
Translate this page into:
Functional outcome of intra-articular platelet-rich plasma in periarthritis shoulder
Address for correspondence: Dr. Ajay Kurahatti, Department of Orthopaedics, Sri Devaraj Urs Medical College, Kolar, Karnataka, India. E-mail: ajaykurahatti@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kurahatti A, Arun HS, Hariprasad S, Nagakumar JS. Functional outcome of intra-articular platelet-rich plasma in periarthritis shoulder. J Orthop Spine 2022;10:78-91.
Abstract
BACKGROUND:
The annual incidence of periarthritis shoulder is between 3% and 5% among general population and as high as 20% among individuals with diabetes. A variety of treatment modalities have been advised but best modality of treatment is subjected to debate. Intra-articular injection of platelet-rich plasma (PRP) is an emerging treatment option and its efficacy needs to be examined and hence the study was conducted.
MATERIALS AND METHODS:
This prospective analytical study on 46 cases with frozen shoulder was conducted in the Department of Orthopedics, R L Jalappa Hospital, Kolar. The patients were injected intraarticularly with PRP with posterior approach. Patients were assessed at 3, 6, and 12 weeks. Outcome measures, visual analog scale (VAS) score for pain, and QuickDASH for functional ability were measured.
RESULTS:
Of 46 patients, 21 were men and 25 were women. Mean age of patients was 51 years. Nondominant shoulder was affected in 27 and dominant shoulder in 19 patients. Eleven patients had diabetes mellitus. Mean active abduction improved from the baseline of 65.1° to 133.04°, mean active flexion improved from 82.6° to 147.28°, mean active external rotation improved from 25.3° to 70.02°, and mean active internal rotation improved from 18.91° to 68.58° at the end of 6 weeks’ follow-up. VAS score improved from 6.19 to 1.84 at 12 weeks post-procedure. Functional ability assessed with QuickDASH score showed improvement with successive follow-ups from 81.5 to 22.9. Approximately 52.2% of study patients had excellent results, and 43.5% and 4.3% of patients had good and fair results, respectively.
CONCLUSION:
In this study, single injection of PRP resulted in significant improvement in range of motion of shoulder, pain, and function with long-term effects. Under total aseptic precautions, when performed with a right technique it has no side effects. This study observes that PRP injection is a reliable, productive, efficient, and safe mode of treatment in periarthritis of shoulder.
Keywords
Adhesive capsulitis
frozen shoulder
periarthritis shoulder
platelet-rich plasma (PRP)
quickDASH score
range of motion
visual analog scale

Introduction
Periarthritis (PA) shoulder is characterized by insidious onset, progressive pain, and loss of active and passive mobility in the glenohumeral joint.[1] It usually presents between ages of 40 and 70 years. The annual incidence of PA shoulder is between 3% and 5% among general population and 20% among individuals with diabetes.[1]
The underlying pathology is soft-tissue fibrosis and inflammation of the capsule, ligaments, and rotator interval.[1] PA shoulder is seen most commonly in posttraumatic patients, soft-tissue injury of shoulder patients, and patients with cardiac problems and diabetes.
A broad range of treatment options have been preferred, which include oral nonsteroidal anti-inflammatory drugs (NSAIDS) as well as intra-articular injection of corticosteroids, intra-articular injection of hyaluronic acid, physical therapy exercises, deep heat modalities, manipulation under anesthesia, hydrodilation, arthroscopic release, but the best treatment is still debated.[2] Intra-articular corticosteroid injection is one among commonly used treatment modalities in PA shoulder.
Platelet-rich plasma (PRP) has emerged recently as a new technology which is believed to stimulate re-vascularization of soft tissue and increase the concentration of growth factors to improve and accelerate tendon healing.
PRP is autologous blood with concentration of platelets above baseline values. One million platelets per milliliter of concentrate is the working definition of therapeutic PRP.[3]
PRP is an emerging treatment option and its efficacy needs to be examined and hence the study was conducted.
Materials and Methods
Source of data
This prospective analytical study on 46 cases with frozen shoulder was conducted in the Department of Orthopedics, R L Jalappa Hospital, Kolar on out-patient and in-patient basis, meeting the inclusion and exclusion criteria.
Study period
12 months with patient follow-up at 3, 6, and 12 weeks from November 2017 to October 2018.
Study design
Prospective analytical study.
Sample size
46.
Sample size estimation
Sample size was estimated based on visual analog scale (VAS) scores with an average variance of 1.96 from study done in the year 2017 to detect a difference of 9.5% difference in mean VAS scores with 80% power and with 95% confidence interval, the sample size required is 41 cases. Expecting patient dropout rate of 10% during follow-up, final sample size is estimated as 41 + 5 = 46.[1]
Method of Collection of Data
Inclusion criteria
Patients with PA of shoulder (Shaffer’s criteria was considered).
Aged more than 30 years.
Exclusion criteria
Massive rotator cuff tears
Shoulder instability
Neurological disorders affecting shoulder.
Previous history of any treatment.
Local skin lesions.
Shaffer’s criteria[4]
A minimum of 1 month of shoulder pain and stiffness for which no other cause could be identified.
Documented restriction of passive glenohumeral and scapulothoracic motion of 100° of abduction or less,
Less than 50% of external rotation when compared to the contralateral shoulder.
Patients were screened to find their eligibility to study. Consent was taken and they were included in the study. Patients were selected without consideration of the duration of symptoms, sex of the patient, severity of the disease, whether associated with comorbid conditions such as diabetes, hypertension, and other variables.
Preparation of Platelet-Rich Plasma
PRP was prepared by a process known as differential centrifugation. In differential centrifugation, acceleration force is adjusted to sediment specific cellular constituents depending on different specific gravity.
Under aseptic precautions, 18 mL of the patient’s peripheral whole blood was obtained using an 18-guage needle. Then, 2-mL sodium citrate was added to the collected blood (in ratio of 1:9), and around 2 mL of PRP was extracted by a double-centrifugation technique at 1300 rpm for 10 min to separate erythrocytes and then again at 3500 rpm for 10 min to concentrate platelets using the Rotek Laboratory Centrifuge.[5,6]
Biomechanism of platelet-rich plasma
PRP provides a matrix for the migration of tissue-forming cells, including fibroblasts that are responsible for collagen synthesis and endothelial cells involved in angiogenesis.[7] During normal tissue healing, trapped platelets become activated and degranulate, resulting in the release of the granule content. Alpha granules of the platelets have been shown to contain mitogenic and chemotactic growth factors important in healing such as platelet-derived growth factor (PDGF), transforming growth factor (TGF), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), and insulin-like growth factor (IGF).[8,9,10]
Release of PDGF can have a chemotactic effect on monocytes, neutrophils, fibroblasts, mesenchymal stem cells, and osteoblasts. PDGF is also a powerful mitogen for fibroblasts and smooth muscle cells.[11] TGF is another growth factor released from platelet granules. TGF is a mitogen for fibroblasts, smooth muscle cells, and osteoblasts. In addition, it promotes angiogenesis and extracellular matrix production.[11,12] VEGF promotes angiogenesis and can promote healing and also aid in endochondral ossification. EGF, another platelet contained growth factor, is a mitogen for fibroblasts, endothelial cells and also is useful in healing.[12] IGF, another platelet-contained growth factor, regulates bone maintenance and is also an important modulator of cell apoptosis, and in combination with PDGF, can promote tissue regeneration.[10,13] Platelet concentrates are potentially useful in tissue healing applications because they function as both a tissue sealant and a drug delivery system that contains a host of powerful mitogenic and chemotactic growth factors.
The dense granules of platelets contain adenosine, serotonin, histamine, and calcium. Adenosine is a nucleoside that plays an important role in many biochemical processes, including transfer of energy. Adenosine is a primary cytoprotective agent that prevents tissue damage. Adenosine receptor activation has been shown to have an anti-inflammatory effect during the inflammatory process.[14] Adenosine also has the ability to increase interleukin 10 (IL-10) production by macrophages in some cases.[15] This increase in IL-10 could indicate a change in the character of the macrophage to an anti-inflammatory state. In other instances, it appears that adenosine can function to activate macrophages to produce pro-inflammatory cytokines, IL-1 and IL-18.[16] Serotonin is a monoamine neurotransmitter. This hormone can be exponentially more effective at increasing capillary permeability than even histamine.[17] Serotonin also acts as a chemo-attractant for fibroblasts and increases their proliferation. Interestingly, macrophage cells have receptors that are sensitive to serotonin. Serotonin injected locally into tissue induces an influx of macrophages into that tissue.[18] Serotonin has also been shown to effect macrophages by suppression of interferon-gamma-induced 1a expression at sites of inflammation.[19] Histamine is a biogenic amine involved in local immune responses. Locally, it also acts as a vasodilator. Histamine enhances permeability of the microvascular system of capillaries and venules. This increased permeability is due to the contraction of endothelial cells and removal of fenestrated diaphragms blocking gaps in the endothelial lining.[20] This increase in membrane permeability allows inflammatory and immune cells greater access to marginate and enter the local area. Histamine is also a strong activator of macrophages. Calcium is the final component of the dense granules. Calcium may also be required in cell migration and regeneration in the remodeling phase. The unique combination and concentration of bioactive molecules that exist within PRP have profound effects on the inflammatory, proliferative, and remodeling phases of tissue healing.[21]
Procedure
All the patients got intra-articular injection of PRP. The surgeon injected a single dose of 2 mL of the PRP into the intra-articular area of the shoulder in an aseptic technique. Posterior approach was used, 2 cm below the angle of the acromion and 2 cm medial to it (Mike Walton). The needle was directed anteriorly and medially towards the coracoid process. 2–3 cm depth was reached with a 20-gauge needle (a study by Agirman showed that the mean joint depth was 43.5 mm at posterior and 27.1 mm at anterior side). X-rays and ultrasound were done if necessary [Figure 1].
