
Translate this page into:
Stable, developmental; LUMBAR canal stenosis: Rethink needed
Address for correspondence: Dr. Satishchandra Gore, 1128 Shivajinagar FC Road, Mission Spine, Pune - 411 016, Maharashtra, India. E-mail: yesgore@yahoo.co.in
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gore S. Stable, developmental; LUMBAR canal stenosis: Rethink needed. J Orthop Allied Sci 2018;6:S3-7.
Introduction
The author is proposing a new way of looking at clinical analysis, imaging, anatomy, pathology, and a surgeon's approach to cover the likely causative pathology during transforaminal endoscopy in an awake and aware patient for symptomatic developmental stenosis. In patient with discogenic back pain and sciatica, the treatment planning and execution has changed as we have access to the pain generator during surgery in awake and aware patient,.[1,2] In case of stenosis since we are treating patients who are stationary at surgery but with symptoms only on movements of walking or prolonged standing, they being awake may not make much difference to symptom analysis or real-time change in symptoms during intervention but since most are aged patients it does make a difference as most associated medical comorbidities can be tackled better during intervention under local anesthesia in our stitchless surgery. We need to apply our mind to rethink concepts on claudication in developmental lumbar stenosis and utility of what we do and why we do it?
Clinical Analysis
The routine symptoms of claudication point to lumbar canal changes and we assess this by analysis of the narration, images, using knowledge from cadaver dissections, and in vivo visualization of the likely cause. Symptoms and signs such as low back pain, bilateral sciatica, intermittent claudication, leg paresthesia, numbness, motor weakness, and in severe cases, bowel or bladder dysfunction are seen.
In case of a patient presenting with claudication, we start with differentiation of most dominant cause, namely vascular or neurogenic. Then if it is neurogenic, it can be a stable or unstable spine with a dynamic instability. Only dynamic imaging can clarify this. If it is neurogenic claudication, then we start exploring if it is present on both sides in lower limbs or only one side. Many times, a bilateral symptom is thought to indicate a central pathology but may not be so. Clinical assessment of developmental lumbar stenosis with respect to claudication is now refined with use of assessment scales.[3] Weiner has proposed a scale, and we also use other modified scales.[4] Specific scales FUKUSHIMA FLS 25 have been proposed and are found effective.[5] It highlights the dominance of numbness than pain as clinical presentation. Standing time, walking distance, and time are found important in assessment. Foraminal stenosis and canal stenosis for L5 root, for example, at L5S1 and L45 can be distinguished by the presence of pain at rest in L5 in case of foraminal stenosis at L5S1. Swelling is observed in MRI scans over DRG in foraminal causes and never in canal causes.
The involvement of bladder in severe stenosis or an aged patient needs more attention. Detrusor underactivity can be better assessed by a noninvasive bedside investigation namely ultrasonography for postvoid residue. We propose a value of 60 ml in female and 100 ml in male patients (unpublished data). Regular use of this assessment has led us to believe that detrusor underactivity is commonly not adequately evaluated leading to dissatisfaction in patients about intervention due to post opeartive retention. It may need long-term rehabilitation in aged patients seeking relief.[6-8]
Imaging
