
Translate this page into:
Percutaneous transforaminal endoscopic decompression and cageless percutaneous bone graft transforaminal lumbar interbody fusion: A feasibility study
Address for correspondence: Dr. Ajay Krishnan, C302, Orange Avenue, Maple County 1, Thaltej, Ahmedabad - 380 059, Gujarat, India. E-mail: drajaykrishnan@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Krishnan A, Barot MP, Dave BR, Bang P, Devanand D, Patel D, et al. Percutaneous transforaminal endoscopic decompression and cageless percutaneous bone graft transforaminal lumbar interbody fusion: A feasibility study. J Orthop Allied Sci 2018;6:S21-7.
Abstract
INTRODUCTION:
In the quest for better alternatives for open transforaminal lumbar interbody fusion (TLIF), minimally invasive surgery-TLIF (MIS-TLIF) has evolved, and feasibility studies of transforaminal endoscopic fusion are also getting reported in western literature. However, the cost of instrumented expandable cage may make it non-feasible for Indian setup whenever it will be commercially available.
METHODS:
This is a retrospective study of 13 patients of single-level percutaneous transforaminal endoscopic decompression and cageless percutaneous bone graft TLIF with percutaneous pedicle screw fixation under combined local with epidural anesthesia. The results of all patients as measured by validated tools of visual analogue score-Back and Leg, Oswestry Disability Index, patient satisfaction index, and fusion. The operating time, Estimated Blood Loss, Length of hospital stay and tolerance of patient for procedure was also scored.
RESULTS:
All the outcome measures were significant (P < 0.05) and fusion achieved in all with a mean follow-up period was 39 ± 6.36 months. Operating room time was 250.23 ± 52.90 min (187–327). Postoperative LOH hospital stay was 29.92 ± 4.94 h (24–39). The tolerance score was 2.30 ± 0.85 (1–3). One superficial bone graft site infection resolved with antibiotics.
CONCLUSION:
It not appealing to be recommendable to general population inspite of it being low cost and with negligible complications. Further research and engineered tools are needed to reduce the operating time.
Keywords
Endoscopy
minimally invasive surgery
percutaneous
transforaminal lumbar interbody fusion

Introduction
Spinal fusion with open transforaminal lumbar interbody fusion (TLIF) when required in the selected patient proves to be effective in improving leg/mechanical back pain, function, and overall quality of life.[1] However, the economic, psychological, and social aspects of the procedure should be understood till the outcome is achieved. And now, many patients have consciously started resisting having an open procedure due to concerns over the morbidity of the procedure, with the additional reasons cited are recovery time and risk.[2-5] Over the past decade, minimally invasive surgery-TLIF (MIS-TLIF) with varying modifications and alternative ways has become very popular for achieving fusion.[4-6] The use of tubular dilators still requires an open incision which though definitely reduces invasiveness but still does damage posterior musculature and removes facet.
Hence, the quest continues for the search for newer surgical methods of MIS to reduce invasiveness and preserve more anatomy with less blood loss, less pain, shorter hospital stay, and quicker recovery. Percutaneous transforaminal endoscopic discectomy (PTELD) is getting famous and exponential rise of reports in literature with excellent outcomes is now coming.[7-14] In India, Dr. S. Gore from Pune introduced this state of art technique in 1999. Thanks to his persistent and never-ending efforts; the number of surgeons who can perform transforaminal surgery has increased, giving reasonably great outcomes of discectomy all around India. As knowledge, skill, and technology evolves, extrapolation of the acquired confidence into other possible applications starts.
Now, transforaminal endoscopic visualized or indirect decompression, with or without interbody expandable/nonexpandable cages (with or without osteobiologics to enhance fusion), percutaneous fixation (facet or pedicle screws) employing long-acting local anesthetics or general anesthesia are getting reported in literature.[15-22]
This feasibility report examines the short-term outcome of percutaneous transforaminal endoscopic decompression and cageless percutaneous bone graft TLIF (pbTLIF) with percutaneous pedicle screw fixation under combined local with epidural anesthesia and literature study.
