
Translate this page into:
Clinical outcome of peroneus longus tendon autograft in primary anterior cruciate ligament reconstruction
*Corresponding author: Preetesh J. Shah, Department of Orthopaedics, Radiance Hospital, Ahmedabad, Gujarat, India drpreeteshs@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Shah PJ, Shah DP. Clinical outcome of peroneus longus tendon autograft in primary anterior cruciate ligament reconstruction. J Orthop Spine 2023;11:49-55. doi: 10.25259/Joasp_47_23
Abstract
Objectives
Peroneus longus tendon (PLT) is employed as a graft for the reconstruction of graft in orthopedic surgical procedures in consideration of its favourable biochemical properties. PLT autograft has demonstrated encouraging outcomes, but there is still a lack of information on its application. We implied measuring the stability of the knee and functional outcomes using PLT autograft. The aim of the study is to evaluate the clinical outcomes of PLT autograft in primary anterior cruciate ligament (ACL) reconstruction.
Material and Methods
A retrospective, multicenter study involved 104 patients undergoing primary reconstruction of ACL with PLT autograft from March 2020 to 2022. A single surgeon performed on each patient. Graft characteristics and harvesting period were recorded. At the preoperative, six-week, six-month, and 12-month postoperative timepoints, the Lysholm score and the International Knee Documentation Committee (IKDC) score were used to assess the stability and functional status of the knee. The functionality of the foot/ankle was recorded using the American Orthopedic Foot and Ankle Score (AOFAS) prior to injury and postsurgery. All the statistical analyses were performed using Statistical Package for Social Sciences (SPSS) version 20.
Results
PLT autograft was done in all the patients with a specific graft harvesting time of 8.16 (6–10 min), graft length 24.77 cm, and graft diameter 8.48 mm. The mean IKDC and Lysholm scores preoperatively were 51.80 ± 8.16 and 50.78 ± 4.87, and significantly (P < 0.0001) increased 95.09 ± 5.44 and 96.35 ± 3.94 at 12-month follow-up, suggesting PLT as an effective reconstructive procedure. The AOFAS score showed no difference preinjury and postsurgery. However, 3 (2.88%) patients experienced toe pain as a postprocedure complication.
Conclusion
PLT autograft had shown significantly higher functional and clinical outcomes inferring to be a viable option for patients and can set a benchmark for ACL reconstruction.
Keywords
Autograft
Graft harvesting
Knee stability
Peroneus longus tendon

INTRODUCTION
The anterior cruciate ligament (ACL) reconstruction post its rupture has been considered the most effective treatment standard for the restoration of stability in knees and joint functionality.1 It is one of the several ligaments in the knee, which is crucial for proper knee movement and stability and is particularly prone to injury during sports and physical activities. Females are two to eight times higher in risk than males to have an ACL tear which may result in long-term consequences such as osteoarthritis and decreased quality of life.2,3 The treatment of ACL injuries can be performed surgically by reconstructing the ligament with an allograft or an autograft, or conservatively by using a knee brace or physical therapy.4 Currently, ACL restoration is performed by orthopaedic surgeons employing the peroneus longus tendon (PLT) as a type of autograft in addition to the widely used bone-patellar tendon-bone or hamstring tendon grafts.5 However, because of the pain in the portion of the knee, extensor strength deficiencies, donor-site morbidity, and the progression of osteoarthritis, some doctors used hamstring autografts for ACL restoration. Autografts of the PLT are frequently employed in some orthopaedic surgeries, such as the restoration of the spring ligament.6 The surgeons consider the strength of the graft, its size, and ease of harvesting the graft with the least amount of donor-site morbidity.1 Moreover, PLT has been suggested as a suitable autograft for the replacement of the ligament, and there is less data available on the clinical effectiveness of PLT.7 In some earlier case studies, the PLT was used as the autograft of first preference for ACL restoration, with satisfactory clinical outcomes and lower morbidity at the donor site.6 The PLT autograft plays a significant role in the functionality of the foot and ankle. According to studies, the strength and safety of the anterior half of the PLT make it more appropriate for ligament repair.7 PLT is a potential graft in reconstructive orthopaedic procedures with respect to its efficient biomechanical properties. The main intent of the PLT is to improve first-ray plantar flexion and provide movement to the foot.5 PLT is a viable graft option for the reconstruction of knee ligament due to its better clinical outcomes, minimal morbidity at the ankle donor site, and comparable tensile strength.8 The parameters for the optimal autograft donor include acceptable strength, suitable size, ease of harvesting, and safety. PLT meets these criteria and has sufficient size and strength to serve as an alternative autograft for an ACL reconstruction.9 Patients with acute ACL rupture underwent ACL repair using the ipsilateral PLT as an autograft. PLT is a viable alternative for an autograft because of its good biomechanical characteristics, including lower failure loading and stiffness. In light of its durability, consistency of clinical results, and reduced donor-site morbidity, it is an effective option. In addition to the PLT’s superficial location, it is promptly readily exposed.10 In the present study, we emphasised the selection of PLT autograft for the surgical procedure of ACL rupture. The aim of this study was to demonstrate in vivo results that show the safety and efficacy of PLT autograft in primary ACL reconstruction.