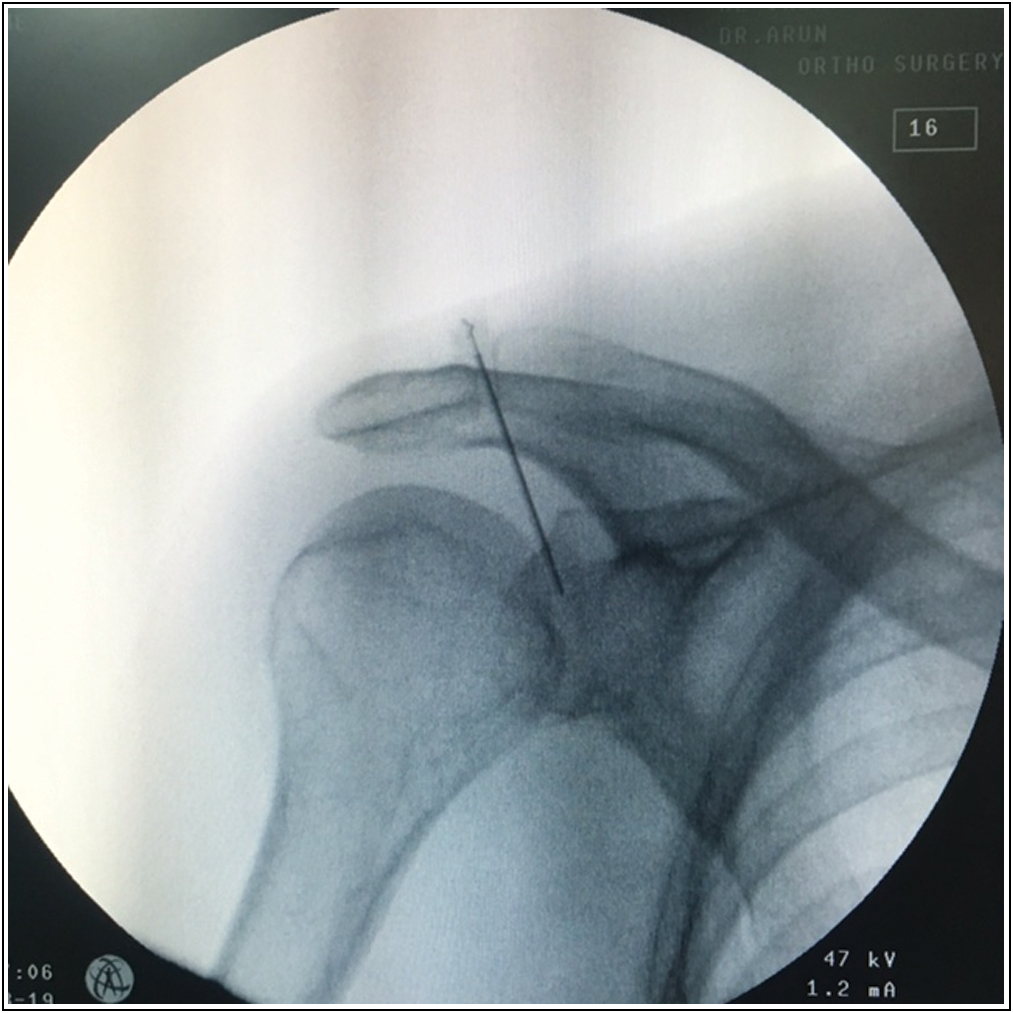
- Intra articular injection of platelet-rich plasma.
Postinjection protocol and rehabilitation
After the PRP injection all the patients were actively mobilized and initial ice pack application was advised for initial 6 h. Codman’s shoulder exercises were advised. For initial pain management paracetamol 500 mg tablets were used as rescue medications. Twelve patients required oral paracetamol for their initial shoulder pain management. Universal shoulder range of movements and exercises were advised for all the patients at their residence. Findings were recorded and outcomes were measured before the injection and during all the follow-ups. Patients were followed up at 3 weeks, 6 weeks and 12 weeks. Outcome measures like active and passive range of motion, visual analogue scale for pain and quickDASH for function were measured.
Results
Of 46 patients, 21 were men and 25 were women. Minimum age of patient included was 30 years and maximum of 80 years. Mean age of patients was 51 years. Nondominant shoulder was affected in 27 patients and dominant shoulder in 19 patients. Eleven patients had diabetes mellitus [Table 1]. Mean active abduction improved from the baseline of 65.1° to 133.04° [Figure 2], mean active flexion improved from the baseline of 82.6° to 147.28° [Figure 3], mean active external rotation