
Translate this page into:
MRI and functional assessment of triportal technique in arthroscopic anatomical single-bundle anterior cruciate ligament reconstruction
Address for correspondence: Dr. Nishanth Shetty, “Kanchana” House, Kadri Kambla Road, Mallika Extension, Bejai-Mangalore 575004, Karnataka, India. E-mail: ynshetty@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Balemane S, Shetty N, Ramu AC, Rahman A. MRI and functional assessment of triportal technique in arthroscopic anatomical singlebundle anterior cruciate ligament reconstruction. J Orthop Spine 2022;10:56-62.
Abstract
BACKGROUND:
Arthroscopic anterior cruciate ligament (ACL) reconstruction surgery is routinely performed using two standard portals; however imprecise portal placement leads to the most common surgical error that is associated with the imprecise placement, which is the non anatomical positioning anatomical positioning of the femoral tunnel because of improper visualization of the posterior aspect of the medial surface of lateral femoral condyle, due to inadequate visualization of the attachment area over the femur using the standard two portals. To decrease the incidence of this error, various other portals have been descried to improve the visualization. We propose the routine use of an accessory medial portal, in addition to the standard anterolateral and anteromedial portals, to enhance the visualization of the lateral wall and to improve the anatomic accuracy. The arthroscope can also be moved interchangeably throughout the portals during the procedure for improved viewing during specific steps. The routine use of this portal was assessed both clinically and radiologically in our study at the end of 1 year by functional scoring and magnetic resonance imaging (MRI) scan, wherein the accuracy of the femoral attachment and healing of the graft were checked.
OBJECTIVES:
To assess the functional and radiological results of the routine use of triportal technique in anatomical ACL reconstruction.
MATERIALS AND METHODS:
We conducted a prospective study on 20 patients who were assessed preoperatively and postoperatively at the end of 12 months using the International Knee Documentation Committee and Lysholm score, and the stability was checked with Lachman and pivot shift test. An MRI of the postoperative knee was performed after 12 months to assess the position of the graft, graft integrity, and healing.
RESULTS:
All the patients at the end of the study had an exceptional functional and clinical outcome, which was correlated on MRI showing a near-accurate placement of the femoral tunnel with acceptable inclination. All our patients showed excellent anteroposterior and rotational stability when assessed by IKDC and Lysholm score at the end of 1-year follow-up.
CONCLUSION:
This study shows that the routine use of the accessory anteromedial portal gives a good functional outcome with the near-accurate placement of femoral tunnel, which corresponds to the MRI findings obtained in our study.
Keywords
Anatomical reconstruction
anterior cruciate ligament
MRI
rotational stability
triportal technique

Introduction
Anterior cruciate ligament (ACL) rupture is one of the most frequent orthopedic sports injuries,[1] which is manifested by a moderate-to-severe disability by the “giving way” episodes the patient experiences during activities of daily living, especially during sports activities. Therefore, arthroscopic (ACL) reconstruction is one of the most often performed orthopedic surgeries. The goal of ACL reconstruction is to replicate the functions of the native ACL.[2] The long-term function of the reconstruction can be assessed by the obliquity of the ligament; hence, various methods have been described to improve our obliquity of fixation of the ACL, which can be achieved only if we get a proper trajectory during the identification and drilling of the tunnels. Most surgeons use only two portals for arthroscopic ACL surgeries; however to improve the visualization of various compartments of the knee, different portals have been described like the one described by Gillquist et al. for the examination of the other regions of the knee, i.e., the patellofemoral and posteromedial compartments.[2] Cohen and Fu have suggested that the use of the only two portals may limit the visualization of the tibial insertion and also limit the adequate visualization of the lateral femoral condyle, and they routinely use the three portal technique for double-bundle ACL reconstruction.[3] The early and accelerated progression of arthritis and the suboptimal outcomes achieved after a inaccurate ACL reconstruction warrants us to change our surgical technique from a standard two portal to a standard three portal technique to obtain a near anatomical ACL.[4]
Materials and Methods
This prospective study was conducted on 20 patients with a complete ACL tear in a tertiary care center between 2016 and 2017. All the patients were treated using the three portals, i.e., the anteromedial, anterolateral, and the accessory anteromedial portals with a hamstring autograft. The scoring system used in this study is the International Knee Documentation Committee (IKDC) score, Lysholm score, and stability score. There were 15 (75%) male and five (25%) female patients. The mean age of the patients was 28.65 ± 4.84. We excluded patients with multiple ligament injury, the presence of a chondral lesion, advanced osteoarthritis, and partial ACL injury. The patients with an associated meniscal injury were identified and treated before or during the operation, and this was done in eight patients (40%), wherein two patients underwent meniscal repair before surgery. The patients were followed up for 12 months.