Lumbar spinal developmental stenosis is compression of DRG and roots by hypertrophy of soft-tissue structures. It is thought that there is a good correlation of bony measurements and the size and dural sac measurements, but that is not essentially proven yet. Various canal shapes have been mentioned and likely correlation of shape and symptoms has been made. About central stenosis the “central” compression over dural sac with roots inside can be from front and from the back. The back cause has been seen most prominent at the level of superior facets. Computed tomography (CT) magnetic resonance imaging (MRI) cuts at different levels in plane of the disc and not in plane of the facet may not indicate the real culprit. Literature on CT MRI about bony measurements is not much relevant as it cannot direct us to the causative soft-tissue pathology with certainty. Image misses the most important area of the superior articular process (SAP) and its soft-tissue cover that is now increasingly thought to be the causative pathology. It is mentioned that 80% of patients have the maximum likely encroachment at SAP tip level [Figure 1a and b].[9,10]
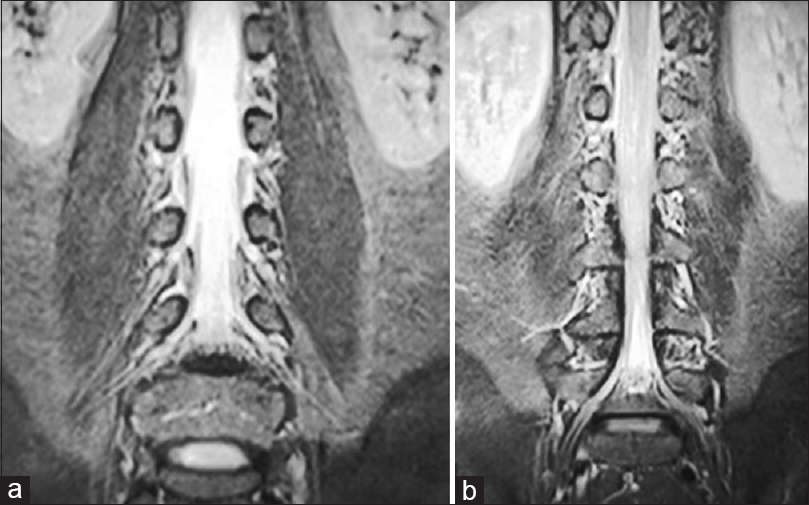
- (a) Coronal image magnetic resonance imaging showing the DRG in foramen at L45. (b) Shows a SAP forming roof of the DRG in lumbar foramen in a more dorsal section
Figure 1a shows the coronal MRI location of DRG in foramen with tissue medial and ventral to the facet and SAP in foramen that is much closer and relevant to DRG compression. The DRG here is lateral and outside medial pedicle line and ligamentum flavum forming roof of the foramen too is well spread laterally beyond medial pedicle line. Transforaminal endoscopy access in foramen is by landing at the medial pedicle line and thus lateral ligamentum flavum relevant to DRG compression is directly at roof of foramen for endoscopists.
This coronal section B highlights the superior facet tissue and relevant to DRG compression and is an earlier dorsal coronal cut versus previous image A. Since the etiopathogenesis of claudication is thought to be arising from DRG and its blood supply and not dural sac compression, we need to be more aware about the anatomy of the roof of the foramen. This essentially includes SAP, facet joint and its soft tissue cover. This soft tissue may hypertrophy and compress the DRG and its vasculatature.
In foraminal stenosis, foramen is smaller on symptom side, and there is decreased lumbar lordosis, decreased disk height, increased facet degenerative change on the symptomatic side, more hypertrophied soft tissue covering SAP and Grade III modic changes in comparison to isolated central stenosis.
MRI classification of Wildermuth classifies the grade of stenosis with respect to the presence of epidural fat and its quantity. In severe stenosis, fat decreases considerably. Results of the survey suggest that there are no broadly accepted quantitative criteria and only partially accepted qualitative criteria for the diagnosis of lumbar spinal stenosis. The latter include disk protrusion, lack of perineural intraforaminal fat, hypertrophic facet, absent fluid around the cauda equina, and hypertrophied ligamentum flavum. Even in symptomatic patients, normal diameter of the spinal canal was noticed in 32% of cases. And in asymptomatic cases, canal narrowing was noticed.[11] Detailed history and clinical examination of the patient along with the radiological investigation of stenosis with MRI scan is expected to establish the diagnosis.[12] Measurement of bony canal measurements is totally irrelevant to DEVELOPMENTAL stenosis. They do not consider the soft tissue and may be more important in patients with achondroplasia or congenital central stenosis. In traditional studies most severe stenosis is found at facet level, and difference in bony canal and dural sac area shows the significance of soft-tissue hypertrophy. MRI myelography may be more helpful in preoperative diagnosis of stenosis. It shows the swelling of the nerve and alterations in its course better.
