
Translate this page into:
Changes in sagittal spinal alignment and pelvic parameters in patients undergoing a total hip arthroplasty
Address for correspondence: Dr. Yoji Ogura, Norton Leatherman Spine Center, 210 East Gray Street, Suite 900, Louisville, KY 40202, USA. E-mail: yojitotti1223@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Ogura Y, Dimar JR, Djurasovic M, Glassman SD, Carreon LY. Changes in sagittal spinal alignment and pelvic parameters in patients undergoing a total hip arthroplasty. J Orthop Spine 2022;10:63-8.
Abstract
BACKGROUND:
The relationship of the spine to the pelvis has been widely studied. However, the role of the hip joint in maintaining sagittal balance remains poorly understood. We aimed to examine if radiographic sagittal spine and pelvic parameters change after Total Hip Arthroplasty (THA), and to evaluate the postural effects on these parameters in standing, sitting, and supine positions.
MATERIALS AND METHODS:
36-inch anteroposterior and lateral standing, sitting and supine radiographs in patients undergoing a unilateral THA pre and post THA were obtained. Standard pelvic and spinal alignment parameters were measured.
RESULTS:
There were 31 cases with complete radiographic information. Pre-THA SVA was 35.7mm, improving to 24.9mm post-THA. Lumbar lordosis was 50.6° standing and 33.8° sitting; maintained post-THA at 50.6° standing and 36.4°sitting. Pelvic incidence remained unchanged in all positions pre and post-THA (49.1° to 51.2°). Pre-THA sacral slope was 36.9° standing, 23.3° sitting and 40.9° supine. This was maintained post-THA (36.0° standing, 22.9°sitting and 39.7°supine). Pre-THA pelvic tilt was 14.5° standing, 27.8° sitting and 8.8° supine. This was maintained post-THA (15.3° standing, 28.2°sitting and 12.0°supine). Lumbar lordosis was significantly less, and pelvic tilt was significantly greater in sitting position than in standing and supine positions, representing the pelvis moves posteriorly as a patient goes to a seated position,
CONCLUSION:
This study establishes baseline values for the normal standing, sitting and supine sagittal spine and pelvic parameters patient’s undergoing THA. THA does not seem to lead to substantial changes in sagittal spine and pelvic radiographic parameters.
Keywords
Lumbar lordosis
pelvic tilt
sagittal spine alignment
sagittal vertical axis
spinopelvic parameters
total hip arthroplasty

Introduction
Significant progress has been achieved regarding the radiographic evaluation of the sagittal spinopelvic alignment over the past decades.[1,2,3] Many studies have demonstrated patients with degenerative lumbar disease adopt posterior pelvic tilt to compensate loss of lumbar lordosis and maintain upright posture.[4] Although hip and spine pathologies often coexist, the role of the hip joint in maintaining sagittal balance remains poorly understood, and few studies have investigated how the hip joint pathology could affect the sagittal spinopelvic alignment. Evaluating the difference prior to and after total hip arthroplasty (THA) is critical to elucidating the role of hip joints in the compensation mechanism.
Although hip surgeons often evaluate sitting x-rays, much attention has been paid to standing radiographic assessment by spine surgeons.[5] In addition, few studies have investigated a spinopelvic alignment in supine position. Post-THA dislocation commonly occurs during postural changes in activities of daily living, particularly when the hip is flexed while sitting, a position in which humans spend a significant amount of time.[6] Thus, understanding the postural changes in spinopelvic alignment is another important issue. However, there is a paucity of evidence in the difference in spinopelvic alignment among postures prior to and after THA.
The aims of our study were 1) to examine the normal radiographic standing and sitting sagittal alignments and pelvic parameters in a typical population undergoing a THA, and 2) to evaluate the postural effects on these parameters in the standing, sitting, and supine positions.
Materials and Methods
Subjects
After receiving Institutional Review Board approval, patients are older than 50 years old scheduled for a primary unilateral THA were approached for participation. After signing an Informed consent subjects had a 36-inch anteroposterior and lateral standing radiograph, an anteroposterior and lateral sitting film and a lateral supine film taken prior to the hip arthroplasty and six months after hip arthroplasty.
