
Translate this page into:
A comparative study between conventional and minimally invasive dynamic hip screw fixation in management of intertrochanteric femoral fractures
Address for correspondence: Dr. Ashish Gohiya, F1 Doctors Quarter, Hamidia Hospital Campus, Bhopal - 462 001, Madhya Pradesh, India. E-mail: gohiya@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gohiya A, Sharma P, Verma R, Gaur S. A comparative study between conventional and minimally invasive dynamic hip screw fixation in management of intertrochanteric femoral fractures. J Orthop Allied Sci 2016;4:36-9.
Abstract
Introduction:
The intertrochanteric fractures of femur are commonly fixed using dynamic hip screw using a conventional open Dynamic Hip Screw (CDHS). This is associated with a long incision, blood loss, considerable soft tissue trauma and pain. All these problems can be avoided using minimally invasive Dynamic Hip Screw (MIDHS), which has a theoretical advantage of less blood loss, soft tissue trauma, and early rehabilitation. Thus, we conducted a prospective comparative study of the two techniques.
Materials and Methods:
This is a prospective comparative study conducted over a period of 2 years at Department of Orthopedics GMC Bhopal. Fifty patients in the age group of 50-80 years who presented with intertrochanteric femur fracture and fulfilled inclusion criteria were divided into two groups of 25 each for fixation by CDHS or MIDHS. Patients in both the groups were matched. The data analysis was performed using SPSS package.
Results:
The patients in minimally invasive group had shorter operative time (45 min vs. 75 min). The average postoperative blood loss in drain in conventional group was 150 ml whereas no drain was used in minimally invasive group. Postoperatively need for analgesic was significantly lower in minimally invasive group (P < 0.05). Duration of hospital stay was significantly less with minimally invasive technique. The duration of bony union was similar in both techniques.
Conclusion:
Our study concludes that the minimally invasive technique of fixation of Intertrochanteric femur fractures is superior in terms of less operating time and less duration of hospital stay.
Keywords
Hospital stay
intertrochanteric fracture
minimally invasive dynamic hip screw
postoperative pain

Introduction
The fractures of the hip are among the most common fractures encountered in the elderly population.[1] As the life expectancy has increased over the years, the incidence of hip fractures has also increased.[2] The intertrochanteric fractures comprise 50% of the fractures around the hip.[3] These intertrochanteric fractures have a 15-20% risk of mortality because of the complications of prolonged immobility.[3] Thus, stabilization with dynamic hip screw (DHS) with a four hole side plate is used for stable fractures in most centers.[4,5]
The conventional open technique (conventional DHS [CDHS]) requires a long incision and thus considerable soft tissue trauma, significant blood loss and pain. To overcome the shortcomings of CDHS a minimally invasive technique (MIDHS) has been advocated recently. This technique has a theoretical advantage of decreased blood loss, less pain, and rapid rehabilitation. We conducted a prospective study to compare these two techniques.
Materials and Methods
This is a prospective comparative study done over a period of 2 years at Department of Orthopedics at a Tertiary Care Center.
Patients presenting to Department of Orthopedics with intertrochanteric fractures were evaluated and analyzed to be included in the study. Fifty patients who presented with an intertrochanteric femur fracture and who fulfilled the inclusion criteria were enrolled in the study. The patients were divided into two groups of 25 each for fixation by open or minimally invasive techniques.
The inclusion criteria were as follows:
Age: 50-80 years
Stable intertrochanteric fracture (AO 31A1, 31A2.1, 31A2.2)
Unilateral fractures.
Exclusion criteria were as follows:
Age <50 and >80 years
Unstable intertrochanteric fractures (AO 31A2.3, 31A3)
Pathological fractures
Any other associated fractures or injury
Patients requiring intensive care.
