
Translate this page into:
A clinico-epidemiological study on trauma cases attending a tertiary care hospital in North India
Address for correspondence: Dr. Kriti Mohan, Rishikesh - 249 203, Uttarakhand, India. E-mail: kriti.mohan@rediffmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Bharti A, Mohan K, Singh RK, Vajpai IN, Midha T, Diwedi A. A clinico-epidemiological study on trauma cases attending a tertiary care hospital in North India. J Orthop Allied Sci 2019;7:17-21.
Abstract
OBJECTIVES:
Injuries are the leading cause of death in the first four decades of life and the third leading cause of death among all patients. Road traffic accidents (RTAs) is the most common cause of injury in India with varied reports of mortality ranging from 7% to 45%. There are several scoring systems to evaluate the severity of injury and predict mortality. However, the reliability of injury score as a mortality predictor is challenging. The purpose of this study was to assess the cause of trauma with its epidemiological correlates and to categorize patients of trauma using the New Injury Severity Score (NISS) and Injury Severity Score (ISS) with their comparison in terms of mortality prediction in the present scenario of trauma in India.
MATERIALS AND METHODS:
Between October 2015 and March 2017, 5122 injured patients meeting the inclusion criteria were enrolled in this prospective longitudinal study. Data of the patients were recorded as per the working pro forma; detailed description of injury, treatment given, ISS and NISS, and ultimate outcome (mortality occurring within 30 days) was documented at the time of arrival/admission and stay at the hospital. Patients were divided into the score groups of 0–8, 9–15, 16–25, 26–49, and ≥50. The patients who were discharged or referred to a higher center were also followed up to 30 days of admission and any mortality occurring was recorded.
RESULTS:
Totally 5122 patients were enrolled in the study, and injuries, NISS/ISS, and outcome as mortality were documented. The overall mortality was 525 (10.25%). RTA constituted 61.56% and mortality was two times higher than that in female. Patients arriving after 24 h had the highest mortality (16.22%) and time lag had a significant effect on outcome. Sensitivity and specificity of NISS/ISS in predicting mortality was 85.5%, 63% and 61.7%, 68.3%, respectively, and the sensitivity of NISS in predicting mortality is higher than ISS whereas the specificity of NISS is similar to ISS.
CONCLUSION:
The major cause of trauma in India is RTA and time lag has a significant effect on the prognosis of the patient, and NISS is a better scale and should be incorporated in management protocols and TRISS methodology.
Keywords
Injury Severity Score
New Injury Severity Score
road traffic accidents
trauma

Introduction
Injury is defined as damage to the body caused by an exchange with environmental energy that is beyond the body's resilience.[1] Trauma is the disease of young and the leading cause of death in thefirst four decades of life.[2] Scenario of trauma consists of various causes such as road traffic accidents (RTAs), railway accidents, drowning, assault, and others, out of which RTA outnumbers all other causes.[3] India has the fourth highest rate of road accident[4] in the world with a reported mortality rate of severely injured patients ranging from 7% to 45%.[5] As per the data issued by the Ministry of Road Transport and Highways 2013, India, mortality due to RTA was 11.6 per lac population as compared to 10.3 in Europe and 16.1 in the United States. Even the mortality rate/10,000 vehicles in India is as high as 10.5 compared to <2 in developed countries.[6] In a study from central India, it was observed that RTA was the most common cause of trauma (46.85%) and the most commonly affected age group was 11–40 years (64.06%)[7] with predominance of males (79.4%), in developing countries such as India, the resources for management of trauma patients in a government setup are constrained, and hence, the need of the hour is to have a simple yet reliable and authentic system for categorization of trauma patients, warranting optimal utilization of available resources. As a basic principle, more severe injuries should be given more importance when compared with less severe ones.
The Injury Severity Score (ISS) is defined as the sum of the squares of the single highest Abbreviated Injury Scale (AIS) score in each of the three most severely injured body regions.[8] Six regions are head, face, chest, abdomen, extremities including the pelvis, and external structures. However, due to an inherent flaw, ISS misses out more severe injury in a particular region while taking into account the second or third body region injuries having less significant injuries.[9] This drawback in the ISS resulted in the formulation of New Injury Severity Score (NISS) which rectifies the above problem.
The NISS is defined as the sum of the squares of the AIS of each of the patient's three most severe injuries; various studies have been conducted in the past to establish the superiority of NISS over ISS in terms of prediction of mortality with inconsistent results;[9-14] therefore, we have conducted this study to assess the cause of trauma with its epidemiological correlates and to categorize patients of trauma using NISS and ISS with their comparison in terms of mortality prediction in the present scenario of trauma in India.