Methods
This report is a retrospective analysis of a case series of patients treated with pbTLIF at a single institution. The patients were operated by author (AK) at a peripheral center with required basic facilities for this type of surgery. All patients were operated with an informed consent. All potential complications explained and if required the need to convert to open surgery at the time of index surgery or later on was as well informed. A total of 13 patients with follow-up more than 2 years were included. The patients' baseline demographic characteristics were evaluated with diagnosis, level, operative room (OR) time, estimated blood loss (EBL), postoperative length of hospital stay (LOH), and perioperative complications. Validated outcome measures of the Oswestry Disability Index (ODI), visual analog score (VAS) L (leg), VAS B (back), and patient satisfaction index were used to interpret the outcome. These are all validated measurement methods. A nonvalidated self-made tolerance scale was recorded which was to assess patients' comfort for the surgery and taken after the surgery. The grading was as follows: L = did not feel any discomfort/bad pain, 2 = well but some mild tolerable, 3 = poor, and 4 = unable to tolerate. Preoperative and periodical timeline outcome were analyzed.
An independent anesthesiologist was present during the whole surgical procedure. Patients were operated in a prone position with soft vertical placed two bolsters on either side. The protected position is given, and free nominal movement of the upper limb and hip, knee, foot, and head was allowed as per comfort of patient to counter fatigue. The patients were operated under conscious sedation with local anesthesia. Supplemental oxygen is given through a nasal cannula. 45 min before surgery, intramuscular midazolam (0.05 mg/kg) and diclofenac are given. There is titrated infusion of dexmedetomidine (0.5–1.0 μg/kg given slowly half dose in 15 min and then as needed the remaining dose) and with fentanyl (bolus dose of 1.0 μg/kg intravenously given 10 min before incision puncture followed by additional doses as needed). This cocktail allowed for continuous feedback from the patient during the entire procedure till decompression and is a live neuromonitoring. Epidural catheter was placed in all cases because of novice procedure which may extend longer duration and was used only later while harvesting bone graft and insertion of percutaneous screws. However, the endoscopic decompression and endplate preparation were done under conscious sedation only.
An uniportal unilateral approach was used [Figure 1]. An imaginary line drawn to the annular puncture site in the skin and surgical trajectory is planned. This varied depending on level of surgery and patient decubitus. The angle is between 20° and 40°, and the puncture point is 12–15 cm from midline. The intended needle entry tract is infiltrated with 8 mL to 10 mL of 1% lidocaine plus bupivacaine 1:1 ratio. A 16-gauge needle was inserted in the safe triangle and confirmed fluoroscopically with patient feedback for safety at all steps. Four milliliters of 0.5% dilution of the mixture was infiltrated on the surface of the annulus. A 7-mm incision was put, and with progressive tissue dilating trocar, a 8 mm beveled working cannula was placed sequentially, and then through the endoscope, an inside-out decompression was done with removal of offending compression (Carl Storz, Germany-Gore System). Disc prolapse excision was done. A visualized foraminoplasty and lateral recess decompression when required were also done till traversing or exiting root decompression, respectively, as needed is completed satisfactorily [Figure 2]. Nouvag drill system was used. After the decompression, the cannula is again advanced to center of disc and the degenerated nuclear material is removed with the use of graspers and shavers. Endplate is prepared with curettes and rasps and confirmed under endoscopic visualization. A possible 90%–100% of the nucleus pulposus was removed while integrity of the annuluses was maintained. The endplate showing paprikas sign (punctate petechial bleeding) was considered as a prepared endplate.