The study was approved by Institutional Ethical Committee. Patients were assigned one of the two, CDHS group or MIDHS group. Patient's details were recorded in the standard proforma. Patients in both the groups were matched with respect to age and preoperative morbidity. Patients in both the groups were worked up for surgery as per the standard protocol. All patients were operated under spinal anesthesia. After induction, patients were placed on fracture table and under C arm image intensifier reduction was checked, standard scrubbing and painting draping was done. In conventional group, the patients were operated by a long incision over lateral aspect of proximal femur, guide wire passed from the lateral surface into the middle of neck and head of femur under C arm guidance reaming done and lag screw of appropriate size passed over guide wire. Over lag screw 135°, four hole standard barrel side plate slided and fixed with 4.5 mm cortical screw of appropriate size. Wound was washed and sutured in layers over a suction drain and dressed.
In MIDHS group entry point on the lateral femoral surface was identified with the help of C arm image intensifier and a 5 cm incision was given. The fascia was cut, vastus laterlalis muscle was separated, and an obliquely cut 50 cc syringe was inserted to make a sleeve [Figure 1]. A guide wire was passed in the center of head and neck of femur, reaming was done over the guide wire. A lag screw of appropriate size was passed over the guide wire [Figure 2]. Four hole 135° standard barrel side plate was inserted first beneath the muscle then over the guide wire slided over the lag screw. The plate was fixed with 4.5 mm cortical screw of appropriate size. The wound was washed, sutured and dressed without a drain.

- Sleeve made up of cut syringe

- Position of dynamic hip screw
Intraoperatively, operative time, flouroscopic exposure time and blood loss during surgery was noted.
In postoperative period severity of pain as assessed by Visual Analogue Scale (VAS), drop in hemoglobin level and duration of hospital stay was noted.
Postoperative management was similar in both the groups and as per the standard protocol. The patients in both the groups were followed up for a minimum period for 6 months. During follow-up pain severity was assessed and time to ambulation was noted along with time to union and any complication.
Statistics
The data were evaluated using IBM SPSS 18 software. Student's t-test for two independent means and Mann-Whitney U-test was employed as a test of significance.
Results
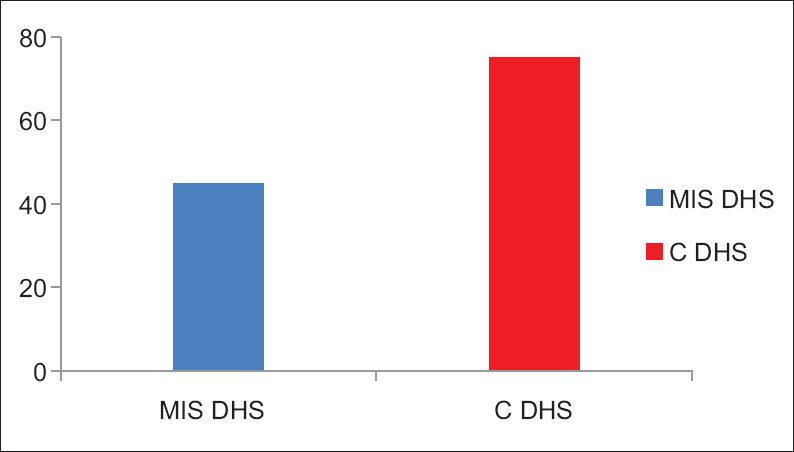
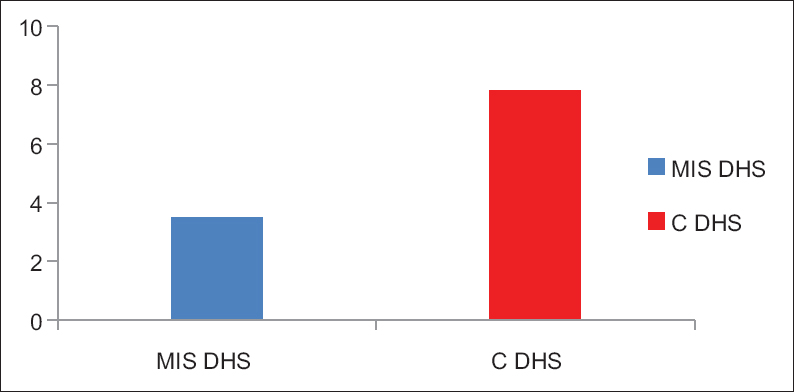
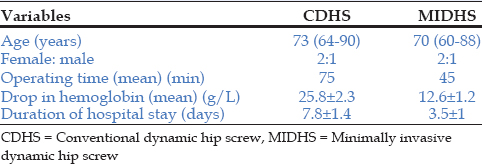
