
Translate this page into:
Unexpected postoperative cerebrospinal fluid leaks without intraoperative dural tears after posterior lumbar interbody fusion

*Corresponding author: Yosuke Kawasaki, Department of Orthopedic Surgery, Mitsui Memorial Hospital, 1 Kanda-izumi-cho, Chiyoda-ku, Tokyo 101-8643, Japan kawasakiyorth@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kawasaki Y, Seichi A, Sasaki K, Kuzuhara S, Toriyama Y. Unexpected postoperative cerebrospinal fluid leaks without intraoperative dural tears after posterior lumbar interbody fusion. J Orthop Spine 2023;11:43-48. doi: 10.25259/Joasp_23_23.
Abstract
Objectives
Postoperative cerebrospinal fluid (CSF) leaks ussually occur after intraoperative dural tears. Sometimes, however, CSF leaks are found postoperatively even in the absence of intraoperative dural tears. The frequency and course of postoperative CSF leaks without intraoperative dural tears after posterior lumbar interbody fusion (PLIF) were investigated.
Material and Methods
The subjects were 200 patients (112 males, 88 females, age 69 ± 10 years) who underwent PLIF at our hospital from July 2014 to March 2020. The causative diseases were lumbar spinal stenosis in 167 cases, spondylolisthesis in 11 cases, lumbar disc herniation in 16 cases, and degenerative scoliosis in six cases. Of all the 200 cases, 27 were revision cases. If a dural tear occurred during the operation, dural repair was performed intraoperatively. Drain suction with negative pressure was discontinued when postoperative CSF leaks were found.
Results
Of the 180 patients without intraoperative dural tears, postoperative CSF leaks were observed in 27 patients (15.0%). Of these 27 patients, three symptomatic patients required reoperation. Residual CSF accumulations one year after surgery were observed in 14 patients, of whom six patients had severe CSF accumulations with a dural sac deformity, all of whom were asymptomatic. Of the 20 patients with intraoperative dural tears, 16 patients (80.0%) had postoperative CSF leaks, but none needed reoperation.
Conclusion
The frequency of postoperative CSF leaks without intraoperative dural tears was 15.0% in the present study. They require strict follow-up because they can cause severe postoperative CSF accumulations and may require reoperation.
Keywords
Cerebrospinal fluid (CSF)
Dural tear
Late presentation of dural tear (LPDT)
Lumbar spinal stenosis
Posterior lumbar interbody fusion (PLIF)
Postoperative CSF leaks
Pseudomeningocele
Spine surgery

INTRODUCTION
Postoperative cerebrospinal fluid (CSF) leaks usually occur when the dura mater is injured intraoperatively, but they sometimes occur in the absence of obvious intraoperative dural tears. When dural tears are repaired intraoperatively, they are generally not associated with long-term adverse clinical outcomes.1,2 On the other hand, if postoperative CSF leaks occur without intraoperative dural tears, it is not possible to assess and repair the dura mater directly, and continuous CSF leaks can occur, which may require reoperation. In addition, continuous CSF leaks can be associated with significant complications, including spinocutaneous fistulas (persistent leak through the incision), symptomatic pseudomeningocele, transdural cauda equina incarceration, intracranial haemorrhage, neurological deficits, hematoma, meningitis, brain abscess, and intracranial hypotension.3,4 Although there are many reports of postoperative CSF leaks, few reports turn their attention especially towards postoperative CSF leaks without intraoperative dural tears. Since postoperative CSF leaks are more likely to occur with highly invasive spinal surgery, we focused on the patients who underwent posterior lumbar interbody fusion (PLIF) and investigated the frequency and course of postoperative CSF leaks without intraoperative dural tears in these patients.
