
Translate this page into:
A study of association between acromion types and shoulder pathology
Address for correspondence: Dr. Prabhu Ethiraj, Department of Orthopaedics, Sri Devaraj Urs Academy of Higher Education and Research (SDUAHER), Kolar, Karnataka, India. E-mail: prabhu.thepreacher@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Venkataraman S, Ethiraj P, Shanthappa AH, Vellingiri K. A study of association between acromion types and shoulder pathology. J Orthop Spine 2022;10:92-5.
Abstract
INTRODUCTION:
Shoulder impingement and rotator cuff tear are commonly seen in shoulder pathology. Pathological changes in the soft tissue around the shoulder can be due to intrinsic degenerative in tendons or extrinsic mechanical compression due to acromion types. Changes in acromion morphology have been postulated, which might be one of the causes of impingement syndrome and rotator cuff tears. But few study results have shown that role of the acromion is doubtful. Our primary objective was to determine acromion types and their prevalence rate with shoulder pathology.
MATERIALS AND METHODS:
Our study was a prospective study. Eighty-five patients who met the inclusion criteria were included in the study. According to Bigliani et al., acromion types were classified as type 1 acromion that has a flat undersurface, type 2 acromion that has a curved undersurface, and type 3 acromion that has a hooked undersurface on supraspinatous outlet view radiographs. Types of acromion were correlated with shoulder pathology (shoulder impingement and rotator cuff tear).
RESULTS:
Out of 85 patients with shoulder pathology, 43 patients had impingement shoulder syndrome and 42 patients had rotator cuff tear. Mean age for the impingement shoulder syndrome group was 39.6 years and for the rotator cuff tear group it was 58.6 years. Overall right shoulder is affected more as compared with the left shoulder. Type 2 acromion was seen in 64.7% study population, type 1 was seen in 23.5%, and type 3 was seen in 11.8%.
CONCLUSION:
In our study, type 2 acromion is more frequently seen in shoulder pathology involving rotator cuff tear and impingement syndrome.
Keywords
Acromion types
rotator cuff tear
shoulder impingement syndrome

Introduction
Shoulder joint is one of the important joints in the human body. Shoulder joint is a complex and mobile joint. Acromion process is an important structure around the shoulder. Shoulder impingement and rotator cuff tear are commonly seen in shoulder pathology. Pathological changes can be due to intrinsic degenerative in tendons or extrinsic mechanical compression due to Acromion types. Neer in 1983 stated that 95% of rotator cuff tear is caused by mechanical compression.[1,2] Since then considerable studies[3,4,5,6] are there to define morphological characteristics of acromion based on cadaveric study and radiographs. Subacromion space consists of supraspinatous tendon subacromion bursa. Supraspinatous tendon lies beneath inferior border of acromion. When shoulder is abducted and internally rotated, supraspinatous tendon comes close to inferior border of acromion.[2,7] Acromioplasty is a surgical procedure where part of acromion process which is in contact with the rotator cuff tendon is shaved or removed. The part of acromion process which is in contact with the rotator cuff tendon produces friction during shoulder abduction or rotation movement, thereby producing damage to tendon. Arthroscopic acromioplasty is still a standard procedure done for shoulder impingement pathology and during rotator cuff repair. Bigliani was the first person who described acromion morphology. Changes in acromion morphology have been postulated that might be one of the causes of impingement syndrome and rotator cuff tears. According to Bigliani et al.,[3] acromion is classified as type 1 acromion that has a flat undersurface, type 2 acromion that has curved undersurface, and type 3 acromion that has a hooked undersurface. These acromion types are better appreciated on outlet view radiographs.[3] The association between acromion morphology, shoulder impingement, and rotator cuff pathology has been described in the literature.[1,4] Few of the authors have stated that hook-shaped acromion has a higher prevalence rate with rotator cuff tears and shoulder impingement syndrome.[3,4,8] Few study results showed that acromion morphology varies with aging.[9,10] But results are ambiguous, and the role of the acromion is doubtful. Our study might help in contributing the association between acromion types and shoulder pathology. Our primary objective was to determine acromion types and their prevalence rate with shoulder pathology.