The mean age of patients in the CDHS group was 73 years whereas in the minimally invasive group it was 70 years. The female to male ratio was 2:1 in both the groups. The mean operative time was 45 min in the minimally invasive group and 75 min in the conventional group [Figure 3]. The difference in operative time was statistically significant with a P value of 0.001. The average postoperative blood loss was 150 ml in the conventional group whereas no drain was put in the minimally invasive group. The mean drop in hemoglobin postoperatively was 12.6 ± 1.2 g/l in MIDHS group whereas in CDHS was 25.8 ± 2.3 g/l [Figure 4]. This difference in the drop in hemoglobin level is statistically significant with P < 0.005 Z score is −6.0012. The patients in both the groups were put on analgesia as per our institutional protocol. The VAS showed no significant difference on the first postoperative day for patients in both the groups. On the second and third postoperative day, the patients in MIDHS group scored low on the scale (P = 0.02). The duration of stay in hospital was 3.5 ± 1 days in the minimally invasive group whereas it was 7.8 ± 1.4 days in the conventional group [Figure 5]. The difference in duration of hospital stay was statistically significant with a P < 0.001. The mean time to bony union was 8-week ± 10 days in the MIDHS group whereas in the conventional group it was 9 weeks ± 11 days. This difference in time to bony union was not statistically significant [Table 1].
- Mean operative time (in minutes)
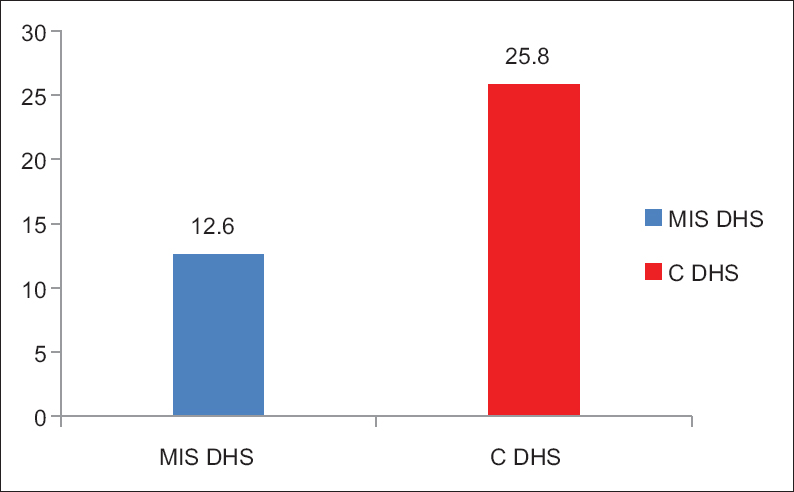
- Mean drop in haemoglobin (in g/l)
- Mean hospital stay (in days)
Discussion
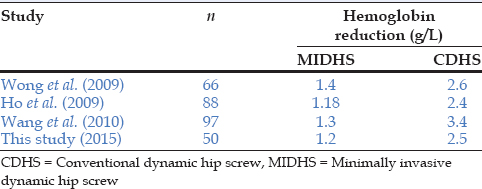
Fractures around hip constitute majority of fractures in the elderly. Intertrochanteric fractures are treated with DHS universally with good stabilization. As these fractures occur commonly in elderly who already have comorbid medical conditions; early ambulation, less duration of hospital stay and better pain control are the postoperative goals. The conventional surgical technique requires large incision, more tissue dissection resulting in considerable amount of blood loss and thus requiring blood transfusion and prolonged analgesia for pain control.[6] All these intraoperative and postoperative factors increase the duration of hospital stay and thus the overall cost of surgery. Thus minimally invasive technique has been considered desirable, as it is associated with a smaller incision, less blood loss, better pain control and lesser duration of hospital stay.[7] Less blood loss in minimally invasive technique is attributed to a smaller incision in the safe vascular zone.[6,8] In our study, the postoperative drop in hemoglobin was significantly more in the CDHS technique as compared to minimally invasive technique [Table 2] which indicates more blood loss in the intraoperative period and beyond. Similar results were found in comparative studies done by Ho et al., Wang et al. and Wong et al.[6,8,9]
The mean operative time in our study in the minimally invasive group was 45 min, which was significantly less than the conventional group, similar results were found in the study done by Zhou et al.,[7] Mahmood et al.[10] MIDHS group had significantly better pain scores than the conventional group. The requirement for analgesics was less from second postoperative day onward in the minimally invasive group. In a randomized control study done by Alobaid et al.[11] similar results were found. A comparative study done by Agrawal et al.[12] and Lee et al.[2] also showed less use of analgesics in the minimally invasive group. The duration of hospital stay was significantly less in the minimally invasive group in our study [Table 1], which is also a universal finding in the all studies done.[7,8,9]
