
Translate this page into:
A rare occurrence of enchondroma with pathological fracture of proximal femur in an adult female: A case report
*Corresponding author: Gujjala Venkata Naga Yeswanth, Department of Orthopaedics, Karnataka Institute of Medical Sciences, Hubli, Karnataka, India yeswanth.orthodr@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mulimani V, Bangarshettar A, Atluri VV, Yeswanth GVN. A rare occurrence of enchondroma with pathological fracture of proximal femur in an adult female: A case report. J Orthop Spine 2023;11:71-75. doi:10.25259/Joasp_13_23.
Abstract
Enchondroma occurrence in the proximal femur is a very uncommon condition. We report a 40-year-old female with a history of accidental slip and fall, sustained injury to her left lower limb, and was unable to bear weight on the injured leg since the fall. Anteroposterior radiograph of the pelvis with bilateral hips shows a well-defined lytic lesion in the neck of the femur with some calcified matrix and no periosteal reaction with the left femoral subtrochanteric fracture. Magnetic resonance imaging scan revealed hypointense signals on T1 and hyperintense signals on T2 sequence over the proximal femur as well as left subtrochanteric femur fracture. After preanesthetic evaluation, bone curettage with excision biopsy with open reduction and internal fixation with long proximal femoral nail and bolts and iliac crest bone graft was done. A biopsy sample sent for histopathological examination reveals enchondroma. Complete weight bearing was started after four months. No recurrence was noted on follow up.
Keywords
Benign bone tumours
Enchondroma
Lytic lesion

INTRODUCTION
Enchondroma is a benign hyaline cartilage lesion that most usually affects people between the ages of 20 and 40, however, it can affect people of any age with no sex differentiation. The most common type of enchondroma is the solitary enchondroma, which arise within the bone’s medullary cavity. In comparison to the proximal humerus, distal femur, and proximal tibia, the prevalence rate in the proximal femurs is 0.7%.1 Sometimes it can also manifest as Ollier’s disease, which is characterised by the appearance of many cartilaginous tumours. When multiple cartilaginous tumours are associated with haemangiomas over soft tissue it is called Maffucci syndrome.2 With this uncommon presentation, we aim to add to the corpus of knowledge for the orthopaedic society since there is little information in the medical literature on the treatment of enchondromas in the proximal femur. Our goal is to provide insightful information that can assist specialists effectively identifying akin cases of proximal femur enchondroma, planning successful interventions, improve patient outcomes.
CASE REPORT
A 40- year-old healthy female reported to our casualty with a history of trauma to her left lower limb. Since the fall, she has complained of pain, swelling, discomfort, and the inability to bear weight on the injured leg. The patient has had type 2 diabetes mellitus for two years and is on regular medication and no other complaints.
On examination, we noted diffuse swelling and tenderness over the left thigh region with restricted hip and knee range of movements. Bony crepitus and abnormal mobility could not be elicited due to pain. There is no lymphadenopathy and distal neurovascular deficits. The patient was stabilised hemodynamically and necessary radiographs were done. Routine blood tests, parathyroid hormone levels, erythrocyte sedimentation rate, and C reactive protein were within the normal range for the patient.
Anteroposterior radiograph of the pelvis with bilateral hips [Figure 1] shows a well-defined lytic lesion in the neck of the femur and proximal femur with some amount of calcified matrix and no periosteal reaction with the subtrochanteric fracture of the left femur. To rule out ovarian carcinoma, cancer antigen 125 levels were done and it was within normal limits.

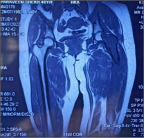
Magnetic resonance imaging (MRI) [Figures 2 and 3] showed hypointense signals on the T1 and hyperintense signals on the T2 sequence over the femoral head, neck, and proximal shaft of the femur, as well as left subtrochanteric femur fracture with the mild collection and surrounding muscle oedema.

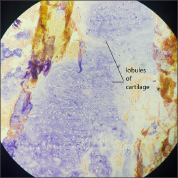
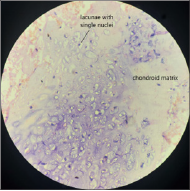
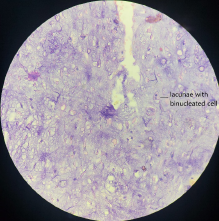
After careful clinical assessment and preanesthetic evaluation, the patient was taken for surgery. We did bone curettage with excision biopsy with open reduction and internal fixation with long proximal femoral nail and bolts and iliac crest bone graft. A biopsy sample was sent for histopathological examination revealed lobules of cartilage [Figure 4], chondrocytes with lacunae with single nuclei and chondroid matrix [Figure 5], and a few were binucleated cells [Figure 6] suggestive of “ENCHONDROMA”.
Immediate postoperatively patient was advised to bed rest. Static quadriceps and knee bending exercises were started on the third day. Non-weight bearing mobilisation began on the fifth day and discharged on the tenth day. After six weeks, partial weight-bearing mobilisation was begun. Complete weight-bearing mobilisation started after four months. On repeat x-rays at six months follow up, there were signs of union and no signs of recurrence [Figure 7] and the patient did not have pain but had little difficulty in sitting cross legged [Figure 8] and squatting.