Anatomy
Our new understanding about symptom causation is heightened by work on ligamentum flavum dissections from ventral aspect,[13,14] a recent imaging study with oblique coronal images[15] and three-dimensional fusion images from CT and MRI images in symptomatic patients.[16] The pathophysiology and cause of nerve or DRG involvement would essentially lie in the upper foramen closer to tip of SAP.
There is a very significant lacuna in our traditional understanding of true anatomy and spread of the ligament. Ventral dissection of the bed of dural sac formed by the ligamentum flavum reveals five types of ligament anatomy in its location and lay[13]. The main finding in that study has been ligamentum flavum laterally is attached to lower pole of the upper pedicle in foramen. This should change our approach to the treatment planning in lateral canal and towards managing claudication in lower lumbar canal stenosis. The area under pedicle in foramen is very difficult to access in posterior midline access as it involves cutting too much bone from facet, that some times may result in iatrogenic fracture of pars. In a sense whatever decompression we do by posterior midline access may be indirect with respect to DRG [Figure 2].
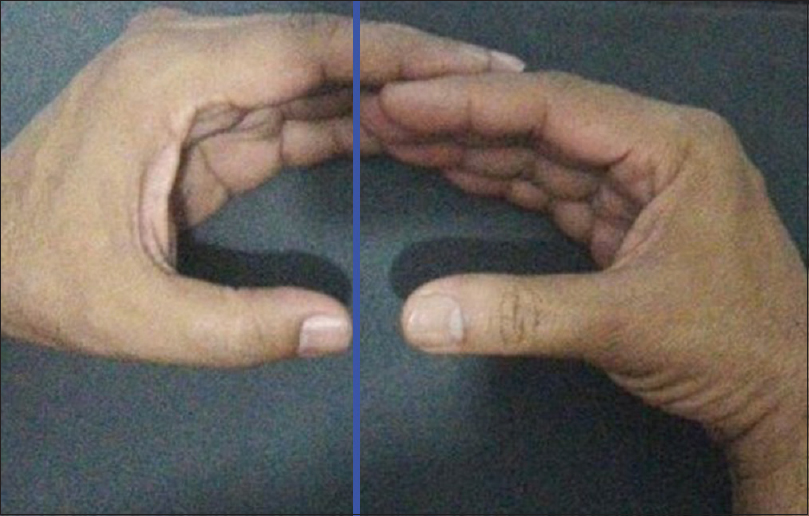
- A simple way to explain foramen and its unyielding, unchanging walls
We are looking at left foramen L45, left hand denotes L4, index finger is inferior facet, thumb is body of L4, right thumb is L5 body and right index is superior facet and tip of index of the right hand is SAP [Figure 2]. If we go by understanding anatomy of the foramen only area that can really change with degeneration and developmental changes is facet ventral surface and the posterior annulus. The bony C of upper vertebra and U of lower vertebra do not show any change. The ventral surface of facet can show soft-tissue hypertrophy that may turn calcified or even ossified over tip of SAP and the posterior annulus (posterolateral part to be precise in foramen) may give rise to symptoms due to an annular tear or a herniated fragment. IT can also generate symptoms by getting hard collagenized in a chronic annular tear with intermittent prolonged healing. That needs a very judicious annulectomy in foramen for the lowering of floor in foramen. DRG is intraforaminal in majority of patients at L45 and at just outside foramen at L34 and just inside at L5S1.
Ligamentum Flavum
Central interlaminar part of ligamentum flavum will be bulging then only if the disc height collapses and best way to know it would be to follow a new proposed line (blue line in image above) demarcating a normal relation of lower endplate of vertebra above and SAP of vertebra below in sagittal image of foramen. The line along lower endplate almost always passes just above the tip of SAP. Any overriding of SAP in upper foramen can then be detected easily by it appearing above the line in a lateral neutral X-ray. The tip can cause symptoms more in extension; of claudication if its soft tissue cover is hypertrophied in addition to more compression by bulging midline posterior ligamentum flavum. Removal of the midline ligament may then be relevant in cases of disc collapse. The contribution of SAP tip and midline ligament is not quantified yet. The contribution of midline ligamentum flavum is not a well settled cause. The proximity of SAP seems to be anatomically more direct causation. There may be a need to jack up the disc height in a grossly collapsed disc using transforaminal lumbar interbody fusion (TLIF) or similar ideas, that may take care of both SAPs over riding in foramen and indirectly some bulging ligamentum in midline. It is significant to note here, that in TLIF as a treatment in symptomatic patients we do not routinely remove the ligament but stretch it while jacking up the disc. Hence, midline ligamentum flavum physical removal may not be needed and relevant to relief of symptoms.