- (a) Image intensifier endoscope position while decompressing which is then further withdrawn to complete the foraminoplasty. Percutaneous pins in situ with endoscope in position clinical picture (b) and corresponding image intensifier view (c)
![Endoscopic view: (A) Visualized foraminoplasty with Nouvag burr. (B) Discal decompression [c] with just visible traversing nerve root [b] with compressing ligament flavum [a] (C) after removal of ligamentum flavum optimally the decompressed nerve root is more visible [b*] and pulsatile peroperatively](/content/178/2018/6/Suppl 1/img/JOAS-6-S21-g002.png)
- Endoscopic view: (A) Visualized foraminoplasty with Nouvag burr. (B) Discal decompression [c] with just visible traversing nerve root [b] with compressing ligament flavum [a] (C) after removal of ligamentum flavum optimally the decompressed nerve root is more visible [b*] and pulsatile peroperatively
At this point, epidural anesthesia was given. Cancellous bone graft was extracted by an indigenized percutaneous way with an incision of 1.5 cm placed over the posterior iliac spine. This is with a hollow mill type system with a trocar. Then, 8–10 g of cancellous bone graft extracted was mixed with 5 g of hydroxyapatite and pushed through the working sheath under fluoroscopic control and impacted. After retrieving the endoscope, the skin was sutured with subcuticular stitches. We applied additional percutaneous pedicle screw fixation through separate incisions of 2 cm in all of our patients [Figures 1 and 3]. No attempt of restoration of height or reduction was made. No neuromonitoring or access system (other than the endoscope) or biologic bone substitutes were used.
![(a) Percutaneously extracted bone graft from iliac crest. (b) Body incisions and access ports: incision 2 cm each for the percutaneous screws [*] 1.5 cm incision for bone graft extraction [#] and 7 mm incision [@] of endoscope access](/content/178/2018/6/Suppl 1/img/JOAS-6-S21-g003.png)
- (a) Percutaneously extracted bone graft from iliac crest. (b) Body incisions and access ports: incision 2 cm each for the percutaneous screws [*] 1.5 cm incision for bone graft extraction [#] and 7 mm incision [@] of endoscope access
All patients were permitted ambulation in the upright position on the same day of surgery using a firm lumbar orthosis. We discharged the patients within 2 days of surgery when the patient felt at comfort.
The patients' indoor case and outpatient records were analyzed for data acquisition till the last follow-up. All patients had preoperative dynamic radiographs and magnetic resonance imaging. All the X-rays (anteroposterior, lateral, and flexion/extension views) and computed tomography scan films at final follow-up were also analyzed for stability, implant position, union, and disc height (DH). DH measurement was done at the posterior intervertebral discal margin on neutral position lateral radiograph, and the difference between immediate postoperative to final follow-up in millimeters was the DH loss and indicates the collapse.
Statistical analysis
Data were expressed as mean ± 2 standard deviation (range of minimum-maximum) for demographic variables. To examine the pre- and post-operative difference of score, Wilcoxon signed-ranks test was used. Paired t-test could not be used due to the small sample size and also because the assumptions of parametric test were not getting fulfilled. The McNemar test would be more appropriate for this, but it was not performed because the compared variables were not dichotomous with the same values. All tests are two sided and statistical significance was set at P < 0.05. All analyses were carried out using the SPSS Inc. Released 2008. SPSS Statistics for Windows, Version 17.0. Chicago: SPSS Inc.
Results
All surgeries were performed on the L4–L5 level in 9 patients, on the L5-S1 level in 4 patients. All patients of L5-S1 were of low iliac crest.
The average age was 55.23 ± 7.29 (45-71) years. There were 5 males and 8 females. The average surgical OR time was 250.23 ± 52.90 min (187–327), and EBL was 47.70 ± 12.35 ml (30–70). Postoperative LOH hospital stay was 29.92 ± 4.94 h (24–39). The tolerance score was 2.30 ± 0.85 (1–3). Pain control in postoperative period and after discharge was achieved using a combination of diclofenac (max 150 mg), tramadol (max 100 mg), paracetamol (max 4 gm), alprazolam and pregabalin 75 mg. In elderly patients, dose was kept toward lower side.