improved from the baseline of 25° to 70.02° [Figures 4 and 5], mean active internal rotation improved from the baseline of 18.91° to 68.58° [Figures 6 and 7] at the end of 6 weeks follow-up. VAS score improved from 6.19 to 1.84 at 12 weeks post procedure. Functional ability, assessed with Quick DASH score showed improvement with successive follow-ups from 81.5 to 22.9. 52.2% of study patients had excellent results, 43.5% and 4.3% of patients had good and fair results, respectively [Table 2]. None had poor results. We also have followed up 41 patients till 1 year. These patients showed a similar functional outcome even at the end of 1 year follow-up. Remaining five patients could not complete the follow-up up to 1 year because four patients could not be contacted and one patient expired. Of the 46 patients, seven patients had recurrence of symptoms of which four patients had an average of VAS score of 5.6 and an average quickDASH score of 55.6 and remaining three patients had an average of VAS scores of 4.8 and an average quickDASH score of 43.6 which were managed by conservative management and physiotherapy and the patients improved at later follow-up.
| Study | Kothari et al.[1] | Sharma et al.[22] | Pushpasekaran et al.[25] | Robert et al.[23] | This study |
|---|---|---|---|---|---|
| Mean age (years) | 51.9 | 52 | 56.4 | 52 | 51.19 |