In open surgery, lower and upper lateral covers of ligamentum flavum indicate us the exiting and traversing roots easily. Techniques have highlighted better results if the ligamentum flavum in interlaminar area is preserved as there are less adhesions and less scarring post operatively. It is also not proven if this central portion really causes the symptoms. Ligamentum width has not been seen to be related to symptoms. Compression of dural sac in the interlaminar area is thought to be causative of symptoms of claudication by some. This is unproven, and this probably has arisen from a wrong imaging of the ligamentum flavum in cross sections of the spine in plane of disc. Routinely, cross sections in lumbar spine MRI are taken in plane of the disc and are not relevant to structures involved in symptom generation. The cross-section in the plane of disc shows the V of lamina and interlaminar ligamentum flavum. If we tilt the gantry angle and make it parallel to facet and ligament, and take a section in plane of facet and ligament then a true anatomy of ligament can be seen and that is now also supported by new fusion MRI and 3D MRI and ventral dissection studies[16][Figure 3].
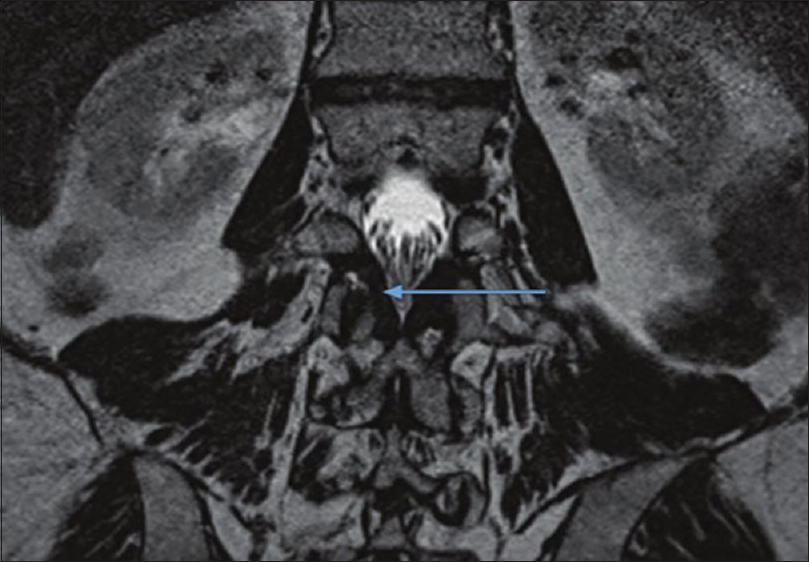
- Coronal oblique image magnetic resonance imaging showing the lateral extent and attachment of ligamentum flavum to upper pedicle in foramen, portion above blue arrow is ligament in roof of foramen
This CORONAL OBLIQUE[14] can show us the real culprit in roof of foramen over lying DRG and axilla. Newer studies on ligament anatomy do support the lateral attachment of ligament is more than 1 cm beyond the medial pedicle line. This can only be assessed by transforaminal access without any midline bone removal.
The popular term bony hypertrophy is a misnomer as after skeletal maturity no bone in human body can grow. This improper use of the term has continued even in today's world as the prime objective in traditional surgery has been to “cut and remove” bone to decompress. The location of DRG is such that routine access from posterior midline cannot reach that area unless pars or more of medial facet is removed. Many times bone cutting results in instability and may beget more stabilization surgery and use of implants. Use of implants in stabilization for stenosis is unproven. Degenerating spine by its very nature is auto stabilizing in most patients.