Operative technique
All operations were performed under spinal anesthesia and with the help of a well-padded thigh tourniquet, in the supine position with a lateral support for the thigh. Examination under anesthesia before ACL reconstruction was done for all patients to ensure ACL deficiency by positive Lachman and pivot shift tests. Informed consent was obtained from all the patients who were included in the study. All patients received a preoperative antibiotic (1 g ceftriaxone IV) 30 min before the operation. Routine diagnostic arthroscopy was performed initially to confirm the diagnosis and to evaluate other pathological conditions (chondral damage and meniscal tears). Any meniscal problems were treated before proceeding to the reconstruction of ACL. Minimal debridement of ACL stump was done leaving behind fibers so as to not obstruct the possible vascular and cellular ingrowth and to avoid the destruction of proprioceptive receptors.
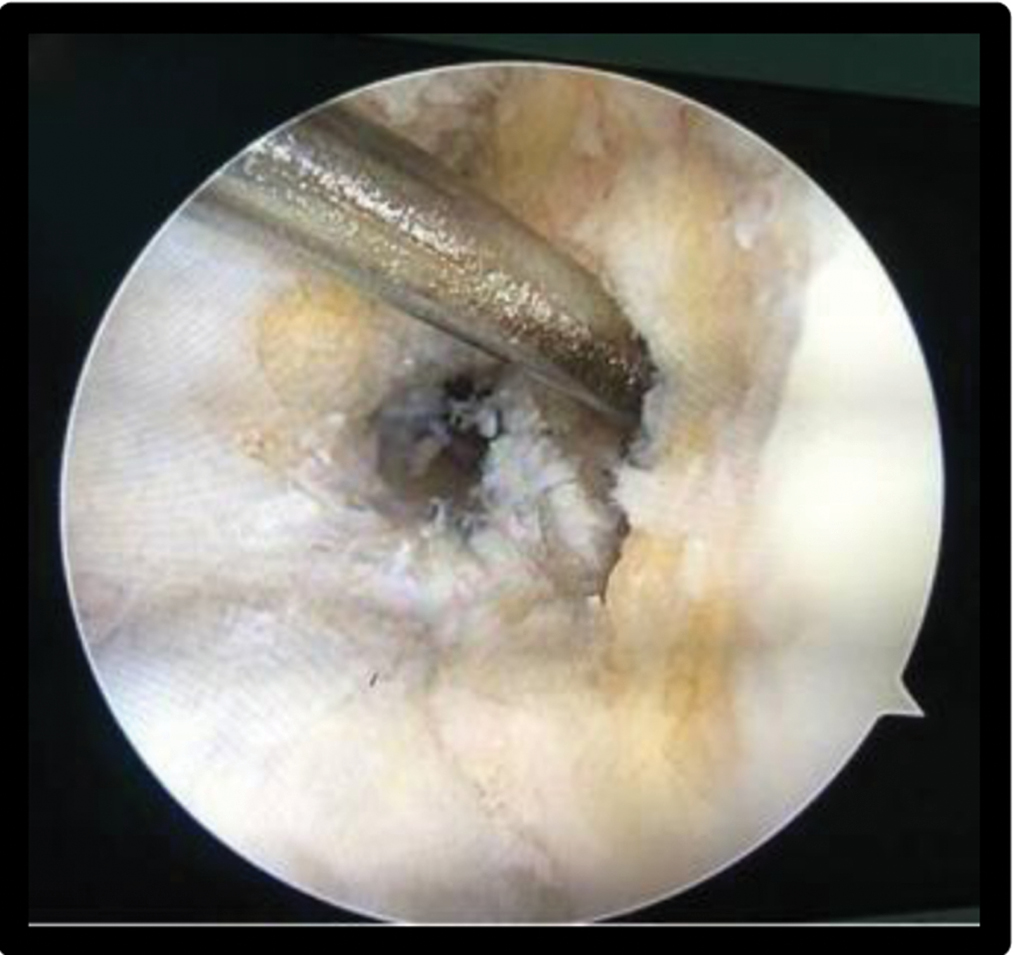
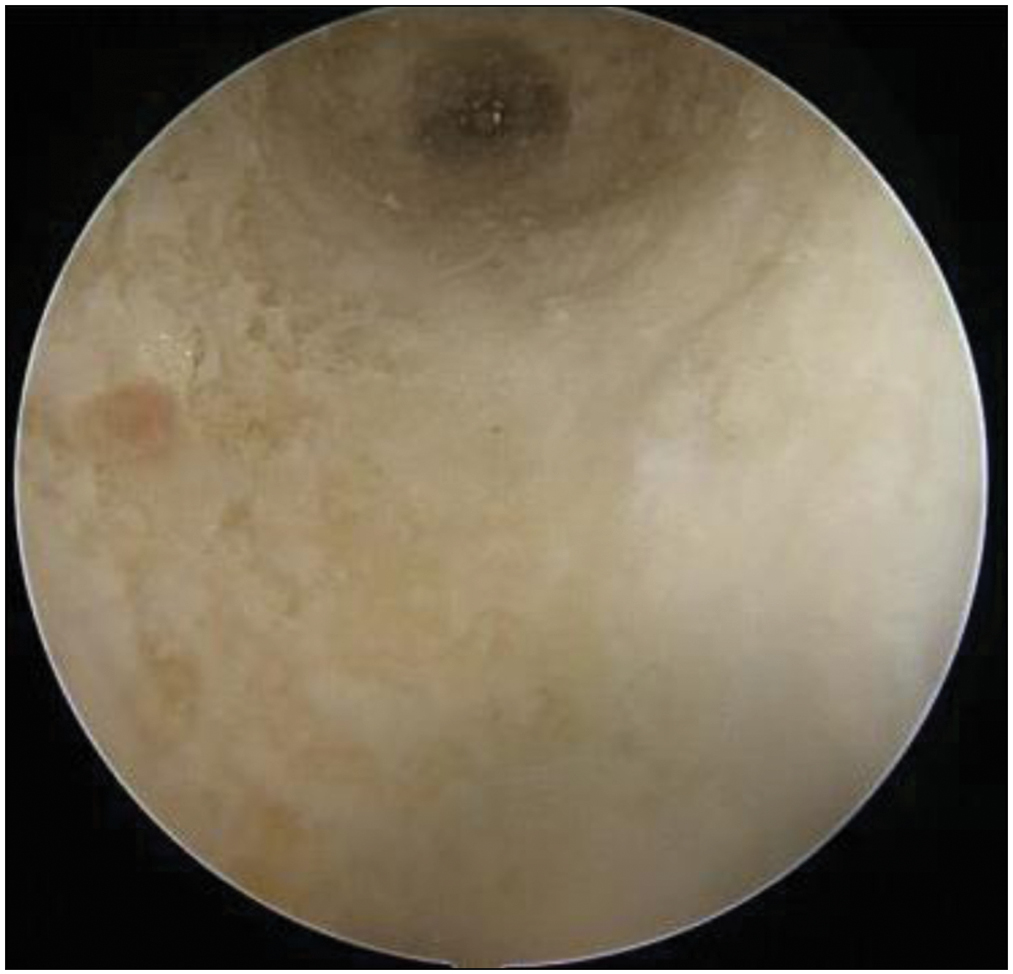
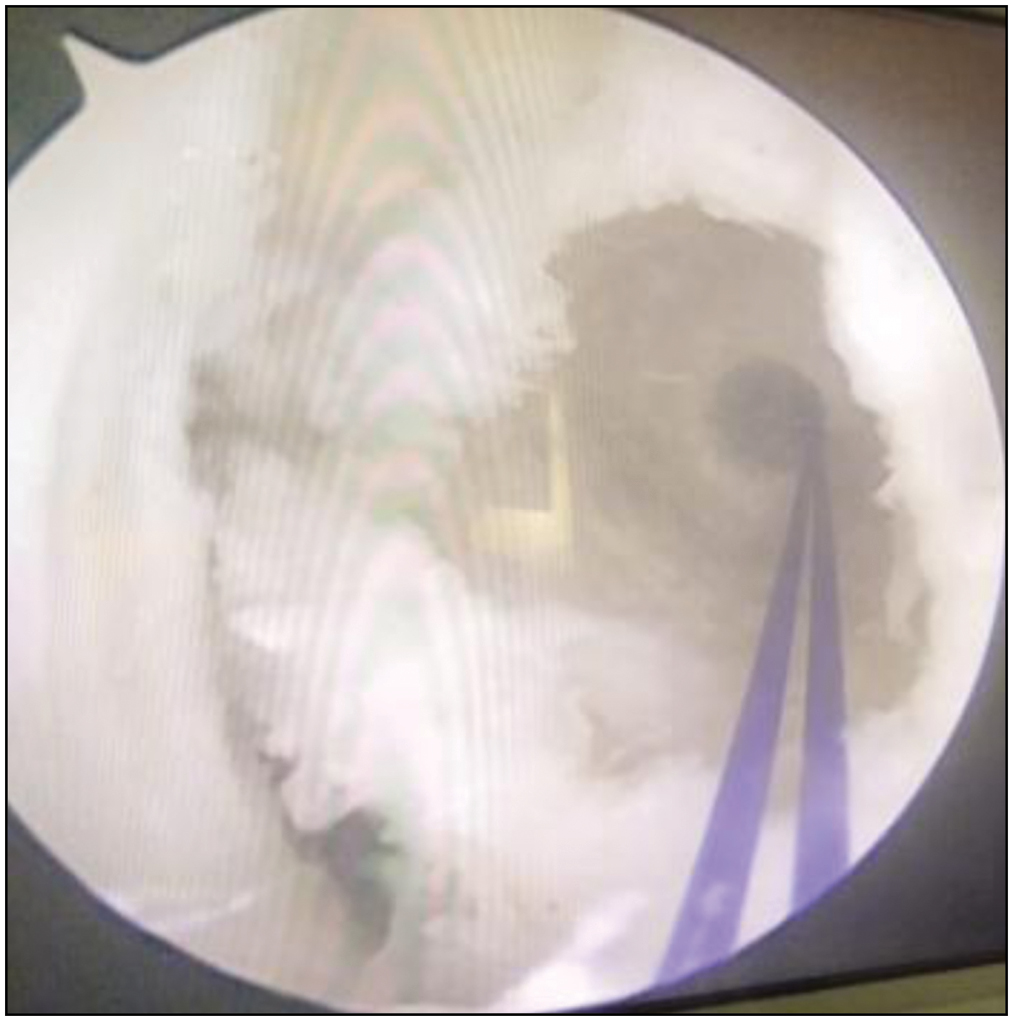
Our method of using two anteromedial portals was performed mainly for the placement of the femoral tunnel. The standard anterolateral portal and anteromedial portals were created [Figure 1]. Another anteromedial portal (far anteromedial or accessory portal) was established as distant as possible from the previous portal (2 cm medial to the medial edge of the patellar tendon and just above the meniscus in the horizontal plane), using a spinal needle to confirm the position as well as the trajectory, such that the medial femoral condyle does not get damaged, thus avoiding complications that can be caused by the interference of the reamer and the arthroscope. This portal permits the arthroscopic visualization of the medial surface of the lateral femoral condyle with the knee in hyperflexion; hence, the anatomic ACL insertion site on the femur and the posterior cortical bone can be located with ease [Figure 2]. On visualizing the anatomical femoral ACL insertion on the medial surface of lateral femoral condyle, the center of anteromedial (AM) bundle of ACL footprint is identified and marked (posterior to lateral bifurcating ridge)[5] with the help of microfracture awl inserted through accessory anteromedial portal. A guide pin was inserted at the point of a pilot hole, which was already made by microfracture awl through the accessory medial portal [Figures 3 and 4]. The femoral tunnel was created using a suitable size reamer up to 20–25 mm depending on femoral condylar length such that lateral femoral cortex should be intact, which was visualized through the accessory anteromedial portal [Figure 5].