Radiographic parameters
Sagittal vertical axis (SVA), lumbar lordosis (LL), pelvic tilt (PT), pelvic incidence (PI), and sacral slope (SS) were measured as previously described.[7] Thoracic kyphosis (TK) was measured as the angle between the upper endplate of T5 and the lower endplate of T12. We evaluated PT and APP-VP (anterior pelvic plane-vertical plane) angle to evaluate sagittal pelvic tilt since spine surgeons typically use PT whereas hip surgeons use APP-VP angle. APP-VP angle was defined as the angle formed by a line drawn from the anterior superior iliac spines to the pubic symphysis and the vertical line connecting the anterior superior iliac spines. This angle was positive in case of pelvis retroversion and negative with the pelvis in anteversion [Figure 1].
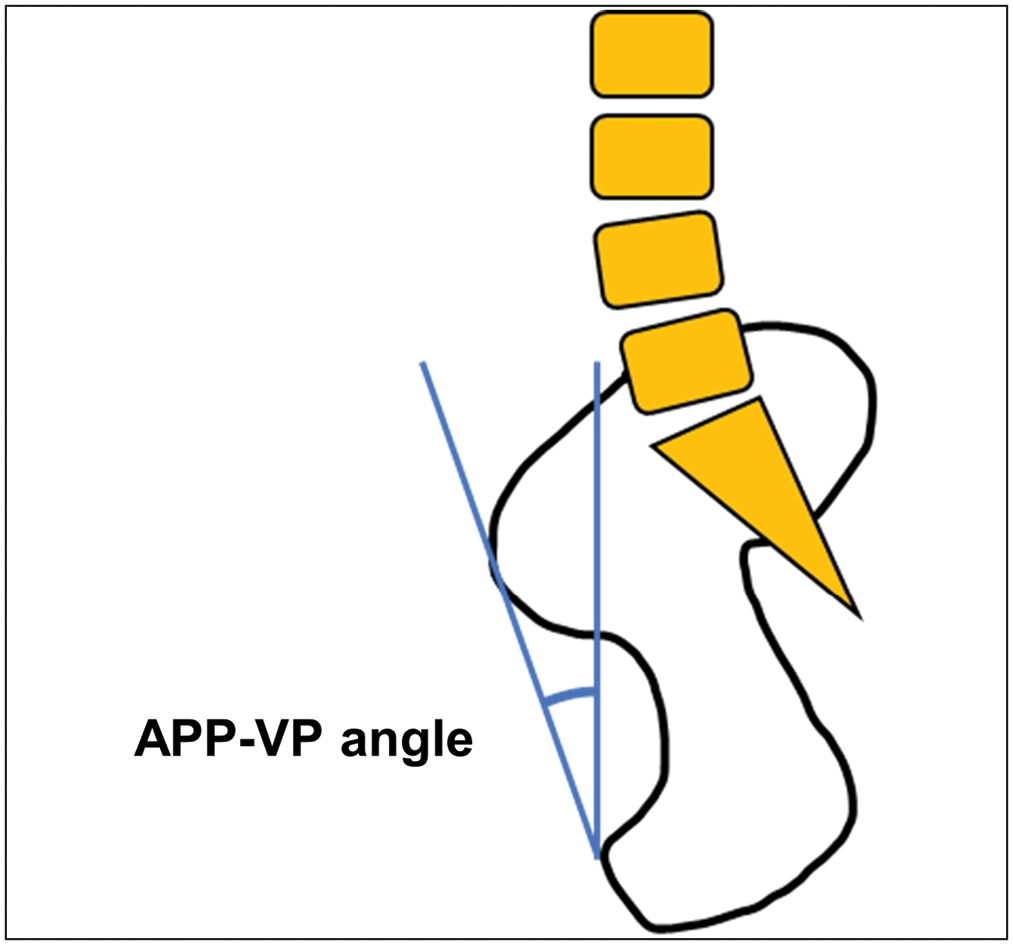
- APP-VP angle was measured between a line drawn from the anterior superior iliac spines to the pubic symphysis and the vertical line
Inter- and intra-observer reliabilities of measurements of the parameters used in the present study have already been shown good to excellent,[8] and was not addressed in this study.
Statistical analysis
Categorical variables were analyzed using the chi-square test whereas continuous variables were analyzed using Student’s t-test. Analysis of variance (ANOVA) was used to assess the difference of continuous measures across the 3 postures. A P value of < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS Statistics 26 (IBM Corp., Armonk, NY). A statistical significance was defined as P value < 0.05.