DISCUSSION
After osteochondroma, enchondroma is the second most frequent benign tumours of the bone which typically affects the bone’s cartilage. These are usually asymptomatic and are often discovered by chance in an unrelated radiological examination or after a pathological fracture. Typically, patients complain of swelling which may or may not be painful.
When pathological fractures or cortical expansion in small bones are present, bone scans show increased uptake.3 The presence of pathology or lytic lesion in the femoral neck region arouses the possibility of various other diagnoses such as simple bone cyst, aneurysmal bone cyst, fibrous dysplasia, Chondroblastoma, giant cell tumour, chondrosarcoma, chondromyxoid fibroma, and osteoblastoma.4 As a result, enchondroma should be considered in such cases.
Simple bone cysts are primarily seen in children and consist of clear serosanguinous fluid surrounded by a lining membrane.4 In skeletally immature patients, an x-ray reveals a lucent lesion with sclerotic borders.
Aneurysmal bone cysts are benign osteoclastic giant cell-rich neoplasms with multiple blood-filled channels and cystic voids, seen under the age of 20 years. Radiographs demonstrate a sharply defined, expansile solitary lucent bone lesion, with thin-walled cavities.5 T2 sequence MRI reveals hyperintense signals.
Fibrous dysplasia is most common in children and young adults, and there is no gender preference. On radiographs, it shows a ground-glass matrix with no periosteal reaction, cystic or sclerotic lesions. MRI shows heterogeneous signals in both T1 and T2 sequencing.
In children, Chondroblastoma are benign neoplasms that develop in the long bone epiphysis or apophysis. On radiographs, it shows radiolucent, fluffy internal calcifications, endosteal scalloping, cortical thinning, and cortical erosion. Chondroblastoma is distinguished from other epiphyseal lesions by the presence of solid or layered periosteal reaction distant from the lesion (involving the diaphysis).6 T2 MRI sequence shows heterogeneous signalling.
Chondromyxoid fibromas are uncommon benign cartilaginous neoplasms, characterised by progressive pain, often long standing or osseous swelling, and limited range of motion in the affected limb. On plain radiography, it appears as a lobulated or oval eccentric lytic lesion with well-defined sclerotic borders.7 Osteoblastoma is rare and most commonly seen in the spinal column. It appears as an expansile lytic lesion with a rim of reactive sclerosis and internal calcification on radiographs. On the T2 sequence, MRI shows an iso or hypointense signal.4 Giant cell tumour is typically seen in long bones. On radiographs, it shows expansile, eccentric lytic lesions with well-defined sclerotic margins. On microscopy, it typically comprises osteoclastic large cells with a varying number of nuclei. MRI findings are non-specific with variable signals on T2 sequence.
Chondrosarcoma is a malignant cartilaginous tumour, usually appear in the fourth to fifth decade of life. It is characterised by pain and palpable mass over the long bones. On radiographs, it shows lytic lesions with popcorn calcifications. Cortical remodelling, thickening, and periosteal reaction can also help differentiate an enchondroma from a low-grade chondrosarcoma.8 In terms of treatment, asymptomatic cases can be treated with serial radiographs and regular checkups. Symptomatic patients have to be addressed surgically. Extended bone curettage of the lytic lesion followed by the use of chemical adjuvants with bone grafting or bone substitutes can be done. Prophylactic fixation is also an option if necessary. Fracture fixation is necessary in cases of pathological fractures.
Recent advances in the management of femoral neck enchondroma allow for arthroscopic curettage and fixation, which is a less invasive surgical procedure with a better outcome clinically.9 Limitations of our study are, shorter follow-up period, limited comparative data, and lack of control group.
CONCLUSION
This case of ours was an incidental finding of the enchondroma with a left femoral subtrochanteric fracture. The mainstay of diagnosis confirmation is by histopathology and radiology. Although it is very rare, enchondroma should be kept as a differential diagnosis. Early diagnosis and intervention can provide fair outcomes in cases of lytic lesions in the proximal femur.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patients consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Prevalence of enchondromas of the proximal femur in adults as an incidental finding on MRI of the pelvis. Indian J Radiol Imaging. 2021;31:582-85.
- [CrossRef] [PubMed] [Google Scholar]
- Enchondroma versus low-grade chondrosarcoma in appendicular skeleton: clinical and radiological criteria. J Oncol. 2012;2012
- [CrossRef] [PubMed] [Google Scholar]
- Maffucci’s syndrome: functional and neoplastic significance—case report and review of the literature. J Bone Joint Surg Am. 1973;55:1465-79.
- [PubMed] [Google Scholar]
- A rare occurrence of enchondroma in neck of femur in an adult female: a case report. J Clin Diagn Res. 2015;9
- [CrossRef] [PubMed] [Google Scholar]
- Bone cysts: unicameral and aneurysmal bone cyst. Orthopaed Traumatol Surg Res. 2015;101:S119-27.
- [CrossRef] [PubMed] [Google Scholar]
- The Frequency and Diagnostic Significance of Periostitis in Chondroblastoma. AJR Am J Roentgenol. 1990;154:309-14.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging features of chondromyxoid fibroma: report of 15 cases and literature review. Br J Radiol. 2016;89
- [CrossRef] [PubMed] [Google Scholar]
- Differentiation of enchondroma and low-grade chondrosarcoma-clinicopatological and radiological findings in 34 cases. Sarcoma. 2002;6:S9.
- [Google Scholar]
- Arthroscopic treatment for femoral neck enchondroma: case report. J Hip Preserv Surg. 2015;2:428-30.
- [CrossRef] [PubMed] [Google Scholar]