The mean follow-up period was 39 ± 6.36 months (25–47). Patient diagnoses included degenerative disc disease (DDD) in 3 patients and additional lumbar disc herniation (LDH) in 1 patient. LDH with instability in 3 patients, lumbar canal stenosis (LCS) with listhesis in 3 patients and LCS with facet arthritis in 3 patients. No patient needed open surgery to be converted. Ambulation was started on the same day of surgery in all patients.
Preoperative VAS-B and VAS-L pain scores were 8.39 ± 1.04 (7–10) and 8.84 ± 0.90 (7–10), which improved to 2.08 ± 0.76 (1–3) and 1.35 ± 0.96 (0–3) at 6 weeks and was at final follow-up 0.77 ± 0.83 (0–2) and 0.92 ± 1.04 (0–3), respectively. Preoperative ODI was 75.97 ± 12.78 (55.56–95.56) which improved to 36.58 ± 11.46 (15.56–53.33) at 6 weeks and was 34.19 ± 8.91 (17.78–51.11) at final follow-up. The improvement on mean values was a 90.82%, 89.59%, and 55% improvement from the preoperative period to final follow-up for VAS-B, VAS-L, and ODI, respectively. The patient satisfaction index was 2.46 ± 0.67 (1-3) at final follow-up. All improvements in the scores were statistically significant (P < 0.05).
Fusion was achieved in all 13 patients and showed no segmental motion on their flexion-extension radiographs at their final follow-up. DH loss of 1.50 ± 0.46 mm (1–2) at the last follow-up visit was noted, and no broken/loose implants were noted.
No transitory dysesthesia was observed. No major complications such as a dural tear, cerebral spinal fluid leakage, and neurologic injury occurred in any of the patients. One patient with superficial skin infection at bone graft extraction site was noted at the time of stitch removal without any general symptoms and responded favourable to oral antibiotics and dressing.
Discussion
Open surgery of the lumbar spine, though address the pathology adequately, may lead to complications that can cause disability in patients.[2-5,23,24] Not just complications, excessive dissections of the spine may lead to prolonged surgical duration and anesthesia, blood loss requiring transfusion, prolonged hospital stay, stronger and longer analgesic intake, protracted rehabilitation, and incomplete recovery due to collateral damage.[2-6,21-26] A combination of MIS with variable pain management protocol has been reported to accelerate recovery after TLIF and done in outpatient setup. However, significant use of analgesics under modified protocols is still needed.[2,3] Aggressive pain management with epidural injections has also been reported with good efficiency.[27]
As can be seen in literature, the aim is on quick recovery to make it possible as outpatient surgery.[2,3] While quick recovery following PTELD surgery has been achieved with undoubtedly the access related damages being the least,[7-14] obtaining these long-term results with fusion surgery is awaited though looks promising.[15-22]
A varied spectrum for indications like DDD, LCS, listhesis and LDH, fresh as well as revision cases treated with endoscopic TLIF have been reported.[1,2,6,23,24] Indications of this endoscopic fusion surgery reported varies. Revision cases finds more favour due to its virgin access.[18-22] Difficult indications in collapsed disc space and listhesis reduction have been achieved with these techniques.[16,19,22] However, we chose only patients in whom no intention to restore the height or listhesis was there. Our indications were simpler indications who needed stabilization and decompression. There was no need to alter the balance or alignment of the spine. However, all cases were having significant disability scores and associated compressive and mechanical back pain. Bilateral arthroscopic approach was used in few series.[16,20]
Doing the surgery under local anesthesia with sedation creates exact setup to expedite the discharge of patient.[15,20,22] The method of conscious sedation offers the surgeon live feedback as the patient will respond to this painful stimulus. In addition, this reduces the side effects of general anesthesia, such as nausea, dysphagia, and memory loss.[7-15,20,22] In our series also, we had done all the decompressive surgery under local anesthesia. However, as the surgical duration was the main constraint, we used supplemental epidural anesthesia for the second half of the continuum surgery.