The time to bony union, desirable screw position and reduction achieved were not significantly different with the P > 0.05. Different studies also have similar results of time to bony union and reduction.[2,7,11]
The intertrochanteric fractures occur in elderly patients with cardiovascular co morbidities, early ambulation and less use of analgesics after MIDHS will definitely lead to less postoperative complications and thus an early discharge.
Conclusion
A MIDHS technique offers the advantage of less dissection, less blood loss, less pain thus less use of analgesics. All these factors lead to lesser duration of hospital stay thus less economic burden to health system and better outlook for already morbid elderly patients in whom the majority of intertrochanteric fracture occur.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Hip fractures in the elderly: A world-wide projection. Osteoporos Int. 1992;2:285-9.
- [CrossRef] [PubMed] [Google Scholar]
- The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995;77:1058-64.
- [CrossRef] [PubMed] [Google Scholar]
- Dynamic hip screw in the treatment of intertrochanteric fractures: A comparison of two fixation methods. Int Orthop. 2007;31:683-8.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical outcomes and treatment of hip fractures. Am J Med. 1997;103:51S-63S.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive dynamic hip screw for fixation of hip fractures. Int Orthop. 2009;33:555-60.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive versus conventional dynamic hip screw for the treatment of intertrochanteric fractures in older patients. Orthopedics. 2012;35:e244-9.
- [CrossRef] [Google Scholar]
- Minimally invasive technique versus conventional technique of dynamic hip screws for intertrochanteric femoral fractures. Arch Orthop Trauma Surg. 2010;130:613-20.
- [CrossRef] [PubMed] [Google Scholar]
- A double-blind, prospective, randomised, controlled clinical trial of minimally invasive dynamic hip screw fixation of intertrochanteric fractures. Injury. 2009;40:422-7.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison between conventional and minimally invasive dynamic hip screws for fixation of intertrochanteric fractures of the femur. ISRN Orthop. 2013;2013:484289..
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive dynamic hip screw: Prospective randomized trial of two techniques of insertion of a standard dynamic fixation device. J Orthop Trauma. 2004;18:207-12.
- [CrossRef] [PubMed] [Google Scholar]
- Modified minimally invasive approach for dynamic hip screw fixation. Eur J Orthop Surg Traumatol. 2011;21:375-9.
- [CrossRef] [Google Scholar]