| Sex | Male | Female | Female | Female | Female |
| % | 64.83 | 58 | 72.1 | 76.6 | 54.35 |
| Dominant shoulder | 58.1% | 52% | 30.3% | - | 31.31% |
| Non dominant shoulder | 41.9% | 48% | 69.7% | - | 58.69% |
| Diabetic | - | - | 6.97% | 15% | 23.9% |
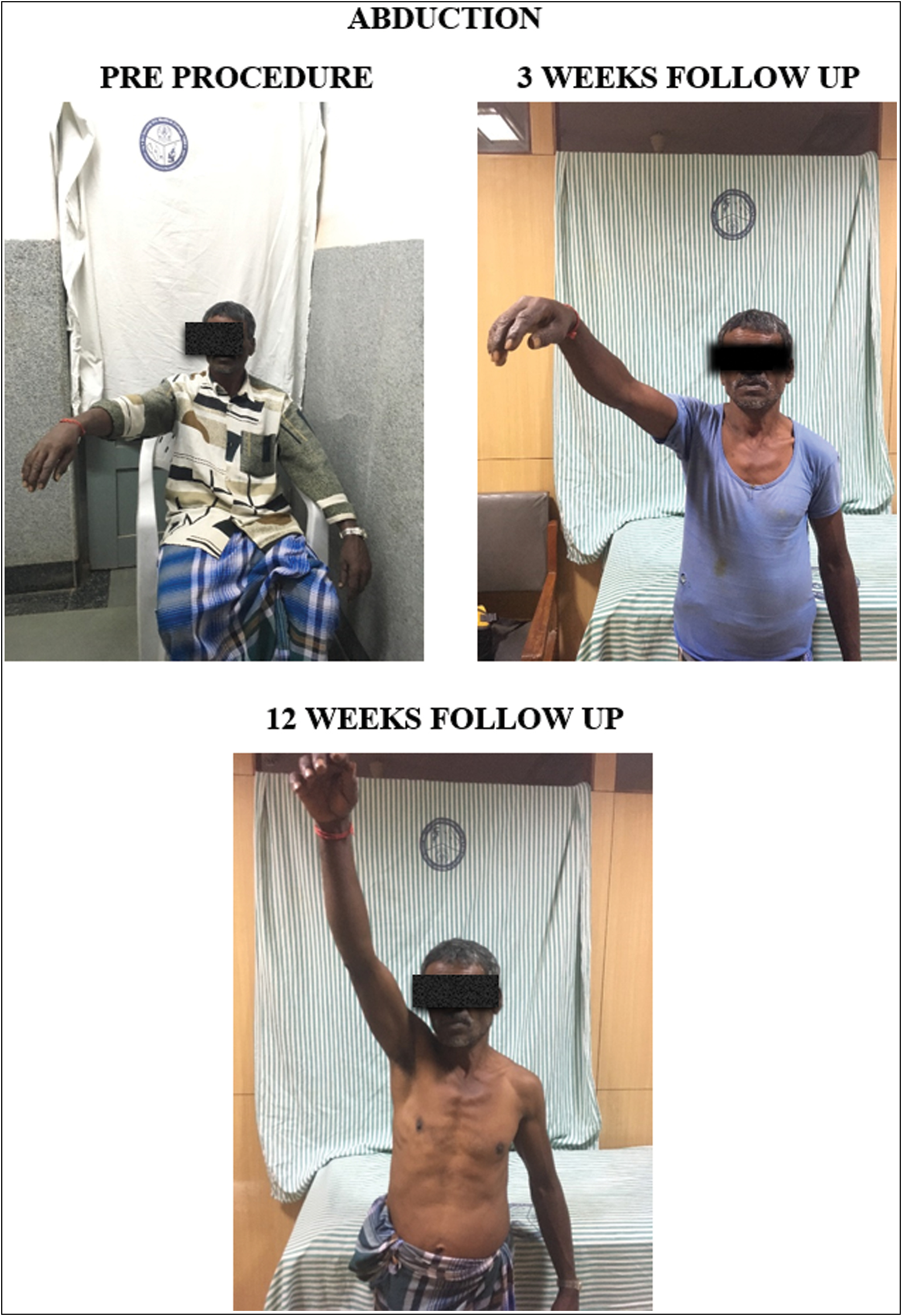
- Abduction: pre-procedure, 3-week follow-up, and 12-week follow-up
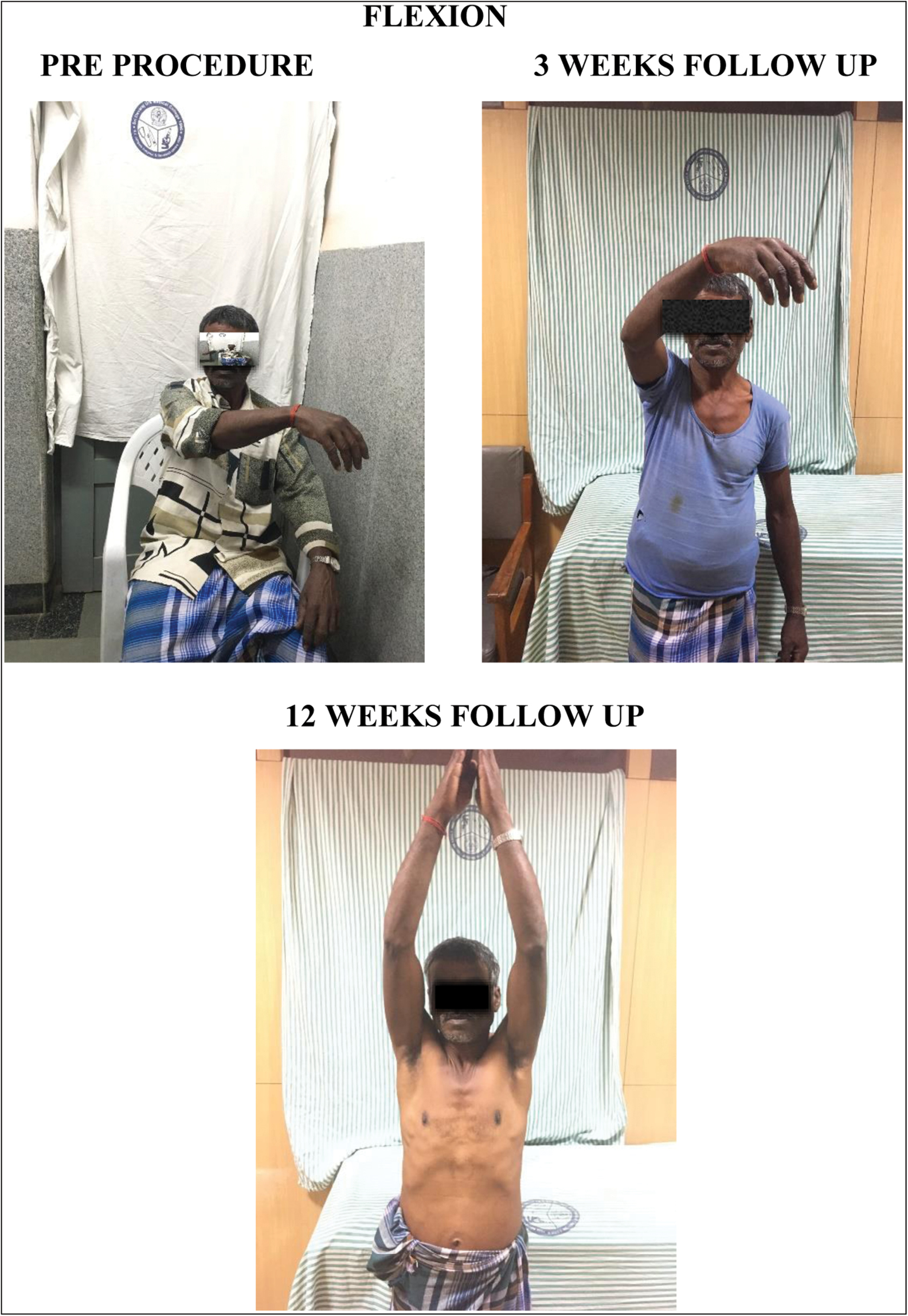
- Flexion: pre-procedure, 3-week follow-up, and 12-week follow-up
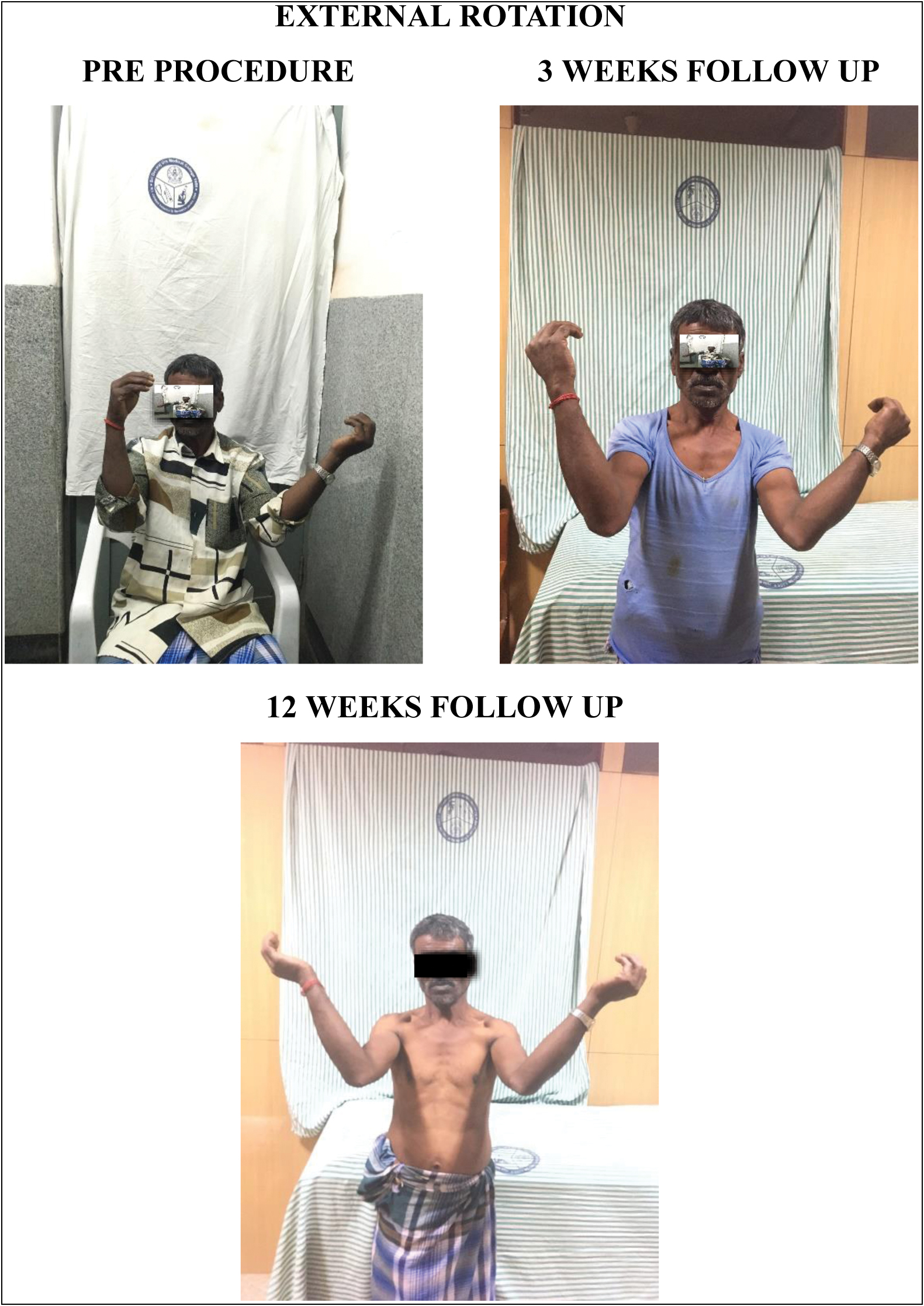
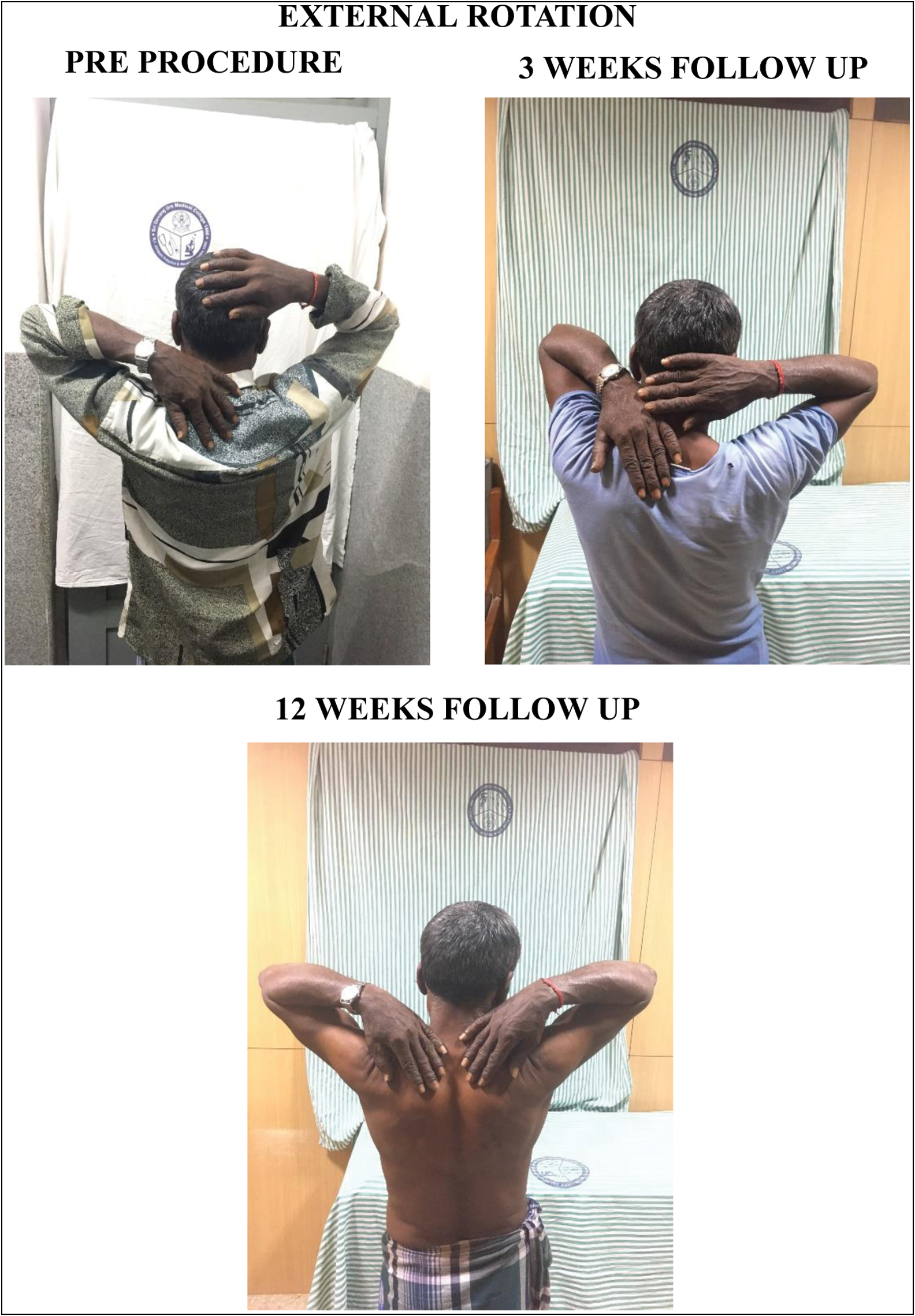
- External rotation: pre-procedure, 3-week follow-up, and 12-week follow-up
- External rotation: pre-procedure, 3-week follow-up, and 12-week follow-up
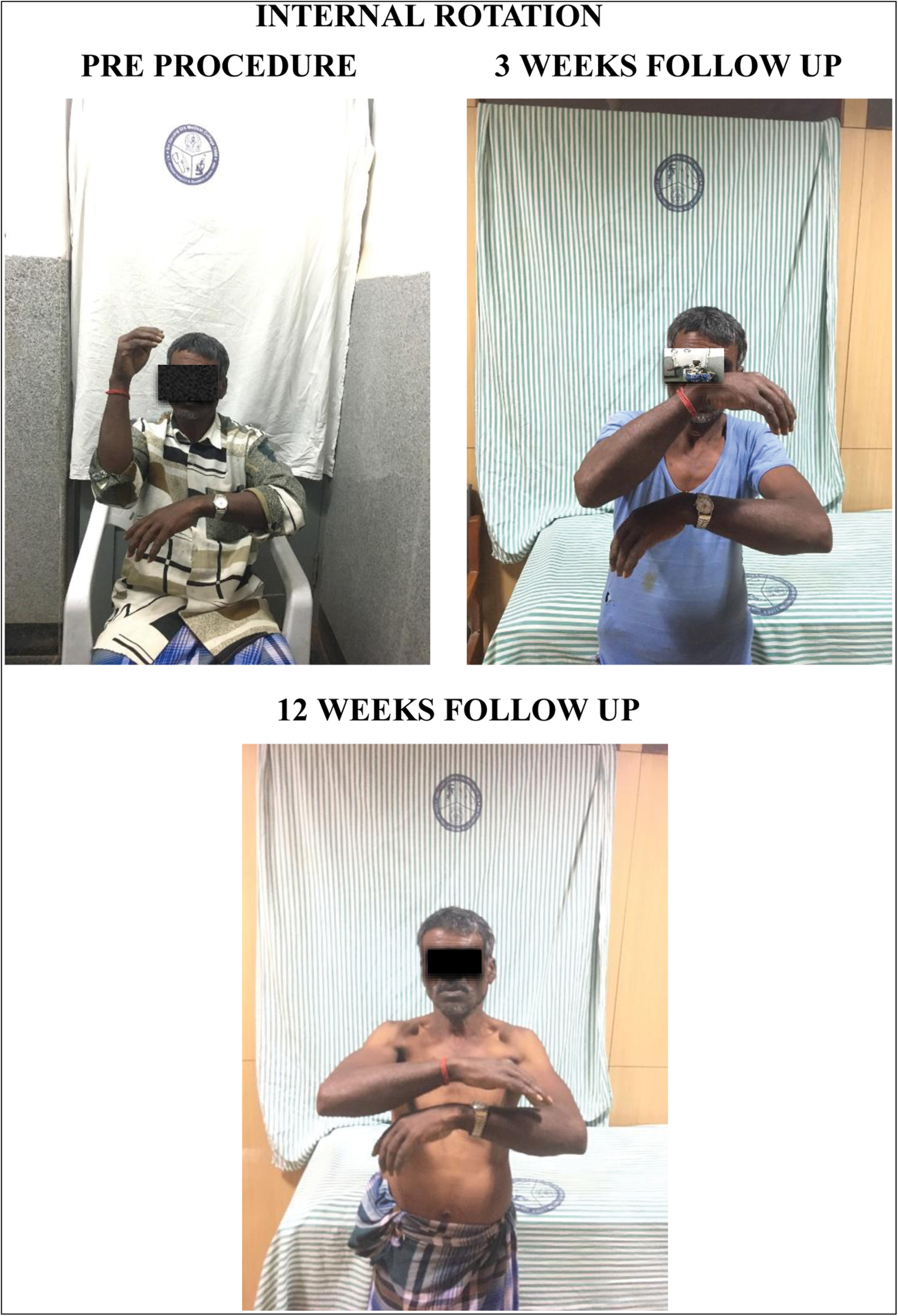
- Internal rotation: pre-procedure, 3-week follow-up, and 12-week follow-up
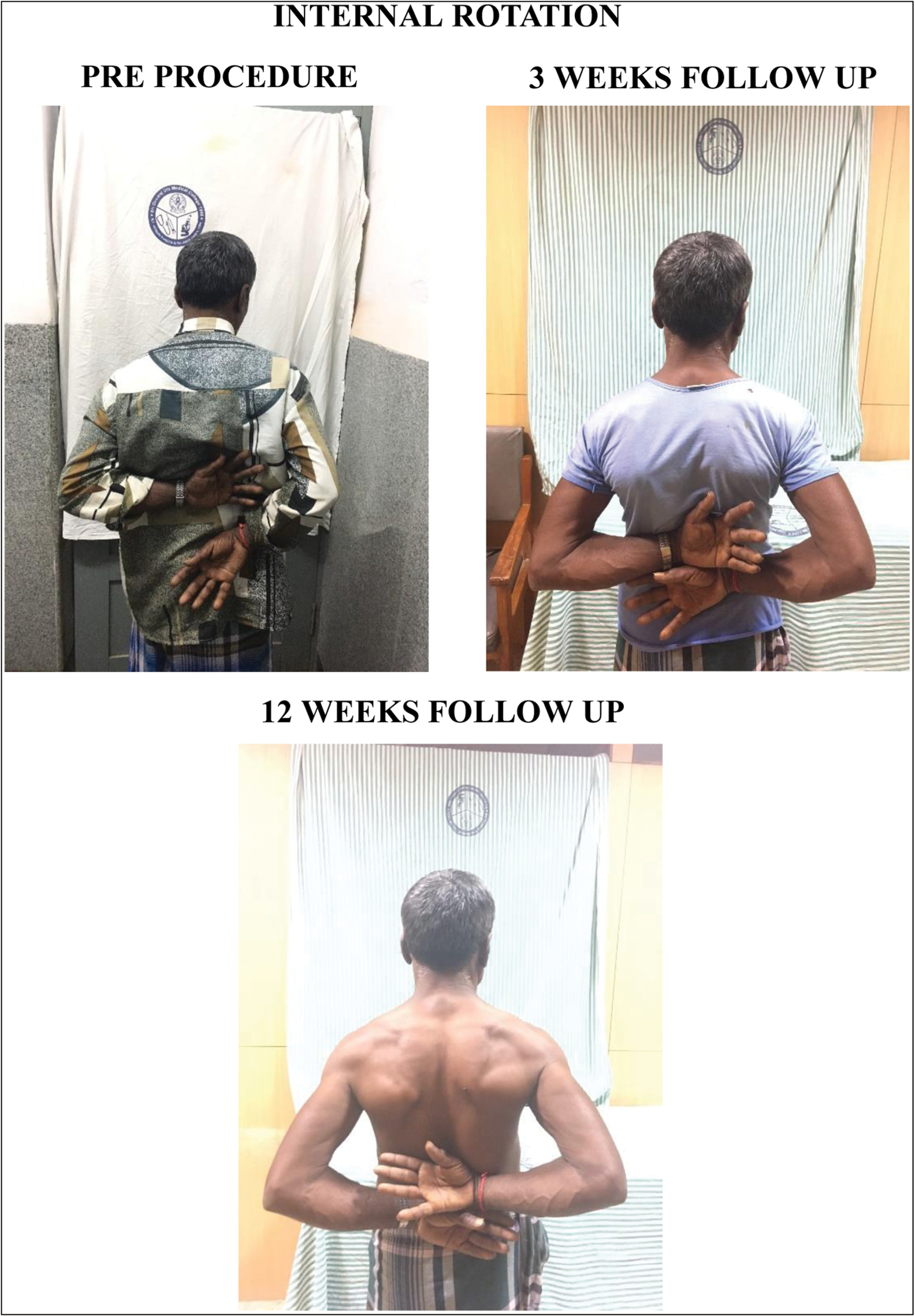
- Internal rotation: pre-procedure, 3-week follow-up, and 12-week follow-up
Discussion
In this study, a descriptive term “Periarthritis Shoulder” is used to describe a clinical syndrome where the patient has a minimum of 1 month of shoulder pain and stiffness for which no other cause could be identified, documented restriction of passive glenohumeral and scapula-thoracic motion of 100° of abduction or less, and less than 50% of external rotation when compared to the contralateral shoulder.