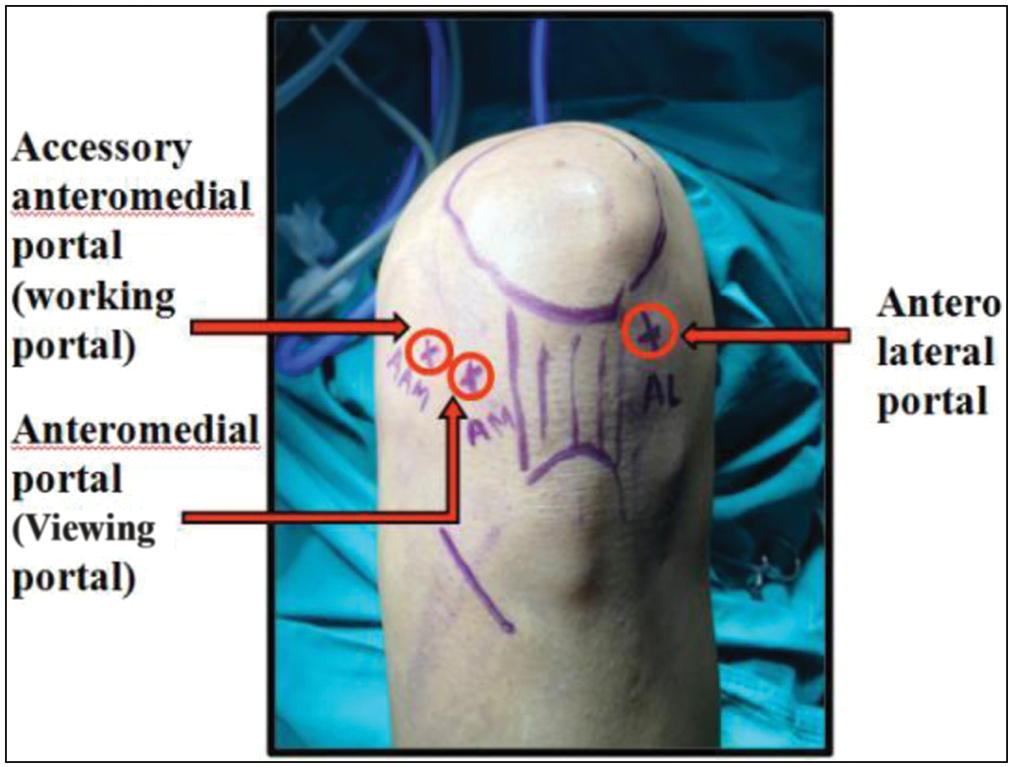
- Standard triportals (anterolateral, accessory anteromedial, and anteromedial)

- Visualization of anatomical femoral ACL insertion on the medial surface of lateral femoral condyle and the creation of femoral tunnel posterior to lateral bifurcating ridge with the help of microfracture awl inserting through accessory anteromedial portal

- Guide pin inserted through the accessory medial portal
- Intraoperative (arthroscopy) picture of the same
- Intact lateral femoral cortex visualized through the accessory anteromedial portal
A tibial tunnel was drilled with a guide pin placed at the center of the ACL insertion site on the tibia, taking care to preserve the remaining ACL tissue as much as possible following which the graft was passed through the femoral tunnel. The graft was fixed with a suspensory fixation at the femoral side [Figures 6 and 7] and the tibial side was fixed with a bioabsorbable screw after cyclical loading of the graft and tautness of the graft was checked with a probe [Figure 8]. The entry of the suspensory fixation into femoral tunnel and the confirmation of the flip of the suspensory fixation device were confirmed by placing the arthroscope in the accessory anteromedial portal [Figure 7]. Postoperative radiographs were done to confirm the tunnel position and the position of the suspensory fixator device [Figures 9 and 10].