Results
Thirty-five patients were enrolled. Four patients were excluded due to lack of radiographs. A total of 31 patients (9 males, mean age 65.1 years) were evaluated. Patient demographics were shown in Table 1.
| n = 31 | |
|---|---|
| Mean age (yrs) | 65.1 ± 8.2 |
| Male (%) | 29.0 |
| BMI | 30.1 ± 5.0 |
BMI = body mass index
Mean ± standard deviation
Comparison of changes in the spinopelvic parameters following THA
The pre-operative and postoperative radiographic parameters are shown in Table 2. The interval between pre- and post-THA radiographs was 6.7 ± 0.9 months. Pre-THA SVA was 35.7mm and improved to 24.9mm post-THA. Lumbar lordosis was 50.6° standing and 33.8° sitting; maintained post-THA at 50.6° standing and 36.4°sitting. Pelvic incidence remained unchanged in all positions pre and post-THA (49.1° to 51.2°). Pre-THA sacral slope was 36.9° standing, 23.3° sitting and 40.9° supine. This was maintained post-THA (36.0° standing, 22.9°sitting and 39.7°supine). Pre-THA pelvic tilt was 14.5° standing, 27.8° sitting and 8.8° supine. This was maintained post-THA (15.3° standing, 28.2°sitting and 12.0°supine). Reflecting the pelvic tilt, the pre-THA anterior pelvic plane angle was -1.5° standing, 12.2° sitting and -6.1°; maintained post-THA (-1.4° standing, 13.4° sitting and -5.5° standing). There were no significant changes postoperatively in any parameters including SVA, LL, PT, SS, PI, TK, and APP-VP angle in any of standing, sitting, and supine positions.
| Parameters | Pre-THA | Post-THA | P Value |
|---|---|---|---|
| Standing | |||
| SVA (mm) | 35.7 ± 474 | 24.9 ± 41.8 | 0.141 |
| LL (°) | 50.6 ± 12.3 | 50.6 ± 11.7 | 0.994 |
| PT (°) | 14.5 ± 6.0 | 15.3 ± 8.7 | 0.423 |
| SS (°) | 36.9 ± 75 | 36.0 ± 71 | 0.206 |
| PI (°) | 50.0 ± 8.6 | 49.6 ± 8.9 | 0.637 |
| TK (°) | 35.1 ± 10.5 | 34.1 ± 9.6 | 0.365 |
| APP-VP angle (°) | -1.5 ± 6.5 | -1.4 ± 6.5 | 0.942 |
| Sitting | |||
| SVA (mm) | 50.2 ± 45.9 | 39.7 ± 33.3 | 0.201 |
| LL (°) | 33.8 ± 12.9 | 36.4 ± 14.3 | 0.215 |
| PT (°) | 27.8 ± 9.9 | 28.2 ± 10.3 | 0.708 |
| SS (°) | 23.3 ± 11.7 | 22.9 ± 10.9 | 0.747 |
| PI (°) | 51.2 ± 9.1 | 50.5 ± 8.5 | 0.373 |
| TK (°) | 31.6 ± 10.2 | 30.4 ± 11.1 | 0.261 |
| APP-VP angle (°) | 12.2 ± 5.1 | 13.4 ± 5.7 | 0.211 |
| Supine | |||
| SVA (mm) | 60.4 ± 38.8 | 56.5 ± 36.1 | 0.661 |
| LL (°) | 44.6 ± 11.7 | 44.5 ± 11.1 | 0.954 |
| PT (°) | 8.8 ± 76 | 12.0 ± 11.6 | 0.097 |
| SS (°) | 40.9 ± 8.8 | 39.7 ± 8.0 | 0.165 |
| PI (°) | 49.1 ± 9.1 | 49.2 ± 8.9 | 0.927 |
| TK (°) | 28.5 ± 79 | 27.9 ± 11.2 | 0.701 |
| APP-VP angle (°) | -6.1 ± 9.1 | -5.5 ± 9.1 | 0.807 |
THA = total hip arthroplasty, APP-VP = anterior pelvic plane-vertical plane Mean ± standard deviation
Postural changes in the spinopelvic parameters
Postural changes in the parameters prior to and following THA were shown in Figure 2. SVA was greatest in supine and smallest in standing position. TK was greatest in standing and smallest in supine position. LL and SS were significantly less in sitting position than in standing and supine positions. PT and APP-VP angle were significantly greater in sitting position than in standing and supine positions. These findings were consistent regardless of pre- and post-THA. PI remained unchanged in all positions pre- and post-THA.