Materials and Methods
The study was carried out on the trauma cases attending the emergency department equipped with Level II trauma care facilities of Medical College Hospital from North India between October 2015 and March 2017, and this research has been approved by the Institutional Review Board of the authors' affiliated institutions.
Study design
It was a prospective longitudinal study.
Statistical analysis
Data were compiled and analyzed using SPSS version 22.(IBM Corporation, New York U.S). Categorical data were analyzed using percentages. Sensitivity, specificity, positive predictive value, and negative predictive value were calculated to compare NISS with ISS as a predictor of mortality in trauma patients.
Inclusion criteria
Patients of trauma admitted to the emergency department were included in our study
All the posttraumatic deaths occurring within 30 days[3] of admission to the hospital.
Exclusion criteria
Age <10 years
Pathological fractures, minor cuts or laceration, superficial injuries, and closed small bone fractures
Patients presenting late (>1 week) due to the complication of initial trauma
Patients absconding within the initial hours (<6 h) of treatment from the hospital
Patients of burns and inhalational injuries as the injury pattern and cause of mortality are different from other trauma groups
Patients brought dead.
On admission to the emergency department, all resuscitative measures were followed according to the Advanced Trauma Life Support (ATLS) guidelines. Data of the patients were recorded as per the working pro forma by the on-duty junior resident final year who were pursuing MS Orthopedics and MS Surgery, which was counterchecked by with an emphasis to record the time of injury, type of injury, time lag between injury and arrival, detailed description of injury, treatment given, ISS and NISS on-duty senior resident (casualty); ultimate outcome (mortality occurring within 30 days) was documented on the working pro forma at the time of arrival/admission and stay at the hospital. At the time of discharge or death, it was further counterchecked by one of the co-authors of this study. We divided the patients in the score group, as per the triage pattern for the trauma patients with score 0–8 mild, 9–15 moderate, 16–25 severe, 26–49 very severe and ≥ 50 lethal and score of 16 or more was considered polytrauma. The patients who were discharged or referred to a higher center for further management were also followed up to 30 days of admission and any mortality occurring was also recorded.
Results
A total number of patients admitted in the hospital during the study period were 64,035, out of which 5122 patients (8.0%) admitted in trauma center were managed and assessed in our study. Out of which 4175 trauma patients were male and 947 were female. Thus, the percentage of males among trauma patients was 81.5%, which implies that the incidence of trauma is 4.4 times more in males as compared to that of females, suggesting that males are more exposed to various causative agents of trauma in the Indian scenario also. The overall mortality was 525 (10.25%), out of which 370 (8.86%) was in male trauma patients and 155 (16.37%) was in female trauma patients. The most common cause of death was multiple injuries in both sexes [Table 1]. In our study, extremities and pelvis were the most frequently injured body parts (34%), followed by head trauma (23.23%) [Table 1].

A major fraction, i.e., 2755 trauma victims out of 5122, arrived within 6 h. Two hundred and fifty of these 2755 patients (9.07%) expired despite best efforts, which is less than the overall mortality of 10.25%, whereas the patients arriving late (>24 h) had significantly higher mortality, i.e., 16.09% [Figure 1] and most common causes of trauma were RTAs followed by fall from height (FFH) [Figure 2]. The major victims fell in the productive age group between 20 and 55 years (3673/5122, 71.7%), while in the elderly age group, it was 680/5122 (13.3%), and in pediatric age group, it was 769/522 (15%). Table 2 and Figure 3 elaborate the comparative analysis of ISS and NISS favoring the NISS.