- Arthroscopic visualization of the femoral insertion after reaming from the accessory anteromedial portal
- View from the anteromedial portal of the suspensory fixation

- Final position of the graft
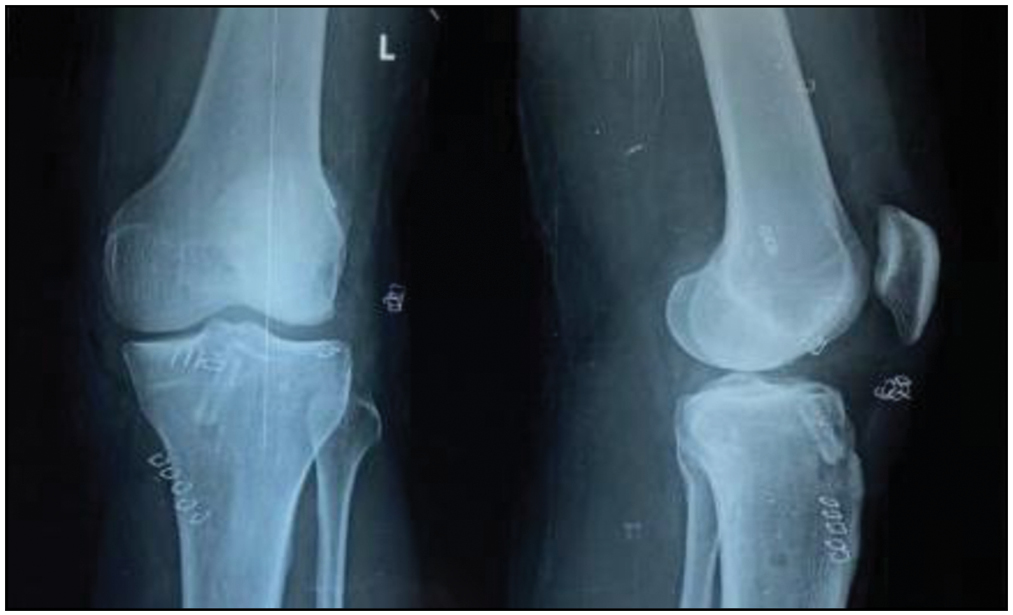
- Postoperative x-ray showing the tunnel position
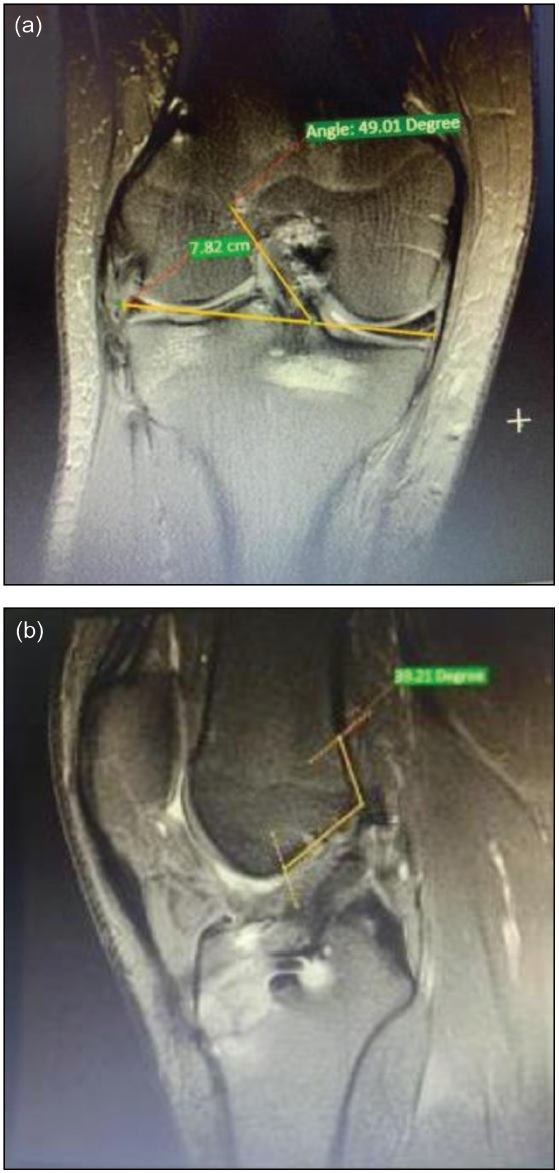
- Calculation of the inclination of the graft in (a) coronal and (b) saggital plane
The postoperative rehabilitation protocol employed was in accordance with the accelerated rehabilitation protocol of Shelbourne and Nitz[6] Joint flexion and extension were allowed starting from the day after the surgery. In patients who did not undergo a meniscal repair procedure, partial weight bearing was allowed for 2 weeks with a knee brace. After 2 weeks, full weight bearing was allowed. In patients who underwent a meniscal repair, partial weight bearing was allowed for 6 weeks with the knee. Jogging was permitted 3 months after the surgery. Sports activity was allowed from 6 to 9 months after surgery depending on the state of recovery.