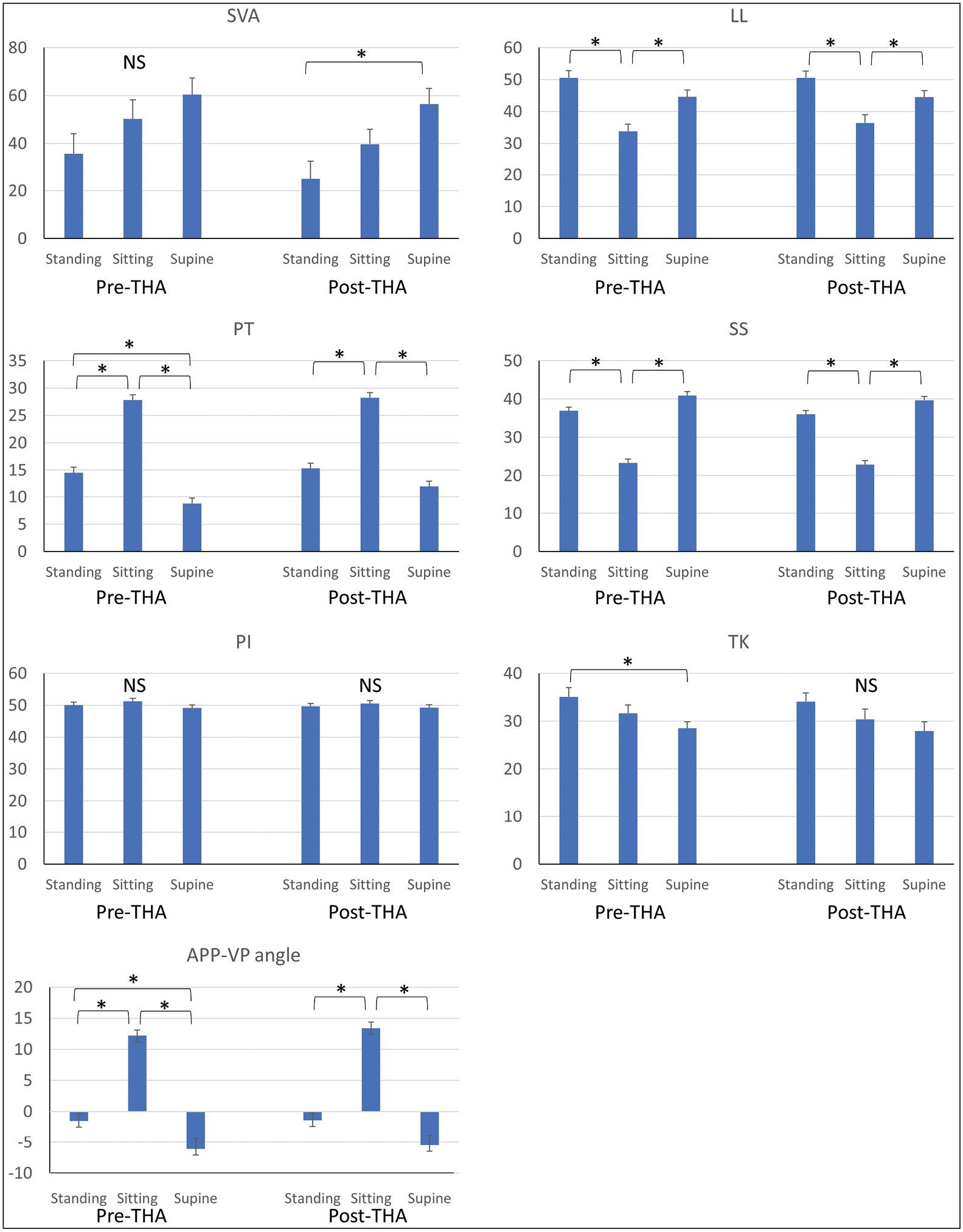
- Differences in sagittal spinal and pelvic parameters in standing, sitting and supine positions prior to and after a total hip arthroplasty
Discussion
Spinopelvic compensatory mechanisms in lumbar degenerative diseases have been well studied. Loss of lumbar lordosis due to degenerative change is compensated for by pelvic retroversion to maintain global sagittal balance.[9,10] However, little is known about compensatory mechanism in patients who have both lumbar and hip pathologies and the impact of THA on spinopelvic alignment. In this study, we demonstrated two important findings. First, we examined whether a THA changed compensatory mechanisms of spinopelvic alignment in patients who had degenerative lumbar disease as well as hip pathology needing a THA. All spinopelvic parameters were not significantly different between pre- and post-THA. This shows that mechanisms, loss of LL was compensated by pelvic retroversion, were maintained after a THA. Second, we compared spinopelvic parameters in standing, sitting, and supine positions pre- and post-THA. Pelvic orientation was significantly different between the postures. The sitting position led to a significantly retroverted pelvis and less LL whereas pelvis was the least retroverted in supine position. This was represented by greater PT and APP-VP, and smaller SS and LL in sitting position. Potential alterations these changes in alignment may be hypothesized as a possible cause of an observed increase in total hip arthroplasty dislocations in patients who have had a previous spinal fusion.