Age incidence
In this study, the average age documented was 51.19 years which was similar to findings of studies conducted by Kothari et al.,[1] Sharma et al.,[22] Robert et al.[23] 33 of the 46 cases were in 5th and 6th decade. It was observed that frozen shoulder was common in fifth and sixth decades of life. R.J. Neviaser and T.J. Neviaser have noted that frozen shoulder is very commonly affected the patients between the age group of 40 and 60 years.[24]
Sex incidence
The female-to-male ratio in this study is 1.20:1. Most authors have documented female preponderance. Kothari et al.[1] recorded a male preponderance.
Side affected
In our study, the nondominant shoulder was most commonly involved with involvement 58.69% of patients showing similar findings with studies by Robert et al.,[23] Sharma et al.[22] and Pushpakaran et al.[25] Most authors have concluded that there is significant difference in the involvement of dominant arm and non-dominant arm.[26]
Associated diseases
It was observed that association of diabetes mellitus is very common, particularly in insulin dependent diabetes mellitus.[26,27] Eleven cases of diabetes mellitus were identified in this study and these were non-insulin dependent and were under control. Four cases were hypertensive and under treatment. We noticed two cases of bronchial Asthma. We did not notice any thyroid disorders in this study.
Treatment of frozen shoulder
All the patients were managed with intra articular PRP injection. The procedure was well tolerated by the patients. Almost all the patients had severe pain and disturbed sleep before treatment. Diffuse shoulder pain particularly during rotational movements was noticed. Tenderness over the glenohumeral joint was present in majority of the patients. Thirty patients of 46 patients were previously treated with oral NSAID but without much relief. The pain relief was observed at 3 weeks and further improvement observed at consecutive follow-ups.
Range of motion
Active abduction [Figure 8]
Mean active abduction improved from the baseline of 65.1° to 133.04° in this study, whereas in study conducted by Kothari et al.,[1] mean active abduction improved from the baseline of 90.1° to 142.3° at the end of the follow-up.
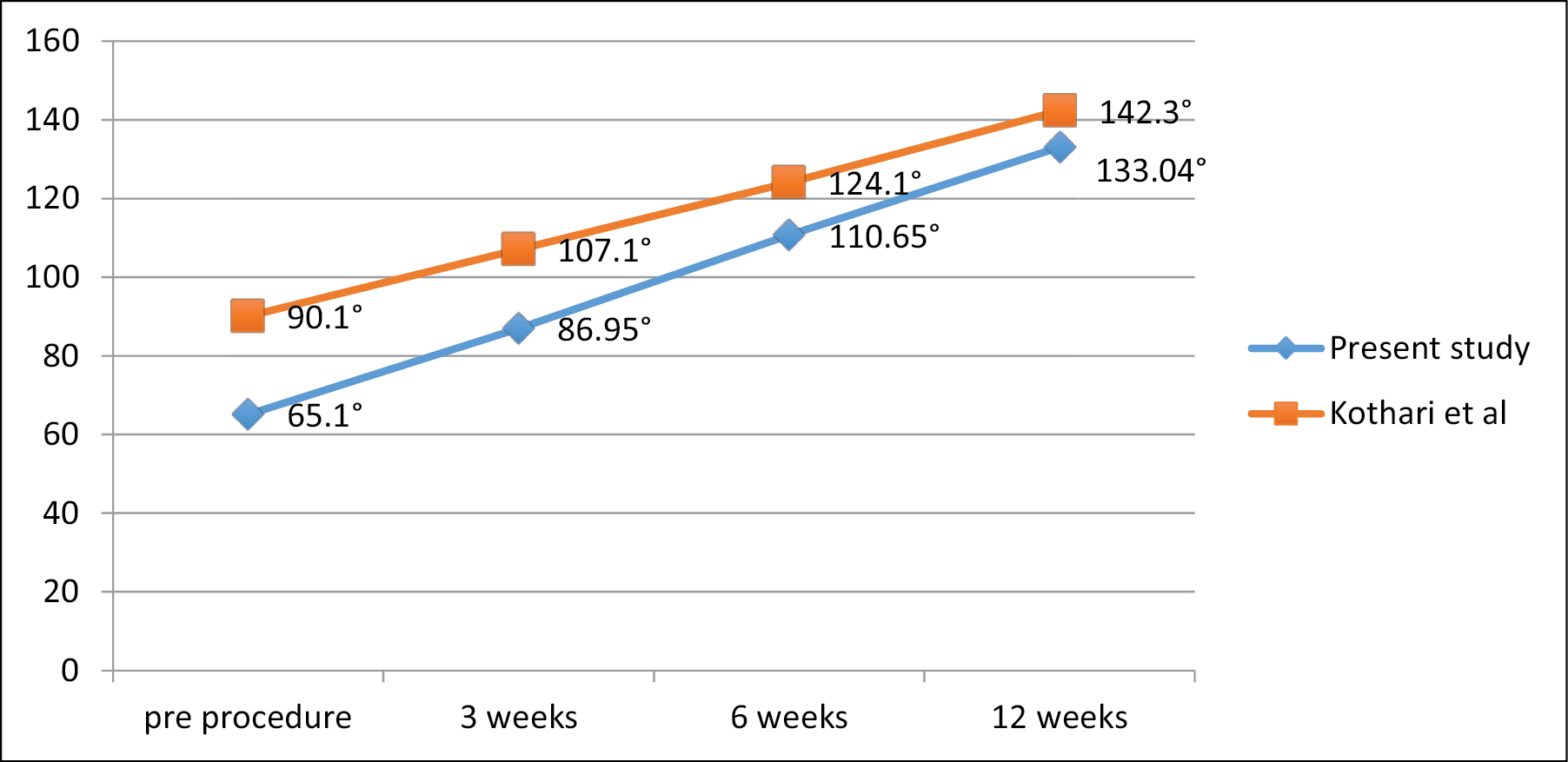
- Active abduction
Active flexion [Figure 9]
Mean active flexion improved from the baseline of 82.6° to 147.28° in this study, whereas in study conducted by Kothari et al.,[1] mean active flexion improved from the baseline of 95.5° to 145.5° at the end of the follow-up.