MATERIAL AND METHODS
This was a retrospective, cohort study. Informed consent was obtained from all participants in this study, and all procedures were approved by the institutional review board of our hospital. The participants were 200 patients (112 males, 88 females, age 69 ± 10 years) who underwent PLIF at our hospital from July 2014 to March 2020. There were 167 cases of lumbar spinal canal stenosis, 11 cases of spondylolysis, 16 cases of intervertebral disc hernia, and six cases of degenerative scoliosis. Of all the 200 cases, 27 were revision cases, 17 were on haemodialysis, and 6 were with rheumatoid arthritis. When performing PLIF, microsurgery was used to perform laminectomy and facetectomy. Pedicle screws (CD HORIZON® SOLERA® Spinal System, Medtronic, Minneapolis, MN, USA) were inserted using a navigation system (StealthStation® S7™ System, Medtronic), and interbody cages (CAPSTONE® PEEK Spinal System, Medtronic) were inserted with autograft bone. The presence or absence of intraoperative dural tears was confirmed in detail using an operating microscope (M525 F50 surgical microscope, Leica Microsystems Co. Ltd., Heerbrugg, Switzerland) in all cases. If the dura was torn during the operation, dural repair was performed under microscopy. After the dura was closed, we used the Valsalva manoeuvre strictly to ensure watertight closure. At the end of the surgery, two 10-Fr drains (BLAKE® Drains and JVAC™ Reservoirs, Ethicon, Cincinnati, OH, USA) were placed in the extradural space on suction. Drain suction with negative pressure was discontinued when the postoperative CSF leak was found. Drain removal depended on the amount of drain output (<100 ml/day).
Clinical evaluation
The presence or absence of intraoperative dural tears, the frequency of CSF leaks found after surgery, and the presence or absence of residual CSF accumulations on magnetic resonance imaging (MRI) one year after surgery were investigated. The details of cases where reoperation was required are also reported.
The diagnosis of postoperative CSF leaks was made clinically when a large amount (>300 ml/day) of clear colourless or red transparent fluid appeared continuously in the drainage bag after surgery. Beta-2-transferrin5 was not used in this study.
Evaluation of postoperative CSF accumulations
The authors created a CSF accumulation grading system [Figure 1]. The presence or absence of CSF accumulations on the dorsal side of the dural sac was examined by MRI one year after surgery and classified using this grading system. In this system, cases without CSF accumulations were defined as “CSF accumulation (−)”. Cases with CSF accumulations were defined as “CSF accumulation (+)”, and cases with severe CSF accumulations with a dural sac deformity were defined as “Dural sac deformity (+)”. The grading was performed blindly and independently by two board-certified spine surgeons (Yosuke Kawasaki and Atsushi Seichi). Each of the two surgeons has more than 20 years of clinical experience and is familiar with the interpretation of MRI images.
RESULTS
The operation time was 263 ± 43 minutes, the amount of intraoperative bleeding was 152 ± 74 ml, and the number of spinal fusion levels was 1−3. Of the 180 patients without intraoperative dural tears, postoperative CSF leaks were observed in 27 patients (15.0%) [Figure 2]. Of these 27 patients, three symptomatic patients required reoperation of the incarcerated cauda equina, and dural closure was performed. Residual CSF accumulations were observed in 14 patients, of whom six patients had severe CSF accumulations with a dural sac deformity, all of whom were asymptomatic. Of the 20 patients with intraoperative dural tears, 16 patients (80.0%) had postoperative CSF leaks, but none needed reoperation. Although postoperative MRI showed residual CSF accumulations in seven patients, there was no severe CSF accumulation with a dural sac deformity. Seven of the 20 with intraoperative dural tears were revision cases, and 20 of the 180 without intraoperative dural teas were revision cases.
Details of the cases that required reoperation are shown below.
[Case 1] A 73-year-old woman underwent PLIF at the L4/5 level for bilateral sciatica and intermittent claudication. Severe canal stenosis at the L4/5 level was decompressed without an intraoperative dural tear. From the day after the operation, headache, nausea and vomiting were observed, and the drainage was serous and over 300 ml/day. Therefore, it was judged that postoperative CSF leaks had occurred, and drain suction with negative pressure was discontinued. The drain tube was removed 72 hours after the operation, and the wound at the drain insertion was stapled. The surgical wound healed uneventfully, and she was discharged from the hospital walking. Five weeks after surgery, fluctuating swelling was noticed over the lumbar spine operative site. MRI showed a 7 × 3 × 3 cm3 lobulated CSF intensity collection on the dorsal side of the dural sac overlying the laminotomy defect. The collection was extended craniocaudally from L4 to L5 and anteroposteriorly from the subcutaneous plane to the dorsal aspect of the dural sac [Figure 3a], and surgical exploration was performed. On the dorsal side of the dural sac, there was a cavity filled with CSF, the wall was unusually thick, wide open, and the cauda equina protruded from a 10-mm, oval-shaped hole in the dural sac. The patient was diagnosed as a case of lumbar pseudomeningocele with transdural cauda equina incarceration, and the pseudomeningocele sac was extirpated. The cauda equina was returned to the dural sac, and the dural defect was then closed with a fascial patch [Figure 3b]. The patient’s postoperative course was uneventful. Three months postoperatively, the patient reported full relief of neurogenic claudication and considerable improvement of bilateral sciatica. One year later, MRI showed complete resolution of the pseudomeningocele, and bony fusion at the L4/5 level was confirmed on dynamic X-rays and Computed Tomography (CT).