A few studies have been performed regarding the impact of THA on spinopelvic compensation. A previous study showed that patients with severe hip osteoarthritis have a flexed hip joint and pelvic anteversion. The lumbar spine had a limited ability to compensate for the pelvic anteversion in these patients, leading to a high incidence of severe unbalance in sagittal plain.[11] Weng et al. compared SS, PT, and LL before and at 1 year after THA, and showed THA partially restored spinopelvic alignment.[12] However, as the present study showed, THA did not result in significant change in the sagittal alignment of the pelvis and lumbar spine in other studies.[13,14] This discrepancy may be due to the difference in the severity of preoperative hip ROM. Further evaluation will be needed to answer this question.
Most of previous studies evaluated only upright radiographs. However, dislocation episodes commonly occur during postural changes in activities of daily living (e.g., standing up and sitting down in a chair, picking an object up off the floor).[6] Therefore, the effect of spinopelvic interactions during postural changes needs further evaluation. Several studies have demonstrated the change of pelvic orientation in various positions.[15,16,17] These studies examined difference in spinopelvic alignment between standing and sitting position using only pre-THA radiographs. Few studies investigated all three main postures including supine, standing, and sitting positions. There is no study to compare spinopelvic alignment between 3 postures pre- and post-THA. In the current study, we evaluated pelvic orientation pre- and post-THA in all three postures. When lying, pelvis is tilted forward. In standing position, pelvis is slightly retroverted. As the patient goes to a seated position, the pelvis is the most retroverted. The difference of pelvic orientation between postures was maintained pre- and post-THA. Our findings not only support previous studies but also provide more details in the impact of THA on spinopelvic alignment.
Sagittal pelvic tilt is the most important parameter when undergoing THA, as acetabular cup orientation is a crucial factor to avoid post-THA dislocation and cup orientation is affected by sagittal pelvic tilt. Spine surgeons typically use PT while hip surgeons prefer APP-VP to see sagittal pelvic tilt. We examined both parameters. Both parameters had similar trend, in which pelvis was the most retroverted in sitting and the least retroverted in supine, and considered to be feasible for evaluation of sagittal pelvic tilt. It was reported that a stiff lumbar spine had an increased risk of dislocation.[18] Sultan et al. reported that dislocation rates ranged between 3% at 1 year and 7.5% at 2 years in THA patients with previous lumbar spinal fusion, exceeding the average rate.[19] Murphy et al[6] showed that 32% of patients who had developed recurrent dislocation had the cup in the safe zone.[20] The mechanism is postulated as follows. Sitting position can be achieved through a combination of flexion of lumbar spine and hip joints, and pelvic retroversion. Patients with stiff spines have a limited change in LL and PT from standing to sitting position,[21] and therefore need to flex their hips to a greater degree to achieve a sitting position,[18] which may lead to impingement between proximal femur and the rim of the acetabulum. In our cohort, patients successfully increased PT when changing posture from standing to sitting [Figure 1], suggesting any existing lumbar pathology had little effect on hip dislocation. Attention should be paid for lumbar stiffness before undergoing THA. The change in sagittal pelvic tilt during the postural changes from standing to sitting is strongly related to the mobility of the lumbar spine in patients with hip diseases who are candidates for THA. The preoperative consideration of lumbar spine mobility using standard radiography with dynamic evaluations in the standing and sitting positions might contribute to better patient outcome.[16]
There are several limitations in this study. First, we evaluated short-term period of changes in the parameters. The interval between pre- and post-THA radiographs was 7 months. We may need radiographic follow-up in long-term period of time to understand more details. Second, we evaluated only radiographic parameters. No clinical outcomes were evaluated although residual hip pain or back pain might influence postop spinopelvic parameters. Lastly, the sample size is relatively small, and the patients did not have significant spinal deformity prior to their THA. The most important finding is that in patients undergoing a THA who do not have a preexisting spinal fusion did not have changes in spinal alignment compensation with the exception that there was a trend toward improved SVA without statistical significance. Further studies may identify a significantly different outcome in patient undergoing THA with prior spinal fusion. Despite these limitations, our study has valuable information since this is the first study to comprehensively evaluate spinopelvic parameters in 3 postures prior to and after THA.