MATERIAL AND METHODS
A total of 104 patients with ACL tear were enrolled with 12-month study duration follow-up retrospectively. The data of the patients who underwent the surgical operation from the time-point of March 2020–2022 were considered for the study. A single surgeon performed the ACL reconstruction with PLT autograft on enrolled patients highlighting the consistency and uniformity of surgical intervention. The study was conducted with the approval of Institutional Ethics Committee Aatman Hospital. The duration since the injury and the surgical procedure was recorded to evaluate the patient’s postoperative outcomes for assessing the success of the intervention. Preoperative demographic data of patients were also recorded. The functional outcomes of the patients were evaluated before the surgery and at the time-point of six weeks, six months, and 12 months after the surgery. The functional evaluation of the operated knee of the patients was performed by using International Knee Documentation Committee (IKDC) score and Lysholm scale. These scores involve various factors, including pain, swelling, range of motion, stability, and the ability of the patients to carry out their daily activities. The resulting scores were then utilised to monitor the patient’s progress to evaluate the effectiveness of their treatment and ensure that patients received the most appropriate care for their knee condition. The conditions at the site of the foot and ankle for PLT graft were assessed with American Orthopaedic Foot Ankle Society (AOFAS) score presurgery and postsurgery. AOFAS score is a set of questionnaires that evaluates the various parameters such as pain, function, alignment, and range of motion in patients.11–13
Surgical technique
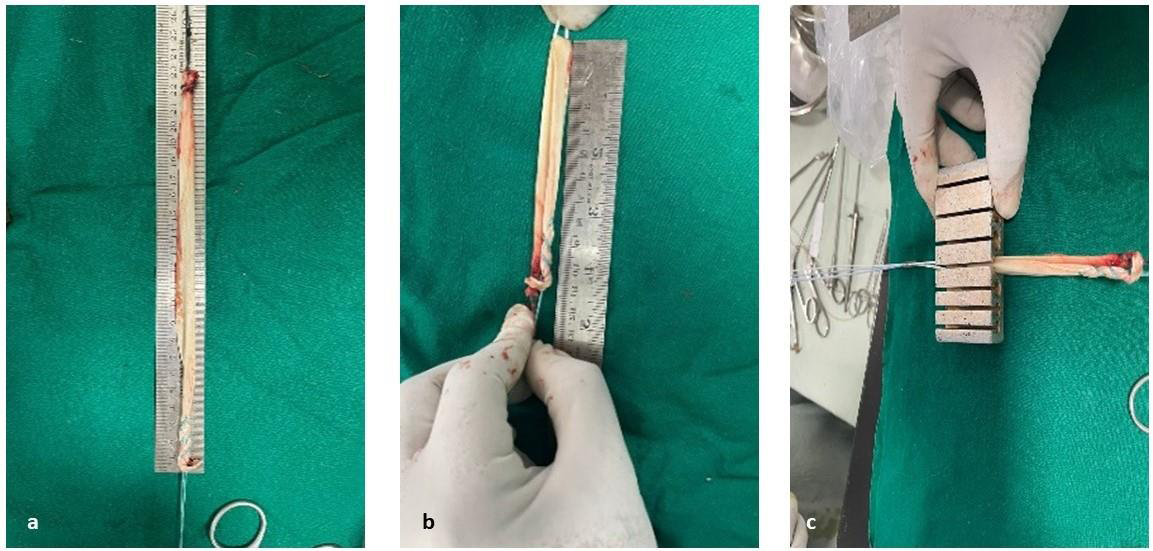
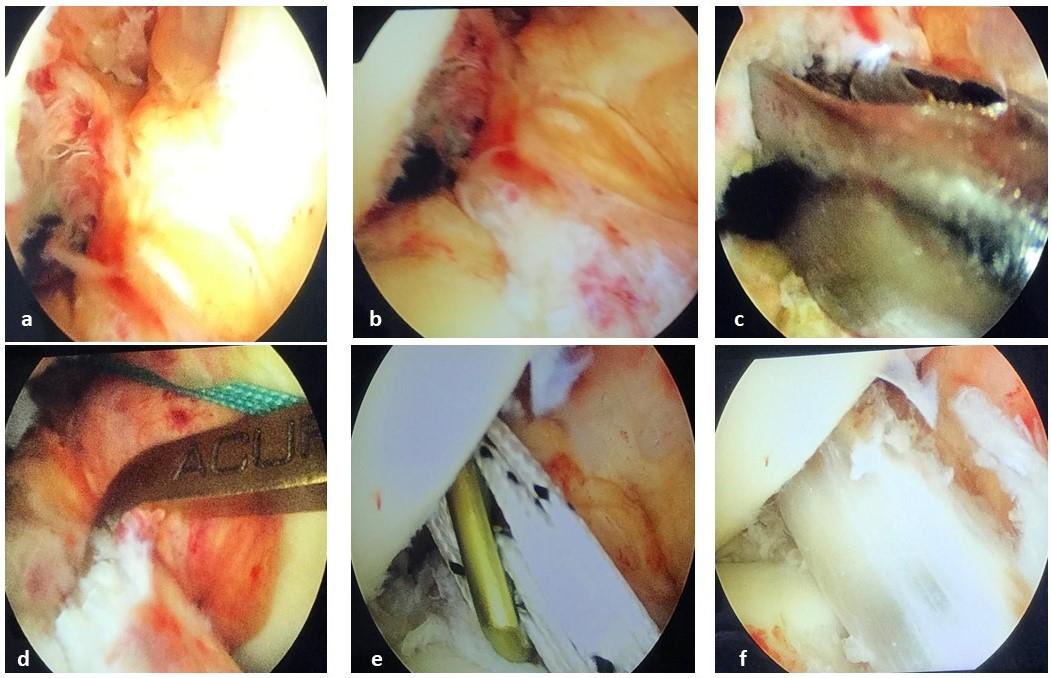