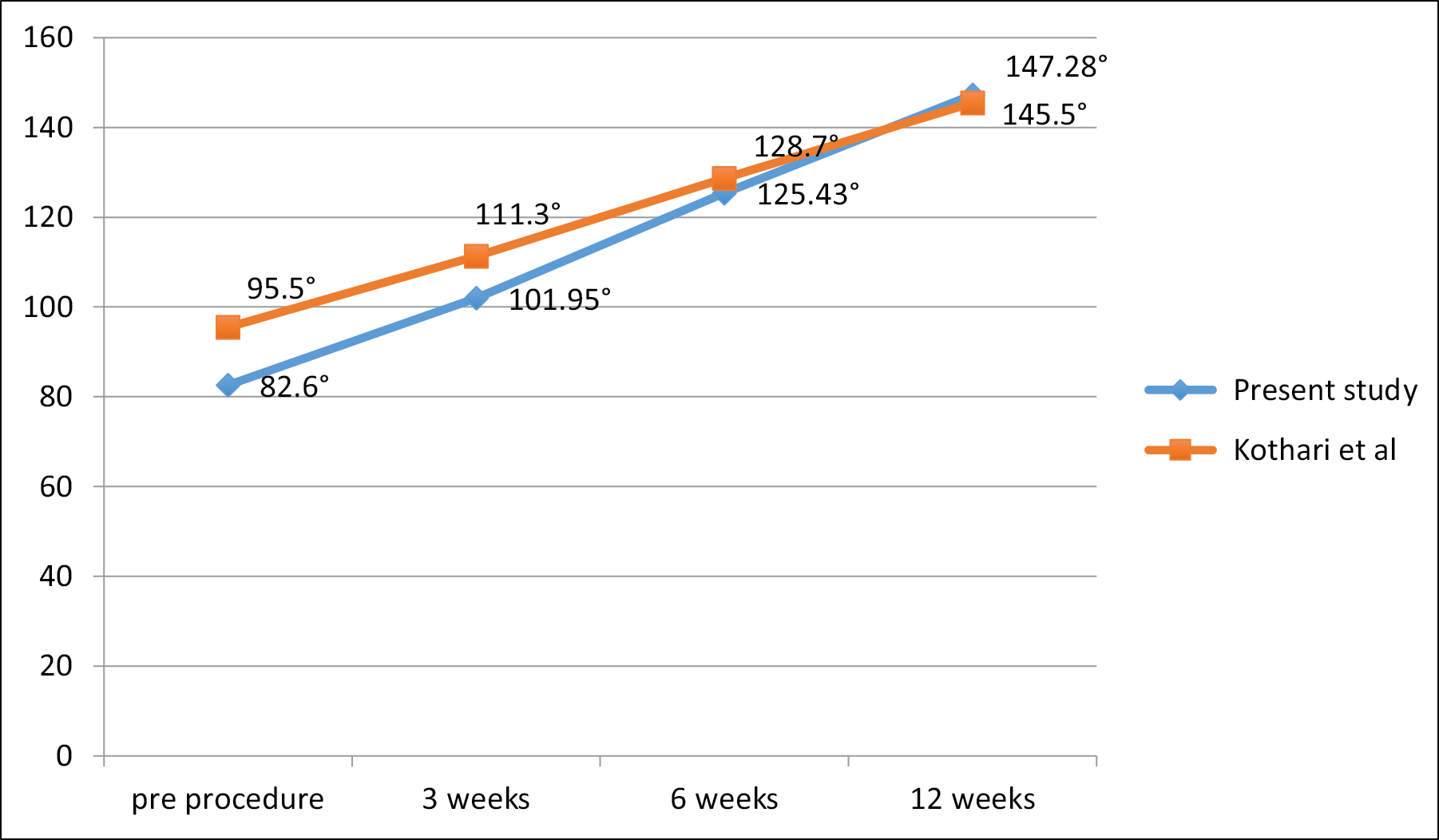
- Active flexion
Active external rotation [Figure 10]
Mean active external rotation improved from the baseline of 25° to 70.02° in this study, whereas in study conducted by Kothari et al.,[1] mean active external rotation improved from the baseline of 34.5° to 80.2° at the end of the follow-up.
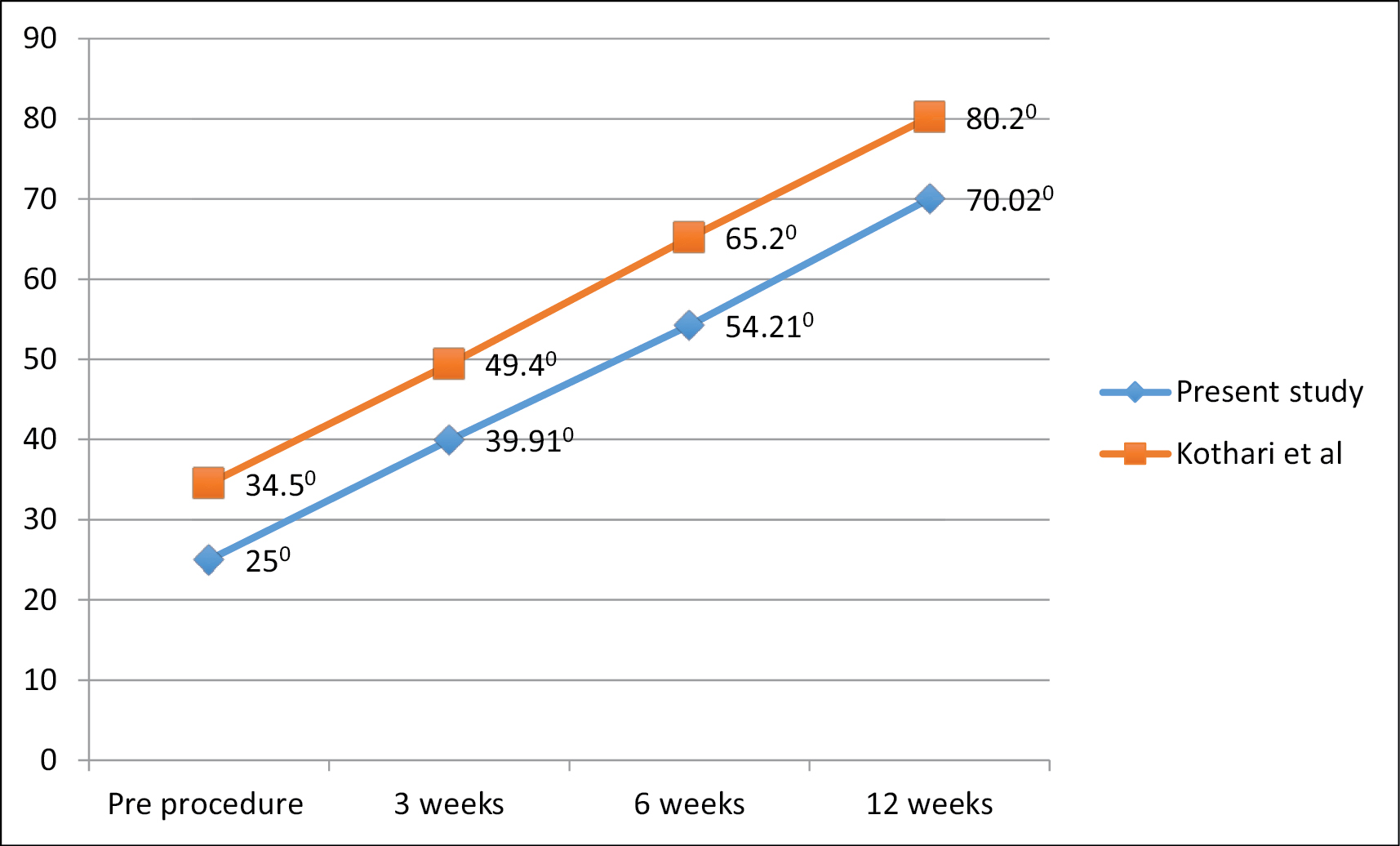
- Active external rotation
Active internal rotation [Figure 11]
Mean active internal rotation improved from the baseline of 18.91° to 68.58° in this study, whereas in study conducted by Kothari et al.,[1] mean active internal rotation improved from the baseline of 21.9° to 57.5° at the end of the follow-up.
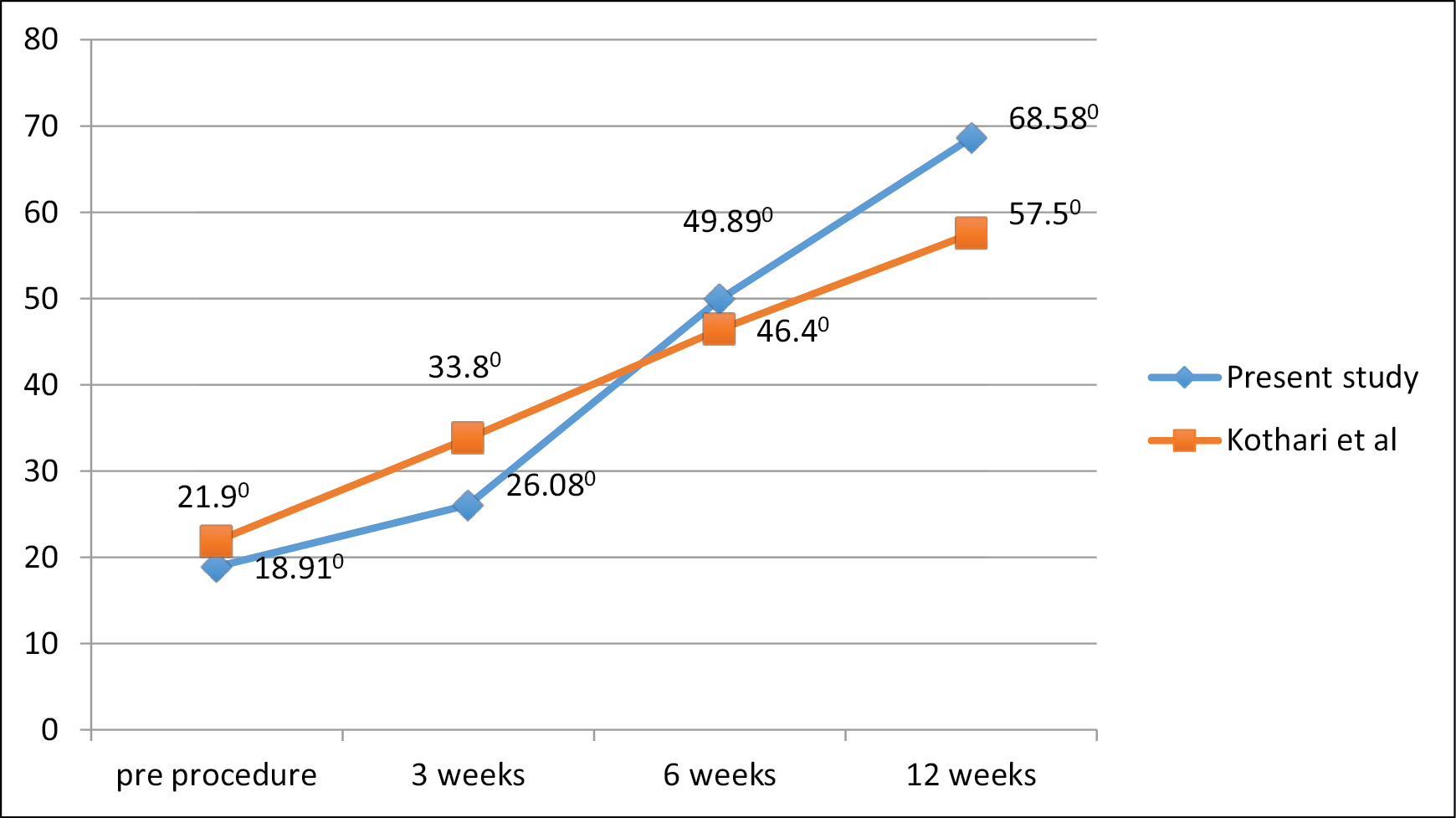
- Active internal rotation
Pain score: VAS score [Table 3 and Figure 12]
VAS score improved from 6.19 to 1.84 within 12 weeks post procedure. This was superior to findings of Kothari et al.[1] 30 and Ahn et al.[28] where final score was 1.9.