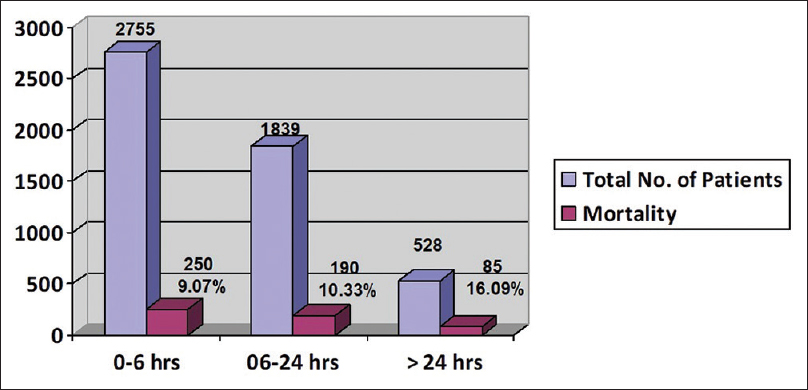
- Time lag between injury and arrival at hospital and its relation with mortality
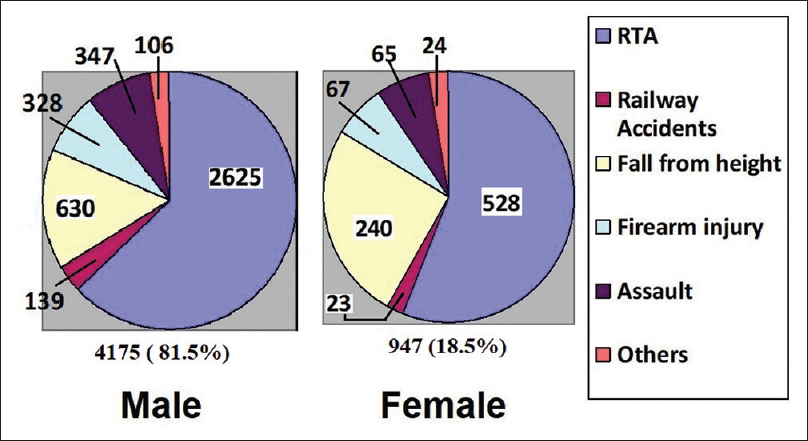
- Causative agent of injury among male and female patients

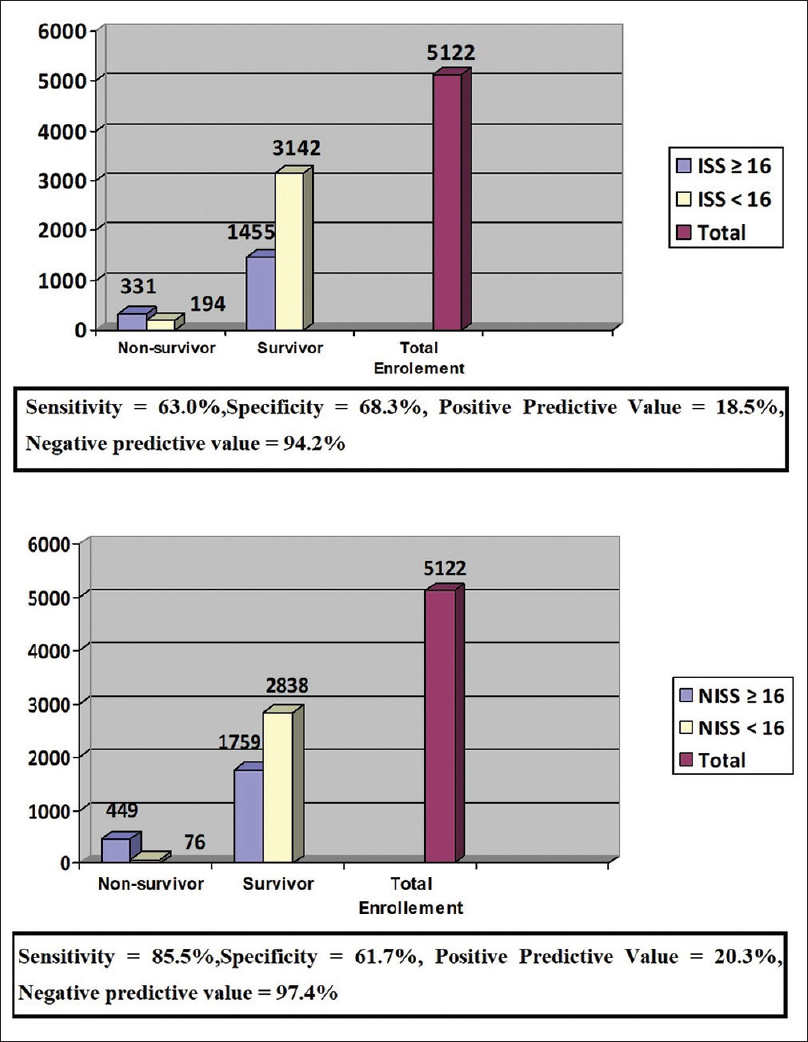
- Sensitivity and specificity of Injury Severity Score and New Injury Severity Score as the predictor of mortality
Discussion
With an initiative from the Government of India, development of national highways and expressways transportation has become swift, but there has been a surge in high-velocity polytrauma, even the district roads are overburdened due to the increase in population and vehicles which has led to an increase in the number of RTA victims and this is expected to be 5.46 lacs death by the year 2020.[15] Hence, these events have led to the establishment of integrated trauma management system in India. Trauma centers have been established in every district, and protocol-based approach for the management of trauma victims is being laid down. Adequate categorization of trauma patients is thus required for the prompt management of victims. In our study, we have used NISS and ISS scoring system for this purpose, and all trauma patients were managed as per the ATLS guidelines and standard resources available in the hospital. Our study had 81.5% males. Male preponderance has been reported in various studies between 71.5% and 85.5%, which is comparable to our study.[16] This male dominance is because they are more exposed to outdoor activities, that too of the productive age group (15–50 years). Total mortality in male trauma patients was 8.86% as compared to 16.37% in female trauma patients.