A few series have mentioned the use of general anesthesia because of the regional cultural protocol and the patient demand, but it needs intraoperative neuromonitoring to do so.[16,19,21] In spite of having followed neuromonitoring protocols, the incidence of dysesthesia and neurological worsening are discouraging.[21] These neurological sequelae may be due to nonvisualized expansion of the Kambin's triangle also in addition to the larger size port used.[19-21] This though expedites the preparation and the expandable cage insertion as well as helps in indirect decompression.[19] This increased the size of incision to 11.5 cm also. In few of the series the preparation was through the working cannula of traditional endoscope and incision size was small and remained around 8 mm. These series also had very low incidences of dysesthesia or worsening.[15,22] Our incision size was also the same, and for probably the same reason, we had no neurological worsening or dysesthesia. Expanding the access port should be seen with caution in further improvisation in future.
The duration of surgery varied from 60 to 251 min in various series.[15-22] Our reported OR time has been highest and the only negative aspect of the series. OR time can be reduced by enhancing the working channel size and technologically made sturdier endplate preparation instruments and with the usage of osteobiologics.[19] In our series, endplate preparation was the most time-consuming part of the surgery but we had no neural worsening or dysesthesia inspite of prolonged time. Looking to the increased neural worsening sequelae reported with wider working channel,[20,21] better engineering and research to make expandable preparatory reamers without increasing the size of the working channel is recommended.
Short-term outcome as in the literature setting aside the complications has been comparable to the outcomes of open TLIF and MIS TLIF with validated measures of VAS, ODI, and/or Macnab's Criteria.[1,2,6,15-24,28] Our outcomes were superior to all series in terms of VAS and ODI. The minimum clinically important difference for lumbar spinal fusion surgery is considered in these results using established spinal outcome measures.[29] Though in another series, the technique was introduced in a group of patients with comorbid conditions, the complication rate of 36% with moderate improvement in outcome is doubted by author himself.[20]
Variable range of rate of pseudoarthrosis (0%–5.6%), cage breakage (nonsymptomatic in 27.77%[22]) or symptomatic migration (5.56%[22] and 26.31%[20]), and revision surgeries (11.11%[22] and 22.8%[20]) also are reported. However, in our series, there was no implant failure and pseudoarthrosis [Figures 4 and 5]. DH at final followup as compared to immediate post operative period showed a loss of 1.50 ± 0.46 mm (1–2). Rather than relying on palpation with probes, use of arthroscopic visualization of the endplate preparation confirms the adequacy of the bed preparation visually.[16] We also agree with the same and may be the possible reason for greater fusion rates. Biologics were used in few studies[15,16,19,21] which increase the fusion rates. However, it should be skeptically used looking at the symptomatic ossification which has been reported in other series.[30] Moreover, the disadvantages of steeper learning curve and irradiation to patient and surgeon are to be considered.[30,31]
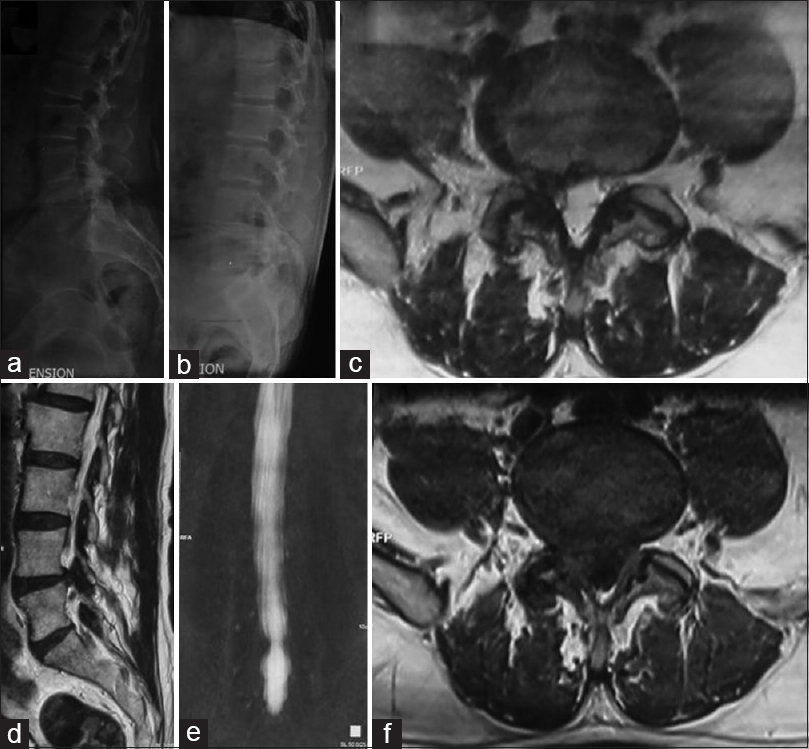