| Authors | Baseline | 3 weeks | 6 weeks | 12 weeks |
|---|---|---|---|---|
| Kothari et al.[1] | 8.4 | 6.4 | 4.2 | 1.9 |
| This study | 6.19 | 4.84 | 3.37 | 1.84 |
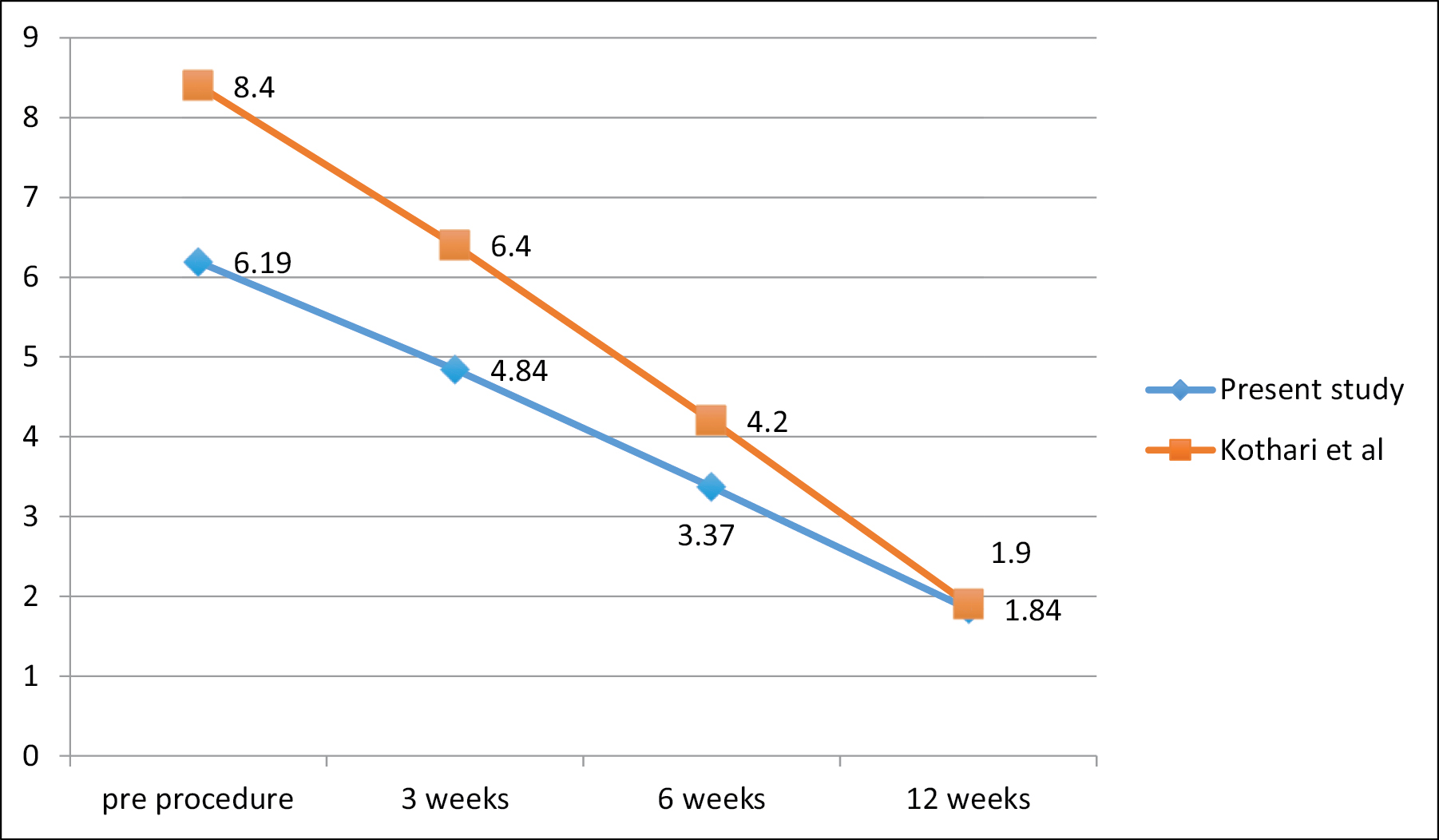
- VAS score graph
The decrease in the mean VAS score of the patients in this study is 1.35(21.8%) from baseline to 3 weeks, 1.47(30.4%) from 3 weeks to 6 weeks, 1.53(45.4%) from 6 weeks to 12 weeks. The reduction of pain is slower initially, and progressively reduces more at 6-week and 12-week follow-up. The decrease in the mean VAS score of the patients in Kothari et al.[1] study is 2(23.8%) from baseline to 3 weeks, is 2.2(34.3%) from 3 weeks to 6 weeks, is 2.3(54.7%) from 6 weeks to 12 weeks. And also progressive reduction of pain of patients in each follow-up in our study is similar compared to those in Kothari et al.[1]
Functional ability score: QuickDASH score [Table 4 and Figure 13]
Functional ability was assessed with QuickDASH scoring showed improvement with successive follow-ups from 81.5 to 22.9. This was comparable to QuickDASH score of study by Kothari et al.[1]
| Authors | Baseline | 3 weeks | 6 weeks | 12 weeks |
|---|---|---|---|---|
| Kothari et al.[1] | 83.5 | 63.7 | 41.6 | 18.7 |
| This study | 81.5 | 60.2 | 40.8 | 22.9 |
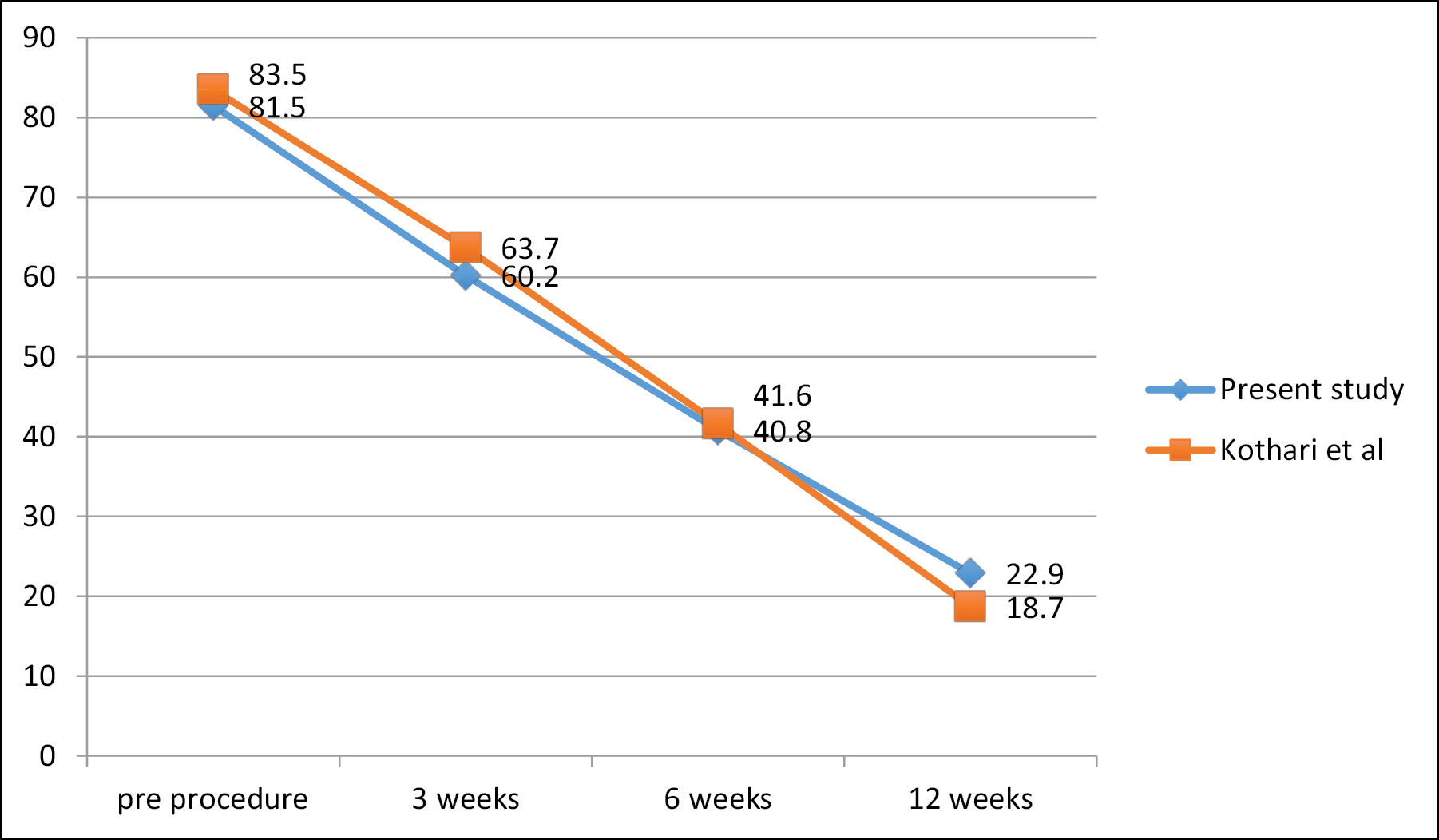
- QuickDASH score graph
The decrease in the mean QuickDASH score of the patients in this study is 21.3(26.1%) from baseline to 3 weeks, 19.4 (32.2%) from 3 weeks to 6 weeks, 17.9(43.9%) from 6 weeks to 12 weeks. The improvement in functional ability progressively increased in each follow-up until 12 weeks. The decrease in the mean QuickDASH score of the patients in Kothari et al.[1] study is 19.8(23.7%) from baseline to 3 weeks, is 22.1(34.7%) from 3 weeks to 6 weeks, is 22.9(55%) from 6 weeks to 12 weeks. Also progressive improvement of functional ability of patients in each follow-up in our study is similar compared to those in Kothari et al.[1]
Conclusion
Aim of this study is to evaluate the outcome of PA shoulder with intra-articular injection of PRP. PA shoulder is not an uncommon condition in the rural population. It is a common cause of shoulder pain and restricted movement. In spite of being treated for over a hundred years, the definition, diagnosis, pathology and most efficacious treatments are still largely unclear.