Materials and Methods
The study was conducted in a tertiary referral hospital after obtaining ethical clearance from the institute. This was a prospective study that included cases from January 2019 to December 2019. A total of 85 patients who met the inclusion criteria were included in the study. Patients with shoulder pathology diagnosed based on ultrasound shoulder or magnetic resonance imaging shoulder. Detailed clinical examination and workup were done for the patient diagnosed with shoulder impingement syndrome or rotator cuff tear.
Required radiographs
Supraspinatous outlet view and shoulder anteroposterior view were taken. For the standard anteroposterior view, the patient was made to stand and affected shoulder is at the center and the arm was held in a neutral position elbow extended and forearm supinated; the patient is slightly tilted around 10° toward the affected side so that scapula is parallel to X-ray cassette. For supraspinatous outlet view, affected shoulder was tilted 40°–45° away from X-ray cassette and X-ray beam was passed 10°–15° craniocaudal tangential to the scapula.
According to Bigliani et al.[3] [Figure 1], acromion types were classified as type 1 acromion that has a flat undersurface, type 2 acromion that has a curved undersurface, type 3 acromion that has a hooked undersurface on supraspinatous outlet view radiographs.[3] Types of acromion will be classified based on radiographs and will be correlated with shoulder pathology and age group.
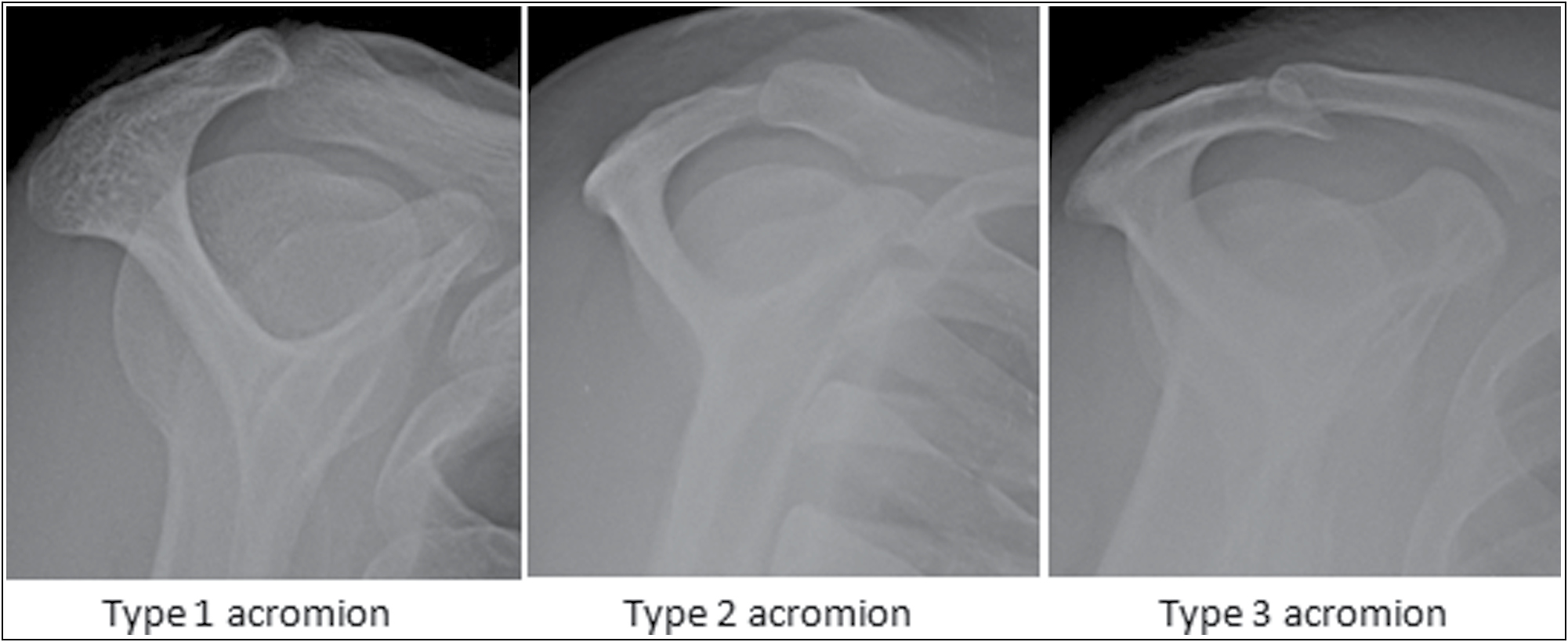
- Three types of acromion X-ray image: (1) type 1––flat, (2) type 2––curved, and (3) type 3––hooked
Inclusion criteria
Patients of age group >20 years.