- A 68-year-old male with unilateral right-sided radiculopathy and back pain for 14 months. (a and b) Radiograph lateral flexion and extension views showing instability Grade 1 listhesis. (c-f) Magnetic resonance imaging T2-axial, T2-parasagittal, coronal magnetic resonance myelogram, and T1 axial sequences showing a lateral recess stenosis right side with facetal arthritis/sagittal facet with a small disc prolapse

- (a and b) Postoperative radiograph anteroposterior and lateral showing good alignment with bone graft and interbody hydroxyapatite (c-e) follow-up flexion/extension lateral and anteroposterior radiograph at 47 months showing stable construct with union and disc height loss of 2 mm. (e and f) Computed tomography scan showing incorporation of the graft across endplate. Preoperative disability significant with an ODI 95.56 that improved to 40.00 at 6 weeks and 35.6 at 47 months postoperative
This study has significant limitations. This is an initial report, and the sample size is too small to draw definitive conclusions as to efficacy and safety. Literature series are also small with 10, 60, 1, 30, 57, 2, and 18 numbers of patients, respectively, with variations of technique and indications, so all appears to be feasibility studies rather than making recommendations.[15-22] The percutaneous method of bone graft harvesting is a novice unpublished method with its instruments not made through research regulatory approvals or patent. However, we have been using this method of harvesting in MISS TLIF and cervical discectomy with cage assisted fusion, where small quantity of bone graft (<10 gm) is needed. The endplate preparatory instruments were also novice and also unapproved and nonvalidated. However, patient consent was taken about all aspects including the trial for benefits and complications. Though it was clearly very safe with no major drawback except the OR time, this series has not been extended further and stopped. Even though the patient satisfaction index[32] was very high at final follow-up, the high tolerance score (low tolerated procedure comfort) taken after surgery was a negative aspect about the procedure comfort. This tolerance score is a nonvalidated score, but similar scores have never been reported in percutaneous endoscopic lumbar discectomy procedures also. We wanted to evaluate it and put it on paper. Ultimately, this procedure must be able to produce an arthrodesis rate equivalent to open procedures and also has secondary gains without increasing any complications. The learning curve has to be relatively easy and reduced operative time is mandatory. In this case series, we were able to demonstrate that with use of this novel method, patients were able to be discharged rapidly from the hospital following single-level pbTLIF surgery and have very good immediate and follow-up outcome. This series represents our efforts in Indian setup to use a combination of several innovative techniques and technologies to do an endoscopic lumbar spinal fusion surgery.
This trend of outpatient surgery is due to increasing economic constraints to reduce postoperative inpatient care and indirectly the costs of surgery.[33-35] In long run in many conventional fusion cases, failure to return to a patient's prior occupation and increased cost to the individual and society are huge.[16] Hence, there will likely be an increasing trend toward techniques that permit outpatient spinal fusion surgery. Although a innumerable list of spine surgery falls under the umbrella name of “minimally invasive spine surgery,” it is now necessary to consider redefining and grading MIS surgeries and be vary of misnomers of MIS surgical procedures,[16] and even endoscopy or percutaneous terms are loosely used.