Under spinal anaesthesia, all patients under tourniquet control were operated by the orthopaedic surgeon. Average tourniquet time was 53 min (40–70 min). After diagnosing the knee joint through arthroscopy and confirming the tear, the decision for ACL reconstruction was taken. The PLT graft was harvested at the same side of the leg where the ACL injury occurred. The incision of 1 inch on the surface of the skin was made by putting a 2-cm incision over the proximal to lateral malleolus along the fibula’s posterior border [Figures 1a and 1b]. The PLT and peroneus Brevis tendon (PBT) were identified after incising the subcutaneous tissue and skin. The tendon sheath was incised, and the tendon was pulled out using a mixter. The tying of the distal ends of PLT and PBT was performed. The incised proximal end of PLT was tied by using a whipstitch [Figures 2a and 2b]. The graft was harvested by using the closed stripper of 7 mm size. The average length of graft was 24.77 cm and the site of the graft wound was closed in layers. The sheath was closed and post that the closure of subcutaneous tissue and skin was carried out [Figures 2c and 2d]. The diameter of the graft was checked after tying the other end of PLT with a whipstitch. The double stranded graft was 8.48 mm in size. At the femoral side of the fixation, the adjustable loop with Endobutton was used in all the subjected cases [Figures 3a–c]. The first transportal femoral entry using a beath pin 7 mm offset aimer was performed. Following this, a 4-mm endoreaming procedure was carried out to enlarge the hole created by the pin. The 20 mm length of the femoral tunnel was made with a graft diameter size reamer. The suture was then passed using the beath pin to railroad the graft [Figures 4a–c]. The tibial entry was done by using an Acufex jig at an angle of 45°. The tibial tunnel diameter was the same as that of the femur diameter. The suture from the femoral tunnel was pulled down and taken out through the tibial exit. The graft was pulled up using a railroad. The Endobutton was flipped on the lateral femoral cortex, and the graft was pulled in the femur using an adjustable loop [Figures 4d–f]. The tibial side graft fixation was done using a bioabsorbable screw (two times bigger than the graft size) after doing cyclical loading [Figure 5]. The graft fixation was checked at the end by doing arthroscopy and checking the graft tension. The intraoperative pivot shift test was performed in all cases.