[Case 2] An 80-year-old woman underwent PLIF at the L4/5 level for bilateral buttock pain and intermittent claudication. Severe canal stenosis at the L4/5 level was decompressed without an intraoperative dural tear. Serous drainage continued for 300 ml/day or more the day after the operation. It was judged that postoperative CSF leaks had occurred and drain suction with negative pressure was discontinued. The drain was removed 72 hours after the operation, and the wound at the drain insertion was stapled. The wound healed uneventfully, and she was discharged from the hospital walking. Three months after surgery, she could not sit because of bilateral buttock pain in the sitting position. MRI showed a 5 × 3 × 2 cm3, CSF-intensity collection on the dorsal side of the dural sac at L4/5 [Figure 4a], and surgical exploration was performed. On the dorsal side of the dural sac, there was a cavity filled with CSF, the wall was unusually thick and wide open, and the protruding cauda equina adhered to a 20-mm connecting hole in the dural sac. The patient was diagnosed as having a lumbar pseudomeningocele with transdural cauda equina incarceration, and the pseudomeningocele sac was extirpated. The protruding cauda equina was peeled off and returned to the dural sac, and the dural defect was then closed with a fascial patch [Figure 4b]. The patient’s postoperative course was uneventful. Three months postoperatively, the patient reported full relief of the buttock pain. One year later, the MRI examination showed complete resolution of the pseudomeningocele, and the bony fusion at the L4/5 level was confirmed on dynamic X-rays and CT.
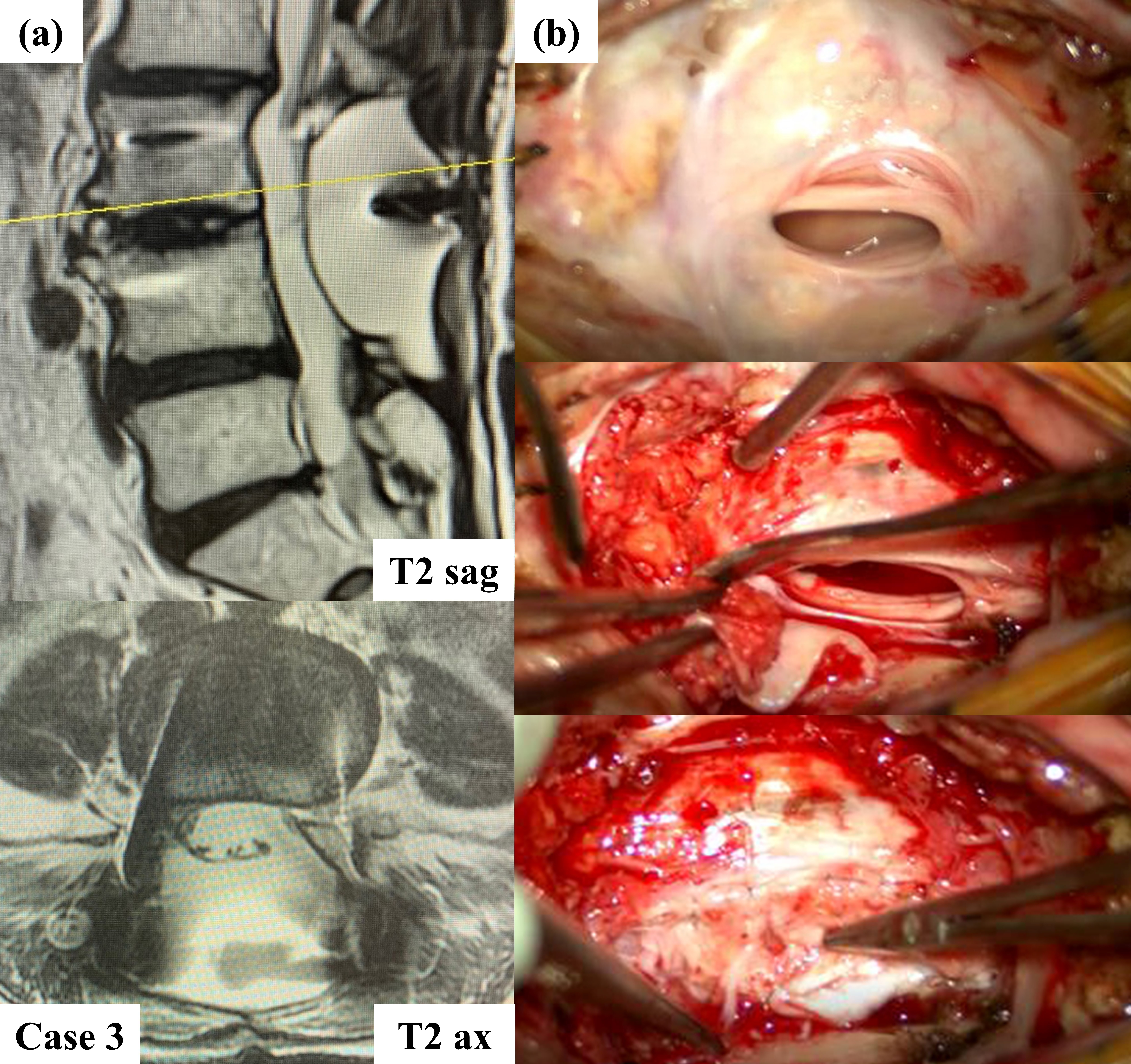
[Case 3] An 84-year-old woman underwent PLIF at the L4/5 level for bilateral buttock pain and intermittent claudication. She had a history of lacunar cerebral infarction. Severe canal stenosis at the L4/5 level was decompressed without an intraoperative dural tear. After the surgery, the drain volume was over 300 ml/day, and headache and nausea occurred when her head was raised. Therefore, it was judged that postoperative CSF leaks had occurred, and drain suction with negative pressure was discontinued. The drain tube was removed four days after surgery, and the patient began walking the next day. Aphasia was observed on the 7th postoperative