Patient with shoulder impingement syndrome or rotator cuff tears
Exclusion criteria
Traumatic shoulder pathology
Previous operated shoulder surgery
Infective shoulder pathology.
Tumors involving the shoulder joint.
Statistical analysis
All the data from our study were evaluated by the chi-square test and SPSS software version 22.0 IBM was used. A value of P < 0.05 was considered statistically significant.
Results
The overall distribution is mentioned in Table 1. Out of 85 patients with shoulder pathology, 43 patients had impingement shoulder syndrome and 42 patients had rotator cuff tear [Table 2]. The mean age group for the impingement shoulder syndrome group was 39.6 years and for the rotator cuff tear group it was 58.6 years. Overall right shoulder is affected more as compared with left shoulder. Type 2 acromion was seen in 64.7% study population, type 1 was seen in 23.5%, and type 3 was seen in 11.8%.
| Frequency | % | ||
|---|---|---|---|
| AGE in years | Less than 51 | 43 | 50.6 |
| More than 51 | 42 | 49.4 | |
| Sex | Male | 50 | 58.8 |
| Female | 35 | 41.2 | |
| Affected side | Left | 39 | 45.9 |
| Right | 46 | 54.1 | |
| Dominant hand | Left | 29 | 34.1 |
| Right | 56 | 65.9 | |
| Diagnosis | Impingement syndrome | 43 | 50.6 |
| Rotator cuff tear | 42 | 49.4 | |
| Acromion type | Type 1 | 20 | 23.5 |
| Type 2 | 55 | 64.7 | |
| Type 3 | 10 | 11.8 | |
| Variable Acromion types (according to Bigliani) | Group 1 Impingement | Group 2 Rotator cuff tear |
|---|---|---|
| Type 1 | 12 | 8 |
| Type 2 | 27 | 28 |
| Type 3 | 4 | 6 |
Approximately 53.5% of study participants aged less than 51 years had type 2 acromion and 76.2% of study participants aged more than 51 years had type 2 acromion. However, this association was not statistically significant [Table 3].
| Acromion type | Total | P Value | ||||
|---|---|---|---|---|---|---|
| Type 1 | Type 2 | Type 3 | ||||
| AGE | Less than 51 | 12(279%) | 23(53.5%) | 8(18.6%) | 43 | 0.06 |
| More than 51 | 8(19.0%) | 32(76.2%) | 2(4.8%) | 42 | ||
In our study, the mean age for type 1 acromion is 46.5 years, for type 2 acromion it is 24.8 years, and for type 3 acromion it is 43.1 years.
Discussion
In our study, acromion was classified according to the Bigliani classification. As per Bigliani et al.,[3] acromion was classified depending on the undersurface of the acromion. Type 1 acromion has a flat undersurface, type 2 acromion has a curved undersurface, and type 3 acromion has a hooked undersurface. In our study, overall patients with shoulder pathology had type 2 acromion more in number.
In the shoulder impingement syndrome group, type 1 acromion was seen in 27.9% of patients, type 2 acromion was seen in 62.8%, and type 3 acromion was seen in 9.3%. In the rotator cuff tear group, type 1 acromion was seen in 19%, type 2 acromion 66.7%, and type 3 acromion 14.3%. Our results were compared with Balke et al.,[1] Paraskevas et al.,[11] and Getz et al.,[12] Nicholson et al.[13] studies, where all these study type 2 acromion was more common. In our study population overall, we found type 1 acromion accounted for 23.5%, type 2 acromion was seen in 64.7%, and type 3 acromion was seen in 11.8%.
Balke et al.[1] reported that the mean age group for impingement patients was 49 years and for rotator cuff tear group patients it was 60 years. In our study, mean age group for shoulder impingement was 39.6 years and the mean age group for rotator cuff tear was 58.6 years. Approximately 81% of our study participants aged less than 51 years had impingement and this association between diagnosis and age was found to be statistically significant. Inference shoulder impingement was seen in relatively young individuals around 30–50 years age group, whereas degenerative rotator cuff tear was seen in the older age group 50–70 years.