Conclusion
The limitation of triangular operating space has been the most important factor for low level of enthusiasm for endoscopic approach by spine surgeons until now. However, with teaching masters expertise, teaching tools, fast-rising technological improvement in endoscope, expandable preparatory instruments, and implantable cages with biologics, it is expected that this very versatile approach will become the most preferred method to achieve interbody fusion in a true ultraminimally invasive way in future. However, in the current form, this selected procedure is not suitable for patients with severe central and lateral recess stenosis as it can only achieve limited decompression. The method followed in this series also cannot be recommended looking to the OR time taken, but the outcome is too good and promising.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Who should undergo surgery for degenerative spondylolisthesis? Treatment effect predictors in SPORT. Spine (Phila Pa 1976). 2013;38:1799-811.
- [CrossRef] [PubMed] [Google Scholar]
- Feasibility and patient-reported outcomes after outpatient single-level instrumented posterior lumbar interbody fusion in a surgery center: Preliminary results in 16 patients. Spine (Phila Pa 1976). 2015;40:E36-42.
- [CrossRef] [PubMed] [Google Scholar]
- Same-day discharge after minimally invasive transforaminal lumbar interbody fusion: A series of 808 cases. Clin Orthop Relat Res. 2014;472:1806-12.
- [CrossRef] [PubMed] [Google Scholar]
- Two-year clinical and radiographic success of minimally invasive lateral transpsoas approach for the treatment of degenerative lumbar conditions. SAS J. 2010;4:41-6.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive treatment (XLIF) of adjacent segment disease after prior lumbar fusions. Internet J Minim Invasive Spinal Technol. 2009;4:1-7.
- [Google Scholar]
- Instrumented minimally invasive spinal-transforaminal lumbar interbody fusion (MIS-TLIF); minimum 5-years follow-up with clinical and radiologic outcomes. 2012. J Spinal Disord Tech. [Epub]. http://dx.doi.org/10.1097/BSD.0b013e31827415cd
- [Google Scholar]
- New emerging gore matrix: Basis of stitchless spine surgery under local anesthesia. J Orthop Allied Sci. 2017;5:1-5.
- [Google Scholar]
- Arthroscopic discectomy of the lumbar spine. Clin Orthop Relat Res (337):49-57.
- [CrossRef] [PubMed] [Google Scholar]
- Posterolateral arthroscopic discectomies of the thoracic and lumbar spine. Clin Orthop Relat Res (304):122-9.
- [CrossRef] [Google Scholar]
- An extreme lateral access for the surgery of lumbar disc herniations inside the spinal canal using the full-endoscopic uniportal transforaminal approach-technique and prospective results of 463 patients. Spine (Phila Pa 1976). 2005;30:2570-8.
- [CrossRef] [PubMed] [Google Scholar]
- Posterolateral percutaneous endoscopic lumbar foraminotomy for L5-S1 foraminal or lateral exit zone stenosis. Technical note. J Neurosurg. 2003;99:320-3.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic transforaminal discectomy for recurrent lumbar disc herniation: A prospective, cohort evaluation of 262 consecutive cases. Spine (Phila Pa 1976). 2008;33:973-8.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous endoscopic approach for highly migrated intracanal disc herniations by foraminoplastic technique using rigid working channel endoscope. Spine (Phila Pa 1976). 2008;33:E508-15.
- [Google Scholar]
- Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complications in 307 consecutive cases. Spine (Phila Pa 1976). 2002;27:722-31.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic minimally invasive transforaminal interbody fusion without general anesthesia: Initial clinical experience with 1-year follow-up. Neurosurg Focus. 2016;40:E13..
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic transforaminal decompression, interbody fusion, and percutaneous pedicle screw implantation of the lumbar spine: A case series report. Int J Spine Surg. 2012;6:157-66.
- [CrossRef] [PubMed] [Google Scholar]
- Full endoscopic transforaminal lumbar interbody fusion approach with percutaneous posterior transpedicular screw fixation in a case of spondylolisthesis grade I with L4-5 central stenosis. J Crit Spine Cases. 2010;3:115-9.