Statistical analysis
The frequency distribution of each categorical component was summarised by categorial variables (relative frequencies and percentages). The statistical package for the social sciences, version 20, was used to carry out the analysis. For continuous variables, the mean ± standard deviation was provided, and for nominal variables, the findings were expressed as a number (%). The Wilcoxon test and paired t-test were employed for ordinal and continuous variables, respectively, to assess changes in pre-post differences. The Chi-square test or Fisher’s exact test was used to compare the frequency of other variables. At P < 0.05, the findings were statistically significant.
RESULTS
The average age of patients was 33.61 ± 11.77. The demographics, injury side, and mechanism were noted and represented in Table 1. The PLT autografting was performed in all the patients, and the grafts harvested were of different lengths and diameters.
| Parameters | n = 104 |
|---|---|
| Age (years), mean ± SD | 33.61 ± 11.77 |
| Gender, n (%) | |
| Male | 74 (71.15) |
| Female | 30 (28.84) |
| Side of injury, n (%) | |
| Right | 57 (54.80) |
| Left | 47 (45.20) |
| Nature of injury/mechanism of injury, n (%) | |
| Accident | 89 (85.58) |
| Sports injury | 15 (14.42) |
n: Number of patients, SD: Standard deviation
The characteristics of the graft are listed in Table 2. The fixation method of the arthroscopic reconstruction technique used was an upper adjustable loop and lower bioscrews in all the participants. The postoperative pivotal shift test was performed on patients to assess knee laxity and stability. The significant difference was not witnessed in the patients with laxity.
| Parameters | Mean | SD |
|---|---|---|
| Graft harvest time (min) | 8.16 | 1.51 |
| Graft length (cm) | 24.77 | 2.15 |
| Graft diameter (mm) | 8.48 | 0.50 |
SD: Standard deviation
Table 3 represents the mean IKDC score was 51.80 ± 8.16, which improved gradually till the 12-month follow-up to 95.09 ± 5.57, demonstrating the significant (P < 0.0001) improvement in patient condition. The Lysholm knee score was improved significantly (P < 0.0001) from preoperatively (50.78 ± 4.87) to 12-month (96.54 ± 3.93) follow-up as given in Table 4. The mean of AOFAS was calculated at the donor site both before the injury and at the 12-month follow-up appointment. The resulting score of 95.53 ± 5.02 indicated no significant difference between the two measurements. There was no discomfort around the ankle’s donor site, no pain or complaints about the ankle joint’s weakening, and no vascular or neurological issues observed. The comorbidities and complications have a significant impact on the recovery process and can make it difficult to assess the effectiveness of treatment. A very small proportion of the patients, i.e., 3 (2.88%), was observed with complications related to the pain while walking on the toes.
| Parameter | Follow-up period | Mean | SD | P value |
|---|---|---|---|---|
| IKDC score | Preoperative | 51.80 | 8.16 | - |
| 6-week | 67.83 | 7.42 | <0.0001 | |
| 6-month | 84.70 | 5.43 | <0.0001 | |
| 12-month | 95.0 | 5.57 | <0.0001 |
IKDC: International Knee Documentation Committee, SD: Standard deviation
| Parameter | Follow-up period | Mean | SD | P value |
|---|---|---|---|---|
| Lysholm knee score | Preoperative | 50.78 | 4.87 | - |
| 6-week | 68.86 | 4.19 | <0.0001 | |
| 6-month | 85.75 | 4.52 | <0.0001 | |
| 12-month | 96.54 | 3.93 | <0.0001 |
SD: Standard deviation
DISCUSSION
The principal discovery from this research was that the PLT appears to be an acceptable choice for ACL reconstruction, as it yields favourable functional outcomes, avoids possible complications associated with using a graft taken from the knee area, and has negligible impact on the ankle joint. PLT can now be considered to be a promising graft which is a safe and efficient alternative to other grafting methods based on the improved functional outcomes amongst the patients that went through arthroscopic primary ACL reconstruction. PLT autograft provides ease and takes less time to harvest, has adequate size, a greater ultimate tensile load, higher thickness and length of the graft, minimal donor-site morbidity, and satisfactory functional results along with improved stability scores of the knee, and after removal, the gait parameters are not affected by PLT and it does not cause instability over the ankle.14 The PLT offers a graft option that closely resembles the native ACL in terms of orientation and size. This anatomical similarity facilitates a more precise and anatomically accurate reconstruction, potentially enhancing knee joint stability.15
The selection of a graft is the primary preoperative factor to consider in ACL reconstruction. This decision plays a critical role in lowering the risk of re-injury and achieving optimal knee stability following the surgical procedure.16 In the first several days after implantation, an autograft experiences revascularisation and recollagenation with a 50% strength reduction. Therefore, the ACL graft substitute should be stronger as compared to the ACL.17 Length, diameter, and harvesting time of selected autograft in the ACL surgical procedure are another major factors contributing toward the graft failure.5 Also, Rhatomy et al.2 showed a remarkable correlation among the physical characteristics of the patients such as gender, weight, height, body mass index, and intraoperative graft’s diameter in ACL reconstruction procedure using PLT autograft in a retrospective cohort study. Considering all the factors, the graft harvesting time was 8.16 ± 1.51 min in our study which included variable graft length of 24.77 ± 2.15 cm and graft diameter of 8.48 ± 0.50 mm.
