outcomes between the interference screw and the Endo button fixation for femoral fixation. We found no difference in outcomes between both groups, provided meticulous technique was followed.
Ethical approval
The research/study approved by the Institutional Review Board at Govt stanley medical college, number 24032021007, dated 24th March 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using the AI.
REFERENCES
- Bomechanical comparison of quadriceps and patellar tendon grafts in anterior cruciate ligament reconstruction. Arthroscopy. 2016;32:71-5.
- [CrossRef] [PubMed] [Google Scholar]
- Patellar tendon anterior cruciate ligament reconstruction with conical press-fit femoral fixation: 5-year results in athletes' population. Knee Surg Sports Traumatol Arthrosc. 2002;10:73-9.
- [CrossRef] [PubMed] [Google Scholar]
- Is all-inside with suspensory cortical button fixation a superior technique for anterior cruciate ligament reconstruction surgery? A systematic review and meta-analysis. BMC Musculoskelet Disord. 2020;21:445.
- [CrossRef] [PubMed] [Google Scholar]
- Tunnel widening after ACL reconstruction with different fixation techniques: Aperture fixation with biodegradable interference screws versus all-inside technique with suspensory cortical buttons. 5-year data from a prospective randomized trial. Arch Orthop Trauma Surg. 2023;143:6707-18.
- [CrossRef] [PubMed] [Google Scholar]
- Editorial commentary: Tunnel widening after anterior cruciate ligament reconstruction may increase laxity and complicate revision. Arthroscopy. 2021;37:2564-66.
- [CrossRef] [PubMed] [Google Scholar]
- Press-fit fixation using autologous bone in the tibial canal causes less enlargement of bone tunnel diameter in ACL reconstruction—A CT scan analysis three months postoperatively. BMC Musculoskelet Disord. 2015;16:200.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical modeling of a bone tunnel enlargement post ACL reconstruction. bioRxiv 2020:2020-09.
- [CrossRef] [Google Scholar]
- An analysis of the biomechanics of interference screw fixation and sheathed devices for bicseps tenodesis. Clin Biomech. 2015;30:551-7.
- [CrossRef] [PubMed] [Google Scholar]
- Migration of “bioabsorbable” screws in ACL repair. How much do we know? A systematic review. Knee Surg Sports Traumatol Arthrosc. 2013;21:986-94.
- [CrossRef] [PubMed] [Google Scholar]
- Sterile pretibial abscess after anterior cruciate reconstruction from bioabsorbable interference screws: A report of 2 cases. Arthroscopy. 2007;23:911.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging ACL reconstructions and their complications. Diagnostic Interv Imaging. 2015;96:11-9.
- [CrossRef] [PubMed] [Google Scholar]
- Interference screw divergence in femoral tunnel fixation during endoscopic anterior cruciate ligament reconstruction using hamstring grafts. Arthroscopy. 2002;18:510-4.
- [CrossRef] [PubMed] [Google Scholar]
- A prospective randomized study of ACL-reconstructions using bone-patellar tendon-bone grafts fixed with bioabsorbable or metal interference screws. Knee Surg Sports Traumatol Arthrosc. 2011;19:753-9.
- [CrossRef] [PubMed] [Google Scholar]