day, and haemorrhagic cerebral infarction and subarachnoid haemorrhage were observed on head CT and head MRI. Neurological treatment (rest, fluid replacement, edaravone administration, blood pressure control, and clopidogrel administration) improved the symptoms. Her consciousness became clear, and motor function and sensory function recovered. She was able to walk more than 2000 steps after leaving the hospital. Four months after surgery, nausea appeared while brushing her teeth, and vomiting and bilateral sciatica then occurred. MRI showed a 5 × 3 × 4 cm3, CSF cystic collection on the dorsal side of the dural sac at L4/5 [Figure 5a]. Bilateral sciatica did not improve even after eight months, and surgical exploration was performed. On the dorsal side of the dural sac, there was a cavity filled with CSF, the wall was unusually thick and wide open, and the cauda equina adhered to a 15-mm connecting hole in the dural sac. The patient was diagnosed as having a lumbar pseudomeningocele with transdural cauda equina incarceration, and the pseudomeningocele sac was extirpated. The cauda equina was peeled off and returned to the dural sac, and the dural defect was then closed with a fascial patch [Figure 5b]. The patient’s postoperative course was uneventful. Three months after surgery, the patient’s bilateral sciatica improved significantly, and she could walk well. One year later, MRI showed complete resolution of the pseudomeningocele, and the fusion at the L4/5 level was confirmed on dynamic X-rays and CT.
DISCUSSION
Even if the dura was torn during the operation, severe postoperative CSF accumulations rarely occurred, and reoperation was not needed, although the frequency of postoperative CSF leaks was high even after dural repair. This was probably due to the well-functioning intraoperative dural repair. On the other hand, when there was no intraoperative dural tear, the frequency of postoperative CSF leaks was low. However, when CSF leaks occurred after surgery, severe postoperative CSF accumulations with a dural sac deformity were more likely to occur. In addition, reoperations were required in some cases. Since the extent of dural damage was impossible to assess directly, strict follow-up was considered necessary in cases with postoperative CSF leaks without intraoperative dural tears.