Balke et al.[1] showed that in both impingement group and rotator tear group male patients are more affected than female patients. In our study population, shoulder impingement syndrome in males are affected more than females whereas in rotator cuff tear females are more than males. Approximately 64% of male participants in our study group had Impingement syndrome and this association between diagnosis and gender was found to be statistically significant.
In our study population, when we considered side affected, in the impingement syndrome group left shoulder was more compared to the right shoulder whereas in rotator cuff tear group right shoulder was more affected than the left shoulder. Therefore, 60.9% of rotator cuff injury was seen on the right side and this association between diagnosis and side was found to be statistically significant.
Some of the studies reported that acromion type varies with the age factor. Wang et al.[9] studied acromion morphology on 272 patients; acromion morphology was determined by Supraspinatous outlet view radiographs. The study showed that there is a significant increase in the number of type 3 acromion in patients aged more than 50 years and also a decrease in the number of type 1 acromion in patients aged more than 50 years. The study concluded that there is a possibility that type 1 acromion may progress to type 2 and then further change to type 3 over time. Speer et al.[10] studied type 3 acromion in young asymptomatic athlete shoulder and results showed that type 3 acromion in the study group was low and concluded that acromion type may change with age. Our study results showed that there was no correlation between acromion type and age. Approximately 53.5% of study participants aged less than 51 years had type 2 acromion and 76.2% of study participants aged more than 51 years had type 2 acromion. However, this association was not statistically significant. The percentage of type 3 acromion in patients aged more than 50 years was less, which again showed that there was no correlation between acromion type and age. Our results compared with studies of Getz et al.,[12] Nicholson et al.,[13] and Vahakari et al.[14] In these studies, there was no correlation between acromion type and age.
Limitation of our study.
Sample size was a small inference drawn from the study and cannot be generalized for the larger population. We included patients who presented to orthopedic outpatient department with shoulder pathology. Therefore, there were no randomization and control groups in our study population to compare acromion types among normal population and shoulder pathology patients.
Conclusion
In our study, type 2 acromion is more frequently seen in shoulder pathology involving rotator cuff tear and impingement syndrome.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Correlation of Acromion morphology with impingement syndrome and rotator cuff tears. Acta Orthop. 2013;84:178-83.
- [CrossRef] [PubMed] [Google Scholar]
- The morphology of the Acromion and its relationship to rotator cuff tears. Orthop Trans. 1986;10:228.
- [Google Scholar]
- The relationship of acromial architecture to rotator cuff disease. Clin Sports Med. 1991;10:823-38.
- [CrossRef] [PubMed] [Google Scholar]
- The relative importance of acromial morphology and age with respect to rotator cuff pathology. J Shoulder Elbow Surg. 2002;11:327-30.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability of radiographic evaluation for acromial morphology. Skeletal Radiol. 1997;26:718-21.
- [CrossRef] [PubMed] [Google Scholar]
- Excision of the acromion in treatment of the supraspinatus syndrome; report of 95 excisions. J Bone Joint Surg Br. 1949;31B:436-42.
- [CrossRef] [Google Scholar]
- Multiplanar analysis of acromion morphology. Am J Sports Med. 1998;26:836-40.
- [CrossRef] [PubMed] [Google Scholar]
- Changes in acromial morphology with age. J Shoulder Elbow Surg. 1997;6:55-9.
- [CrossRef] [PubMed] [Google Scholar]
- Acromial morphotype in the young asymptomatic athletic shoulder. J Shoulder Elbow Surg. 2001;10:434-7.
- [CrossRef] [PubMed] [Google Scholar]
- Acromial morphology: Relation to sex, age, symmetry, and subacromial enthesophytes. Radiology. 1996;199:737-42.
- [CrossRef] [PubMed] [Google Scholar]
- The acromion: Morphologic condition and age related changes. A study of 420 scapulas. J Shoulder Elbow Surg. 1996;5:1-11.
- [CrossRef] [PubMed] [Google Scholar]
- Acromial shape in asymptomatic subjects: A study of 305 shoulders in different age groups. Acta Radiol. 2010;51:202-6.
- [CrossRef] [PubMed] [Google Scholar]