Time lag was an important aspect of our study. Patients coming within 6 h of injury had 9.07% mortality which was significantly lower than patients arriving after 24 h of injury (16.22%) [Figure 1]. The causative agents of hospital trauma admission were RTAs (61.56%), FFH (16.98%), firearm injuries (7.72%), other violence (8.03%), railway accident (3.16%), and other causes (2.53%) [Figure 2], as compared with the reports of Yangon General Hospital, Myanmar (WHO 2013),[17] which accounted for RTAs 53.6%, FFH 15.6%, violence 12.3%, and others (7.3%) in the total trauma admission of the hospital. As per national injury surveillance, Thailand, 2005–2010, RTA (47.31%), FFH (16.51%), violence (9.54%), and self-harm (4.03%) were the major causes of admission.[18] Available data from the Southeast Asia region (SEAR) show that RTA (18%), self-inflicted injuries (15%), and fires (burns, 11%), FFH (7%), violence (7%), and drowning (6%) are the major cause of hospital admission.[19] While data from the United States show that RTA (5.0%), poisoning (61.6%), and FFH (14.3%) were the major causes of hospital admission.[20] A study from North India by Rastogi et al. in 2014[21] stated that the major cause of injury was motorcycle accidents and FFH (61%), followed by pedestrian and bicycle accidents (17.8%), others and firearm injuries constituted 4.7%. All these suggest that in the Indian scenario as well as in SEAR, major cause of morbidity and mortality is RTA probably owing to poor traffic conditions, trauma health-care infrastructure, and inadequate implementation of traffic rules, enforcement of safety norms due to huge population, etc.
While comparing NISS and ISS, Table 2, in 0–8 score group of NISS, mortality was 2.2%, while in the same ISS group, mortality was 5.04%. In NISS group 9–15, patients had mortality of 2.90%, significantly lower when compared to those detected in the similar ISS group (6.59%), suggesting that at lower scores, NISS had a statistically greater negative predictive value for mortality (P< 0.05) as compared to ISS. In NISS group 25–50, mortality was 29.73% significantly higher than detected by ISS, i.e., 25.45%. This means at higher scores the NISS had more positive predictive value for mortality when compared to ISS. None of the patients survived in the ISS or NISS score group of more than 50, whereas in the 16–25 score group statistically significant difference was not recorded (P > 0.05). The sensitivity of NISS in predicting mortality was 85.5%, which is very much higher than that of ISS which was 63% while the specificity of NISS was 61.7%, which is almost similar to that of ISS which was 68.3%. Thus, this study shows that NISS is a better scale of predicting mortality than ISS [Figure 3]. Singh et al. in their study also concluded that the Revised Trauma Score (RTS) and Trauma and ISS (TRISS) were superior in predicting mortality in comparison to ISS.[4]
With the basic difference that on contrary to ISS which considers one most sever injury per body region from three most severely injured body regions, NISS considers up to three most severe injuries in a particular body region irrespective of other injuries in the body[9] NISS thus behaves in a way that is more consistent with a trauma surgeon's instincts than does the ISS, as injuries increases in number, chances of mortality increases, but if these injuries are accumulating in a single body region, mortality becomes inevitable thus enforcing implementation of NISS in trauma management protocol, and as the integral components of TRISS methodology are RTS and ISS, the use of NISS in its calculation may be more beneficial for assessing trauma victims.