In the present study, the follow-up rate was 85.0% one year after the operation. The cases that could not be followed up included death in one case, reoperations in three cases, spinal surgery at other levels in nine cases, and MRI was not performed one year after surgery in 14 cases. Three cases were lost to follow-up. Possible causes of postoperative CSF leaks without intraoperative dural tears include intraoperative dural tears that were not noticed during surgery, postoperative dural tears due to increased CSF pressure associated with postoperative postural changes, and postoperative dural tears due to the negative pressure by the suction drain or misplaced drainage tubes. Although the definite cause is inconclusive, in our view, the adverse effect of the negative pressure by the suction drain for thinned dura mater after long-term spinal stenosis may be a strong factor. We are going to perform a controlled study by dividing patients into two groups with or without negative pressure by a suction drain.
Although there may be criticism such as “It seems to be a high rate of un-detected intraoperative dural tears and high rate of failure of primary dural repairs because the incidence of CSF leaks in this study is high.”, the presence or absence of intraoperative dural tears was confirmed in detail using an operating microscope in all cases during surgery, and the Valsalva manoeuvre was used strictly to confirm watertight closure when dural repair was performed.
It has been reported that the probability of developing symptomatic and non-symptomatic pseudomeningoceles after lumbar laminectomy is 0.068% to 2%.6 In the present study, symptomatic pseudomeningoceles occurred in three of 200 cases (1.5%). The relatively high percentage may be due to only targeting the cases with high invasion, such as spinal fusion.
Symptomatic giant pseudomeningoceles are reported to be more likely to occur in the lumbar region because the lumbar spinal fluid is under higher hydrostatic pressure than the upright cervical spine, and more surgical procedures are performed on the lumbar spine.6 Postoperative CSF leaks without intraoperative dural tears may also be more likely to occur in the lumbar region, because the lumbar spine is under higher hydrostatic pressure than the cervical spine.
Postoperative CSF leaks may be easily missed especially if drain use was discontinued according to a predetermined time (typically by 12–48 hours postoperatively) because it is difficult to monitor changes in drain output adequately.
All three cases that required reoperation had both late presentation of dural tear (LPDT)2,7,8 and postoperative CSF leaks without intraoperative dural tears. These facts suggest that patients with postoperative CSF leaks without intraoperative dural tears are more likely to develop LPDT compared with patients with intraoperative dural repair. According to the present study, non-symptomatic postoperative CSF accumulation with a dural sac deformity does not seem to require additional invasive treatment.
CONCLUSION
The frequency of postoperative CSF leaks without intraoperative dural tears after PLIF was 15.0% in our study. They were likely to result in postoperative CSF accumulations with a dural sac deformity. In the three cases, a large dural/arachnoid defect accompanied by transdural cauda equina incarceration occurred, resulting in a symptomatic pseudomeningocele that required repair. Since the extent of dural damage was impossible to assess directly, strict follow-up was considered necessary in cases with postoperative CSF leaks without intraoperative dural tears.
Ethical approval
The research/study approved by the Institutional Review Board at Mitsui Memorial Hospital, number 2019C12, dated 1st March 2019.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Long-term results of lumbar spine surgery complicated by unintended incidental durotomy. Spine (Phila Pa 1976). 1989;14:443-6.
- [CrossRef] [PubMed] [Google Scholar]
- Late-presenting dural tear: incidence, risk factors, and associated complications. Spine J. 2018;18:2043-50.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of cerebrospinal fluid leak after spine surgery. Chin J Traumatol. 2017;20:81-3.
- [CrossRef] [PubMed] [Google Scholar]
- Multiplicity of cerebrospinal fluid functions: New challenges in health and disease. Cerebrospinal Fluid Res. 2008;5:10.
- [CrossRef] [Google Scholar]
- Management of giant pseudomeningoceles after spinal surgery. BMC Musculoskelet Disord. 2010;11:53.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence and treatment of delayed symptoms of CSF leak following lumbar spinal surgery. Eur Spine J. 2015;24:2069-76.
- [CrossRef] [PubMed] [Google Scholar]
- Conservative management for late presenting dural tears after spine surgery: An institutional experience and literature review. World Neurosurg. 2020;134:e82-92.8.
- [CrossRef] [PubMed] [Google Scholar]