Access and the NEW Concept of Foraminoplasty
There is a fair uncertainty on what works in stenosis surgery.[14] Even over the top posterior midline access does not reach the relevant lateral extension of ligamentum flavum and may be a too morbid access.[15] Our transforaminal access and work in foramen is more relevant to this hypertrophied tissue in roof of foramen as seen in adjoining images [Figure 4]. It is also important anatomical relation that SAP and superior facet is always behind the disc or dorsal to disc. Foraminoplasty is planned on these concepts in gore system, where access to and removal of lateral ligamentum flavum that is lateral to medial pedicle line forming the roof of foramen is more relevant than a midline structure. This is easily removed under vision directly. Figures 4-10 show the access and removal of this ligamentum flavum and soft tissue over SAP tip and between SAP tip and upper pedicle. Surgery is in upper larger part of foramen and is under local anesthesia. Additional neuromonitoring is not needed as patient is awake and aware through out surgery.[17,18]
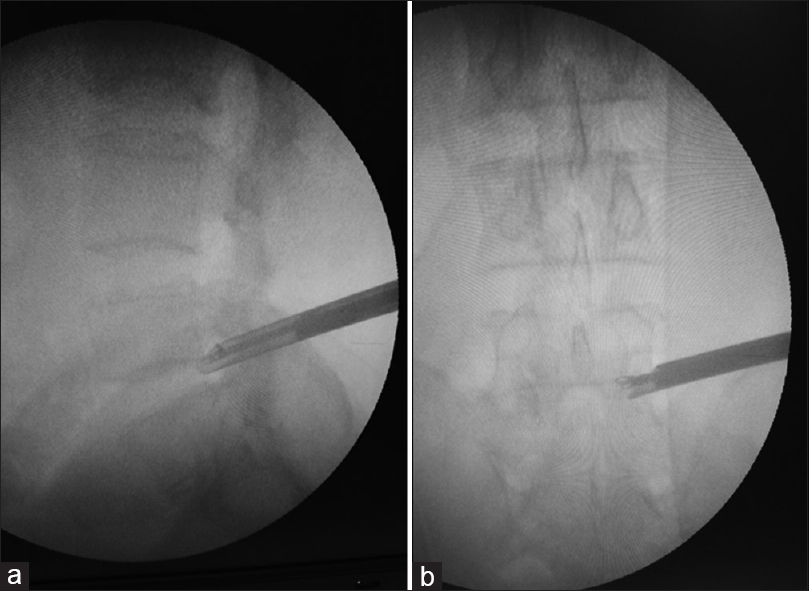
- (a) Intraoperative X-ray showing working in upper foramen on SAP tip. (b) Working in upper foramen, over SAP tip in symptomatic stenosis lateral sagittal image
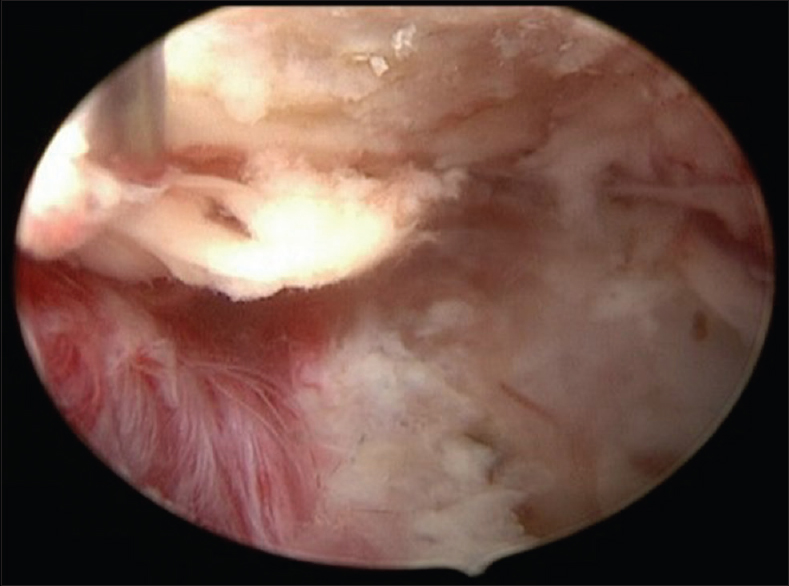
- Use of hook under and over SAP tip to mobilize ligamentum and then remove it

- Use of side fire laser in foramen, red structure below is the exiting nerve
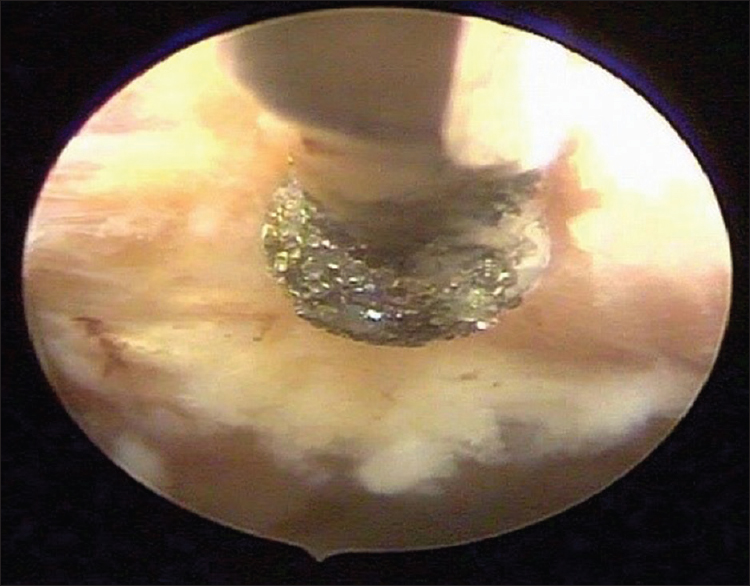
- Use of diamond tip drill to remove hypertrophied soft tissue from the SAP and under surface of superior facet
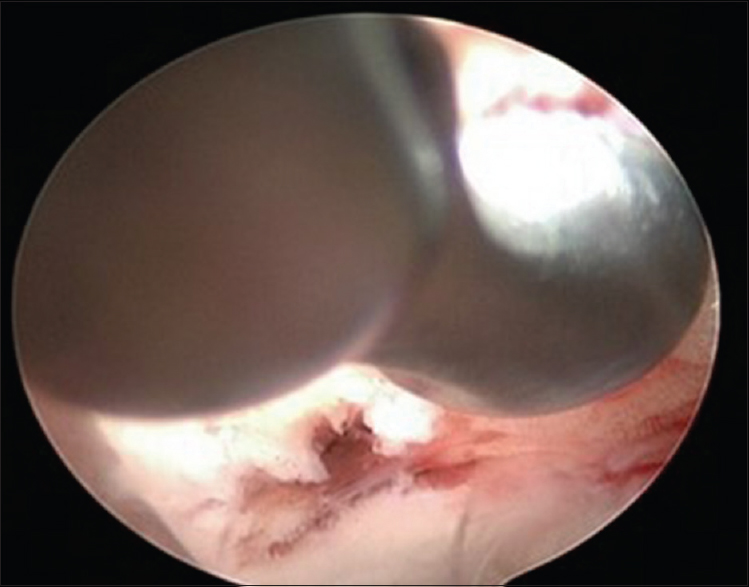
- Use of side curette on facet tip and surface
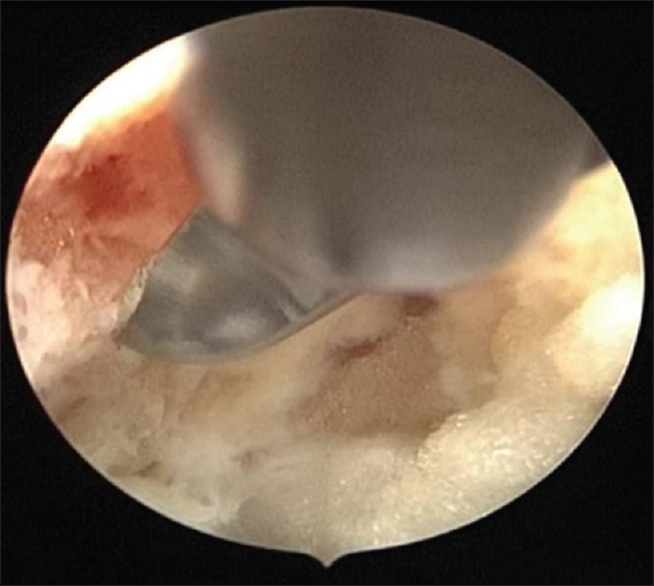
- Use of straight curette under facet and over SAP

- Intraoprative image foraminal view of left L45 with SAP of L5 seen in the right side of the pic.