Though many other methods of treatment have been tried, beginning from conservative methods like analgesics, ROM exercises to use of intra-articular or oral steroids, hydraulic-distension of joint, pain and shoulder stiffness are still haunting the patients as well as orthopedic surgeons.
We treated 46 patients with PA shoulder using intra articular injection of PRP. There were 21 men and 25 were women with maximum age of 80 years and minimum of 30 years with mean of 51 years. Non dominant shoulder was affected in 58.69% of patients. 23.91% of patients were diabetic, 8.69% hypertensive and 4.34% patients have bronchial asthma. The study reflects the increasing importance of PRP in treatment of PA shoulder, especially when steroids are contraindicated in such patients.
Concomitant home exercises program along with intra articular PRP injection was found to be beneficial for PA shoulder.
In this study, single injection of PRP resulted in significant improvement in range of motion of shoulder, pain and function. Under total aseptic precautions, when performed with a right technique it has no side effects.
In this study we observed that intra articular PRP injection is a safe, reliable, cost effective procedure in the management of PA shoulder.
Limitations of study
Though it is a prospective study, the study was done for a shorter duration of time and with limited sample size.
The intra-articular injection of the PRP was given based on the clinical examination which is also a limitation of this study as better imaging modalities could be used to confirm the position of the needle.
The diagnosis of PA shoulder is essentially a clinical diagnosis and it is a diagnosis of exclusion rather than confirmation unlike other painful conditions of the shoulder. This itself is a limitation to the study and a future diagnostic investigative modality for confirmation of this diagnosis could overcome this limitation.
Human subjects
Consent was obtained by all participants in this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Not applicable.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Comparative efficacy of platelet-rich plasma injection, corticosteroid injection and ultrasonic therapy in the treatment of periarthritis shoulder. J Clin Diagn Res. 2017;11:RC15-8.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of ultrasonic therapy, sodium [7] hyaluronate injection and steroid injection in the treatment of periarthritis shoulder. IJPMR. 2012;23:105-10.
- [CrossRef] [Google Scholar]
- Principles and methods of preparation of platelet-rich plasma: A review and author’s perspective. J Cutan Aesthet Surg. 2014;7:189-97.
- [CrossRef] [PubMed] [Google Scholar]
- Frozen shoulder. A long-term follow-up. J Bone Joint Surg Am. 1992;74:738-46.
- [CrossRef] [PubMed] [Google Scholar]
- A cost-effective method for obtaining standard platelet-rich plasma. Wounds. 2014;26:232-8.
- [Google Scholar]
- Local injection of autologous platelet-rich plasma in treatment of lateral epicondylitis and plantar fascitis: Randomised clinical trial. Egypt Rheumatoid. 2012;34:43-9.
- [CrossRef] [Google Scholar]
- Wound healing and inflammatory response to biomaterials. In: Chu CC, von Fraunhofer JA, Greisler HP, eds. Wound Healing Closure and Devices. Boca Raton, FL: CRC Press; 1997. p. :7-24.
- [CrossRef] [Google Scholar]
- Involvement of platelets in stimulating osteogenic activity. J Orthop Res. 1995;13:655-63.
- [CrossRef] [PubMed] [Google Scholar]
- Preparation of Growth Factor Enriched Autologous Platelet Gel. In: Presented at the 27th Annual Meeting of the Society for Biomaterials. 2001.
- [Google Scholar]
- Insulin-like growth factor binding protein-3 is present in the alpha-granules of platelets. Endocrinology. 1993;132:996-1001.
- [CrossRef] [PubMed] [Google Scholar]
- Wound healing: The role of platelet-derived growth factor and transforming growth factor beta. Vet Surg. 1993;22:490.
- [CrossRef] [PubMed] [Google Scholar]
- Growth factors in the treatment of diabetic foot ulcers. Br J Surg. 2003;90:133-46.
- [CrossRef] [PubMed] [Google Scholar]
- Bone growth factors in maxillofacial skeletal reconstruction. Int J Oral Maxillofac Surg. 2002;31:469-84.
- [CrossRef] [PubMed] [Google Scholar]
- Selective sphingosine 1-phosphate 1 receptor activation reduces ischemia-reperfusion injury in mouse kidney. Am J Physiol Renal Physiol. 2006;290:F1516-24.
- [CrossRef] [PubMed] [Google Scholar]
- Adenosine augments Il-10 production by macrophages through an A2b receptor-mediated posttranscriptional mechanism. J Immunol. 2005;175:8260-70.
- [CrossRef] [PubMed] [Google Scholar]
- Atp activates a reactive oxygen species-dependent oxidative stress response and secretion of proinflammatory cytokines in macrophages. J Biol Chem. 2007;282:2871-9.
- [CrossRef] [PubMed] [Google Scholar]
- Release of 5-hydroxytryptamine and histamine from tissues of the rat. J Physiol. 1957;137:179-92.
- [CrossRef] [PubMed] [Google Scholar]
- Macrophage infiltration in tumors and tumor-surrounding tissue: Influence of serotonin and sensitized lymphocytes. Cancer Immunol Immunother. 1988;26:145-52.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of serotonin on murine macrophages: Suppression of Ia expression by serotonin and its reversal by 5-Ht2 serotonergic receptor antagonists. J Immunol. 1986;137:276-82.
- [CrossRef] [PubMed] [Google Scholar]
- On the mechanism of vascular leakage caused by histaminetype mediators: A microscopic study in vivo. Circ Res. 1967;21:833-47.
- [CrossRef] [PubMed] [Google Scholar]
- Calcium: A potential central regulator in wound healing in the skin. Wound Repair Regen. 2002;10:271-85.
- [CrossRef] [PubMed] [Google Scholar]
- Adhesive capsulitis of the shoulder, treatment with corticosteroid, corticosteroid with distension or treatment-as-usual: A randomised controlled trial in primary care. BMC Musculoskelet Disord. 2016;17:232.
- [CrossRef] [PubMed] [Google Scholar]
- Intra-articular corticosteroid injection for the treatment of idiopathic adhesive capsulitis of the shoulder. Hss J. 2007;3:202-7.
- [CrossRef] [PubMed] [Google Scholar]
- 3rd, Kirby RM Office evaluation and management of shoulder pain. Orthop Clin North Am. 1982;13:453-75.
- [CrossRef] [PubMed] [Google Scholar]
- Thawing frozen shoulder by steroid injection: An evaluation and comparative study between a novel three-site injection and single-site. J Orthop Surg. 2017;25:1-5.
- [CrossRef] [PubMed] [Google Scholar]
- The frozen shoulder diagnosis and management. Clin Orthop Relat Res. 1987;223:59-64.
- [CrossRef] [Google Scholar]
- Chapter 21: Frozen shoulder. In: Rockwood CA Jr, ed. The Shoulder. Vol 2. Philadelphia, PA: W.B. Saunders Company; 1990. p. :837-62.
- [Google Scholar]
- Early intra-articular corticosteroid injection improves pain and function in adhesive capsulitis of the shoulder: 1-year retrospective longitudinal study. Pm R. 2018;10:19-27.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of corticosteroid injection in adhesive capsulitis. Clin Rehabil. 2008;22:503-12.
- [CrossRef] [PubMed] [Google Scholar]
- Nonoperative management of adhesive capsulitis of the shoulder: Oral cortisone application versus intra-articular cortisone injections. J Shoulder Elbow Surg. 2010;19:172-9.
- [CrossRef] [PubMed] [Google Scholar]