However, Fiil et al.18 showed increased postoperative sagittal laxity that was linked to an increased risk for revision surgery of ACL reconstruction and may also be linked to worsened knee-related quality of life and hindered athletic performance. Similarly, as per the multicenter cohort study by Ueki et al.19, hyperextension of the knee and higher preoperative pivot shift after anaesthesia were considered to be the risk factors for persistent pivot shift after one year of ACL reconstruction. In the present study, both conditions were observed to be negative.18,19
According to the patient reports, ACL reconstruction with PLT autograft results in satisfactory results, an intact and functional knee, low graft failure rates, and clinical outcomes that are considerably better.20 Setyawan et al.8 conducted a study to assess the functional results and morbidity at the donor site following single-bundle PLT autograft repair of the posterior crucial ligament (PCL) reconstruction. They observed a significant increase in functional score after two years of surgery. The mean IKDC score preoperatively and postoperatively was 47.58 ± 11.75 and 78.17 ± 4.52, respectively. The Lysholm score was 49.26 ± 11.54 preoperative; 80.20 ± 5.04 postoperative. The AOFAS was 93.26 ± 4.20 at the donor site.8 Joshi et al.4 evaluated the functionality and stability results of knee undergoing ACL reconstruction using PLT graft where they reported the mean IKDC score was 78.16 ± 6.23 postoperatively, and the mean AOFAS was 98.4 ± 4.1.4 In a study conducted by Singh et al., an inadequate hamstring graft was augmented with the anterior half of the peroneus longus during ACL reconstruction. The functional outcome was evaluated using the IKDC score at six weeks, three months, and six months that analysed its functional results, donor-site complications, and associated parameters. They observed the mean IKDC score at six months was 87.35.21 Likewise, the results of the present study also demonstrated that ACL reconstruction with PLT had a remarkable improvement with better clinical outcomes post 12-month follow-up resulting from IKDC and Lysholm scores. These results indicated that PLT autograft could potentially be used as the primary mode of treatment in ACL reconstruction with improved outcomes in patients with considering its strength, satisfactory ankle function, larger graft diameter, and preventing the occurrence of any potential complications.
Limitations
The limitations of this study are the limited sample size. The findings could not possibly be accessible to a larger population for the reason of the small sample size. A more objective clinical test needs to be used to reflect the true functions of the knee. The follow-up of 12 months in the study can also be a shortcoming, and further research could emphasise on a longer assessment of ACL reconstruction that uses peroneus longus autografts. Through a single surgeon, an identical rehabilitation system, and the same surgical approach helped to reduce bias.
CONCLUSION
PLT has been found to be a highly reliable and secure autograft option for the patients undergoing primary ACL reconstruction. The number of factors, including tensile load, graft length, thickness of the graft, shorter duration for graft harvesting, negligible donor-site morbidity, positive outcomes for donor ankle functional test (AOFAS score), and knee stability scores (IKDC and Lysholm score), collectively suggest that the selection of this graft demonstrates promising reliability, effectiveness, and viability. The use of PLT in ACL reconstruction contributes toward the advancement of surgical techniques in the field of orthopaedics. These benefits position PLT as a potential benchmark for other types of grafts in terms of effectiveness and safety.