REFERENCES
- The “Inside Out” Transforaminal Technique to Treat Lumbar Spinal Pain in an Awake and Aware Patient under Local Anesthesia: Results and a Review of the Literature. Available from: http://www.ijssurgery.com/10.14444/1028 (accessed )
- [Google Scholar]
- In-viv o endoscopic visualization of patho-anatomy in symptomatic degenerative conditions of the lumbar spine II: Intradiscal, foraminal, and central canal decompression. Surg Technol Int. 2011;21:299-319.
- [Google Scholar]
- Microdecompression for lumbar spinal canal stenosis. Spine (Phila Pa 1976). 1999;24:2268-72.
- [Google Scholar]
- Outcomes of decompression for lumbar spinal canal stenosis based upon preoperative radiographic severity. J Orthop Surg Res. 2007;2:3..
- [Google Scholar]
- Lumbar spinal stenosis-specific symptom scale: Validity and responsiveness. Spine (Phila Pa 1976). 2014;39:E1388-93.
- [Google Scholar]
- Use of bladder volume measurement assessed with ultrasound to predict postoperative urinary retention. North Clin Istanb. 2016;3:209-16.
- [Google Scholar]
- Postoperative bladder catheterization based on individual bladder capacity: A randomized trial. Anesthesiology. 2015;122:46-54.
- [Google Scholar]
- Clinical correlation of a new MR imaging method for assessing lumbar foraminal stenosis. AJNR Am J Neuroradiol. 2012;33:818-22.
- [Google Scholar]
- Uncertainties in the diagnosis of lumbar spinal stenosis. Radiology. 2011;261:681-4.
- [Google Scholar]
- Anatomical study of lumbar spinal canal diameter on MRI to assess spinal canal stenosis. Int J Anat Res. 2015;3:1441-4.
- [Google Scholar]
- Radiologic criteria for the diagnosis of spinal stenosis: Results of a Delphi Survey. Radiology. 2012;264:174-9.
- [Google Scholar]
- Morphological changes of the ligamentum flavum as a cause of nerve root compression. Eur Spine J. 2005;14:277-86.
- [Google Scholar]
- Anatomical analysis of the relation between human ligamentum flavum and posterior spinal bony prominence. J Orthop Sci. 2017;22:260-5.
- [Google Scholar]
- Lumbar stenosis: Oblique coronal images in MRI for assessment of ligamentum flavum. J Spinal Surg. 2016;3:117..
- [Google Scholar]
- Three-dimensional visualization of ligamentum flavum relative to the affected spinal nerve root by MRI/CT fusion imaging: Three case reports of lumbar radiculopathy and motor palsy. J Pain Manage Med. 2016;2:3..
- [Google Scholar]
- What interventions improve walking ability in neurogenic claudication with lumbar spinal stenosis? A systematic review. Eur Spine J. 2014;23:1282-301.
- [Google Scholar]
- Bilateral “over the top” decompression through unilateral laminotomy for lumbar and thoracic spinal canal stenosis. Ideggyogy Sz. 2007;60:467-73.
- [Google Scholar]