- [Google Scholar]
- Endoscopically assisted transforaminal percutaneous lumbar interbody fusion. In: Lewandrowski KU, Lee SH, Ipenburg M, eds. Endoscopic Spinal Surgery. London, UK: JP Medical; 2013. p. :129-34.
- [CrossRef] [Google Scholar]
- Percutaneous transforaminal lumbar interbody fusion (pTLIF) with a posterolateral approach for the treatment of denegerative disk disease: Feasibility and preliminary results. Int J Spine Surg. 2015;9:41..
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous endoscopic transforaminal lumbar interbody fusion: Is it worth it? Int Orthop. 2013;37:1507-10.
- [CrossRef] [PubMed] [Google Scholar]
- True percutaneous transforaminal lumbar interbody fusion: Case illustrations, surgical technique, and limitations. J Neurol Surg A Cent Eur Neurosurg. 2016;77:344-53.
- [CrossRef] [PubMed] [Google Scholar]
- Corrigendum to “Percutaneous transforaminal endoscopic lumbar interbody fusion: Clinical and radiological results of mean 46-month follow-up" Biomed Res Int. 2017;2017:3431257..
- [CrossRef] [PubMed] [Google Scholar]
- Lumbar spinal fusion. A cohort study of complications, reoperations, and resource use in the medicare population. Spine (Phila Pa 1976). 1993;18:1463-70.
- [CrossRef] [PubMed] [Google Scholar]
- Complications associated with single-level transforaminal lumbar interbody fusion. Spine J. 2009;9:623-9.
- [CrossRef] [PubMed] [Google Scholar]
- Back muscle injury after posterior lumbar spine surgery. Part 1: Histologic and histochemical analyses in rats. Spine (Phila Pa 1976). 1994;19:2590-7.
- [CrossRef] [Google Scholar]
- Back muscle injury after posterior lumbar spine surgery. Part 2: Histologic and histochemical analyses in humans. Spine (Phila Pa 1976). 1994;19:2598-602.
- [CrossRef] [Google Scholar]
- Pre-incisional caudal epidural blockade and the relief of pain after lumbar spine operations. Int Orthop. 1997;21:62-6.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive versus open transforaminal lumbar interbody fusion for degenerative spondylolisthesis: Comparative effectiveness and cost-utility analysis. World Neurosurg. 2014;82:230-8.
- [CrossRef] [PubMed] [Google Scholar]
- Minimum clinically important difference in lumbar spine surgery patients: A choice of methods using the oswestry disability index, medical outcomes study questionnaire short form 36, and pain scales. Spine J. 2008;8:968-74.
- [CrossRef] [PubMed] [Google Scholar]
- Symptomatic ectopic bone formation after off-label use of recombinant human bone morphogenetic protein-2 in transforaminal lumbar interbody fusion. J Neurosurg Spine. 2010;12:40-6.
- [CrossRef] [PubMed] [Google Scholar]
- Learning curve and clinical outcomes of minimally invasive transforaminal lumbar interbody fusion: Our experience in 86 consecutive cases. Spine (Phila Pa 1976). 2012;37:1548-57.
- [CrossRef] [PubMed] [Google Scholar]
- Patients' expectations and satisfaction in lumbar spine surgery. Spine (Phila Pa 1976). 2005;30:2689-94.
- [CrossRef] [PubMed] [Google Scholar]
- Can computer-assisted surgery reduce the effective dose for spinal fusion and sacroiliac screw insertion? Clin Orthop Relat Res. 2010;468:2419-29.
- [CrossRef] [PubMed] [Google Scholar]
- An analysis of the differences in the acute hospitalization charges following minimally invasive versus open posterior lumbar interbody fusion. J Neurosurg Spine. 2010;12:694-9.
- [CrossRef] [PubMed] [Google Scholar]
- Acute hospital costs after minimally invasive versus open lumbar interbody fusion: Data from a US national database with 6106 patients. J Spinal Disord Tech. 2012;25:324-8.
- [CrossRef] [PubMed] [Google Scholar]