Acknowledgment
The authors want to thank all the staff members of our department; the conduction of this study would not have been possible without their assistance. They are extremely thankful to the postgraduate students of our department for their technical support during the tenure of this study.
Ethical approval
The research/study was approved by the Institutional Review Board at Aatman Hospital, number ECR/1565/Inst/GJ/2021, dated 29th April 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Peroneus longus tendon autograft versus hamstring tendon autograft in anterior cruciate ligament reconstruction: A comparative study with a mean follow-up of two years. Archives Bone Jt Surg. 2022;10:695-701.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of anthropometric features on peroneus longus graft diameter in anterior cruciate ligament reconstruction: A cohort study. Ann Med Surg. 2019;48:77-80.
- [CrossRef] [PubMed] [Google Scholar]
- Predisposing factors for anterior cruciate ligament injury. Br J Sports Med. 2011;45
- [CrossRef] [PubMed] [Google Scholar]
- Peroneus longus tendon autograft for anterior cruciate ligament reconstruction: A safe and effective alternative in nonathletic patients. Niger J Surg. 2021;27:42-7.
- [CrossRef] [PubMed] [Google Scholar]
- Eversion and first ray plantarflexion muscle strength in anterior cruciate ligament reconstruction using a peroneus longus tendon graft. Orthop J Sports Med. 2019;7
- [PubMed] [Google Scholar]
- Peroneus longus autograft can be recommended as a superior graft to hamstring tendon in singlebundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019;27:3552-9.
- [CrossRef] [PubMed] [Google Scholar]
- All-inside singlebundle reconstruction of the anterior cruciate ligament with the anterior half of the peroneus longus tendon compared to the semitendinosus tendon: A two-year follow-up study. J Knee Surg. 2018;31:1022-30.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior cruciate ligament reconstruction with peroneus longus tendon graft: 2-years follow-up. Ann Med Surg. 2019;43:38-43.
- [Google Scholar]
- Predicting the peroneus longus tendon autograft size in ACL reconstruction by using anthropometric parameters: A study in South Sulawesi population. J Orthop. 2020;22:-4.
- [Google Scholar]
- All-inside anterior cruciate ligament reconstruction using an anterior half of the peroneus longus tendon autograft. Orthop J Sports Med. 2021;9
- [PubMed] [Google Scholar]
- Half-peroneus-longus-tendon graft augmentation for unqualified hamstring tendon graft of anterior cruciate ligament reconstruction. J Orthop Sci. 2015;20:854-60.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability and validity of the subjective component of the American Orthopaedic foot and ankle society clinical rating scales. J Foot Ankle Surg. 2007;46:65-74.
- [Google Scholar]
- Validity and reliability of the Thai versions of the Lysholm knee scoring scale and Tegner activity scale. Orthop J Sports Med. 2023;11
- [CrossRef] [PubMed] [Google Scholar]
- Peroneus longus tendon autograft for anterior cruciate ligament reconstruction: A safe and effective alternative in nonathletic patients. J Orthop Sports Med. 2023;5:133-8.
- [Google Scholar]
- The postoperative knee: Cruciate and other ligaments. InImaging of the Knee: Techniques and Applications. 2023:293-351. Berlin: Springer;
- [Google Scholar]
- Emerging trends in anterior cruciate ligament reconstruction. J Knee Surg. 2017;30:63-9.
- [Google Scholar]
- A high level of knee laxity after anterior cruciate ligament reconstruction results in high revision rates. Knee Surg Sports Traumatol Arthrosc. 2022;30:3414-21.
- [Google Scholar]
- Risk factors for residual pivot shift after anterior cruciate ligament reconstruction: Data from the MAKS group. Knee Surg Sports Traumat Arthros. 2018;26:3724-30.
- [CrossRef] [PubMed] [Google Scholar]
- Peroneus longus tendon autograft has functional outcomes comparable to hamstring tendon autograft for anterior cruciate ligament reconstruction: A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthros. 2021;29:2869-79.
- [Google Scholar]
- A study of the functional outcome of supplementation of hamstring graft with anterior half of the peroneus longus tendon in arthroscopic anterior cruciate ligament reconstruction. Cureus. 2022;14
- [CrossRef] [PubMed] [Google Scholar]