Conclusions
This study establishes baseline values for the normal standing, sitting and supine sagittal spine and pelvic parameters in patients undergoing THA. Compensation mechanism was maintained pre- and post-THA. In sitting position, pelvis was significantly retroverted, which should be considered prior to a THA or a spino-pelvic fusion to avoid dislocation. There were no substantial changes in the sagittal spine and pelvic parameters after THA. Future studies will find this study useful as a detailed control cohort for comparison of the spino-pelvic indices and their potential differences in patients with a concurrent spine fusion and THA.
Ethics approval
This study was approved by the University of Louisville Institutional Review Board and Norton Healthcare Office of Research Administration.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Not applicable.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005;30:2024-9.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of decompression surgery without fusion for lumbar spinal stenosis on sagittal spinopelvic alignment: Minimum 2-year follow-up. J Neurosurg Spine. :1-7. [Epub ahead of print].
- [CrossRef] [PubMed] [Google Scholar]
- Impact of sagittal spinopelvic alignment on clinical outcomes and health-related quality of life after decompression surgery without fusion for lumbar spinal stenosis. J Neurosurg Spine. :1-6. [Epub ahead of print].
- [CrossRef] [PubMed] [Google Scholar]
- When is compensation for lumbar spinal stenosis a clinical sagittal plane deformity? Spine J. 2016;16:971-81.
- [CrossRef] [PubMed] [Google Scholar]
- Spinopelvic compensatory mechanisms for reduced hip motion (ROM) in the setting of hip osteoarthritis. Spine Deform. 2019;7:923-8.
- [CrossRef] [PubMed] [Google Scholar]
- The safe zone range for cup anteversion is narrower than for inclination in THA. Clin Orthop Relat Res. 2018;476:325-35.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: A prospective multicenter analysis. Spine (Phila Pa 1976). 2013;38:E803-12.
- [CrossRef] [PubMed] [Google Scholar]
- Determining the validity and reliability of spinopelvic parameters through comparing standing whole spinal radiographs and upright computed tomography images. Bmc Musculoskelet Disord. 2021;22:899.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of compensatory mechanisms in the pelvis and lower extremities in patients with pelvic incidence and lumbar lordosis mismatch. Gait Posture. 2017;56:14-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pelvic retroversion: A compensatory mechanism for lumbar stenosis. J Neurosurg Spine. 2017;27:137-44.
- [CrossRef] [PubMed] [Google Scholar]
- Characteristics of sagittal spine-pelvis-leg alignment in patients with severe hip osteoarthritis. Eur Spine J. 2015;24:1228-36.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of total hip arthroplasty on sagittal spinal-pelvic-leg alignment and low back pain in patients with severe hip osteoarthritis. Eur Spine J. 2016;25:3608-14.
- [CrossRef] [PubMed] [Google Scholar]
- Change in spinal alignment after total hip arthroplasty. Orthop Surg. 2013;5:261-5.
- [CrossRef] [PubMed] [Google Scholar]
- Hip-spine syndrome: The effect of total hip replacement surgery on low back pain in severe osteoarthritis of the hip. Spine (Phila Pa 1976). 2007;32:2099-102.
- [CrossRef] [PubMed] [Google Scholar]
- Lumbar-pelvic-femoral balance on sitting and standing lateral radiographs. Orthop Traumatol Surg Res. 2013;99:S87-103.
- [CrossRef] [PubMed] [Google Scholar]
- Importance of the spinopelvic factors on the pelvic inclination from standing to sitting before total hip arthroplasty. Eur Spine J. 2016;25:3699-706.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal factors influencing change in pelvic sagittal inclination from supine position to standing position in patients before total hip arthroplasty. J Arthroplasty. 2014;29:2294-7.
- [CrossRef] [PubMed] [Google Scholar]
- Total hip arthroplasty patients with fixed spinopelvic alignment are at higher risk of hip dislocation. J Arthroplasty. 2018;33:1449-54.
- [CrossRef] [PubMed] [Google Scholar]
- The impact of spino-pelvic alignment on total hip arthroplasty outcomes: A critical analysis of current evidence. J Arthroplasty. 2018;33:1606-16.
- [CrossRef] [PubMed] [Google Scholar]
- Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60:217-20.
- [CrossRef] [Google Scholar]
- Predictability of acetabular component angular change with postural shift from standing to sitting position. J Bone Joint Surg Am. 2014;96:978-86.
- [CrossRef] [PubMed] [Google Scholar]