Conclusion
The major cause of trauma in India is RTA and time lag has a significant effect on the ultimate prognosis of the patient which warrants a good prehospital and inhospital care. Mortality rate increases as the time lag between injury and arrival to hospital increases. NISS is a better mortality predictor as an anatomical scoring in traumatized patients when compared to ISS. The sensitivity of NISS in predicting mortality is very much higher than that of ISS while the specificity of NISS is almost similar to that of ISS. Therefore, this study shows that NISS is a better scale of predicting mortality than ISS in the Indian scenario also, and we also recommend using NISS instead of ISS as one of the components in TRISS methodology for assessing trauma victims.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Advances in the epidemiology of injuries as a basis for public policy. Public Health Rep. 1980;95:411-21.
- [Google Scholar]
- Trauma: The unrecognized epidemic. Anesthesiol Clin North Am. 1996;14:1-2.
- [CrossRef] [Google Scholar]
- Accidents and injuries. In: Parks Textbook of Preventive and Social Medicine (23rd). Jabalpur: M/s Banarsidas Bhanot Publishers; 2015. p. :405.
- [Google Scholar]
- Evaluation of trauma and prediction of outcome using TRISS method. J Emerg Trauma Shock. 2011;4:446-9.
- [CrossRef] [PubMed] [Google Scholar]
- The differential survival of trauma patients. J Trauma. 1987;27:602-6.
- [CrossRef] [PubMed] [Google Scholar]
- Capacity Building for Developing Trauma Care Facilities on National Highways Operational Guidelines. Government of India Ministry of Health and Family Welfare; 2013. Available from: http://www.dghs.gov.in/WriteReadData/userfiles/file/Operational_Guidelines_Trauma.pdf (accessed )
- [Google Scholar]
- Pattern of trauma in central India: An epidemiological study with special reference to mode of injury. Internet J Epidemiol. 2009;9:4726..
- [CrossRef] [Google Scholar]
- The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974;14:187-96.
- [CrossRef] [Google Scholar]
- A modification of the injury severity score that both improves accuracy and simplifies scoring. J Trauma. 1997;43:922-5.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the new injury severity score and the injury severity score in multiple trauma patients. Chin J Traumatol. 2008;11:368-71.
- [CrossRef] [PubMed] [Google Scholar]
- NISS predicts postinjury multiple organ failure better than the ISS. J Trauma. 2000;48:624-7.
- [CrossRef] [PubMed] [Google Scholar]
- The difference between ISS and NISS in a series of trauma patients in Brazil. Annu Proc Assoc Adv Automot Med. 2003;47:301-9.
- [Google Scholar]
- Predictors of mortality in adult trauma patients: The physiologic trauma score is equivalent to the trauma and injury severity score. J Am Coll Surg. 2002;194:695-704.
- [CrossRef] [PubMed] [Google Scholar]
- Prediction of mortality in pediatric trauma patients: New injury severity score outperforms injury severity score in the severely injured. J Trauma. 2003;55:1083-7.
- [CrossRef] [PubMed] [Google Scholar]
- 2016. National Injury Surveillance. Trauma Registry and Capacity Building Centre Dr. RML Hospital, New Delhi. Available from: http://www.nisc.gov.in/PDF/March%202016%20report.pdf (accessed )
- Epidemiological and trauma injury and severity score (TRISS) analysis of trauma patients at a tertiary care centre in India. Natl Med J India. 2004;17:186-9.
- [Google Scholar]
- Injury Surveillance Report 2010-2013 by Injury Prevention Project Department of Health Ministry of Health Myanmar. Available from: http://www.searo.who.int/entity/disabilities_injury_rehabilitation/country_experiences/isreport2010-2013mmr.pdf?ua=1 (accessed )
- [Google Scholar]
- Thailand's Report Situation of Severe Injuries Year 2005-2010. 2012. Data from Injury Surveillance (is), Thailand. Available from: http://www.searo.who.int/entity/disabilities_injury_rehabilitation/country_experiences/Thailandsituationseverinju2005-10.pdf?ua=1 (accessed )
- [Google Scholar]
- 2011. Strategic Approaches for Injury Prevention and Control in the South-East Asia Region World Health Organization. Available from: http://www.apps.searo.who.int/PDS_DOCS/B4668.pdf (accessed )
- National Ambulatory Medical Care Survey: 2015 State and National Summary Tables, U.S. Department of Health and Human Services. Available from: https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2015_namcs_web_tables.pdf (accessed )
- Epidemiology of patients admitted to a major trauma centre in Northern India. Chin J Traumatol. 2014;17:103-7.
- [Google Scholar]