We performed an magnetic resonance imaging (MRI) for all patients after 12 months to assess the position of the graft and the accuracy of femoral tunnel placement for the purpose of this study. The femoral tunnel was located, and the inclination of the graft in both coronal and sagittal planes was calculated.
Postoperative complications we encountered were an intraoperative lateral femoral cortex blow out in one case (3.3%). Postoperative superficial wound infection at the graft site was observed in one case (3.3%). Also, tourniquet neuropraxia was observed in one case (3.3%). Finally, postoperative neuropraxia of the saphenous nerve was seen in two cases (6.6%).
Statistical analysis was expressed as means ± standard deviation (SD). The data obtained from the used triple score system were analyzed statistically using Wilcoxon signed-rank test. P values less than 0.05 were considered significant.
Results
The evaluation of ACL injury and associated injuries was as follows:
Site of injury: 12 patients had their ACL injury in the left knee (60%), whereas eight patients had their ACL injury in the right knee (40%).
Mechanism of injury: 10 patients (50%) in this study were injured in a road traffic accident, five patients (25%) were injured during sports, and five patients (25%) were injured at the work site.
Associated meniscal injury: Eight patients (40%) had a meniscal injury, wherein two patients underwent meniscal repair before surgery.
Assessment of the results of surgery
Assessment using IKDC scoring system
Before surgery, 10 (50%) patients had IKDC grade (D), and 10 (50%) patients had IKDC grade (C). After surgery, 16 (80%) patients had normal IKDC grade (A) and four (20%) patients had nearly normal grade (B) [Figure 11].
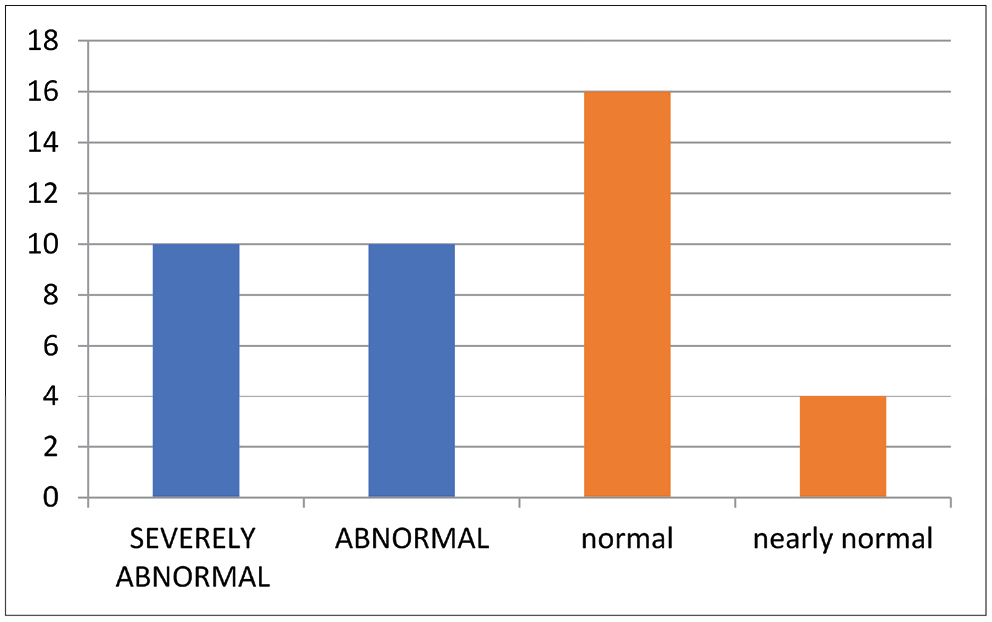
- Final results of IKDC score
Lysholm score
Before surgery, the mean score was 46.7 ± 3.5, and after surgery, the mean rose to 87.3 ± 9.44 [Figure 12]; it was not normally distributed, so nonparametric test, Wilcoxon signed-rank test, was used. It gave a P value of 0.0001, which is statistically significant.
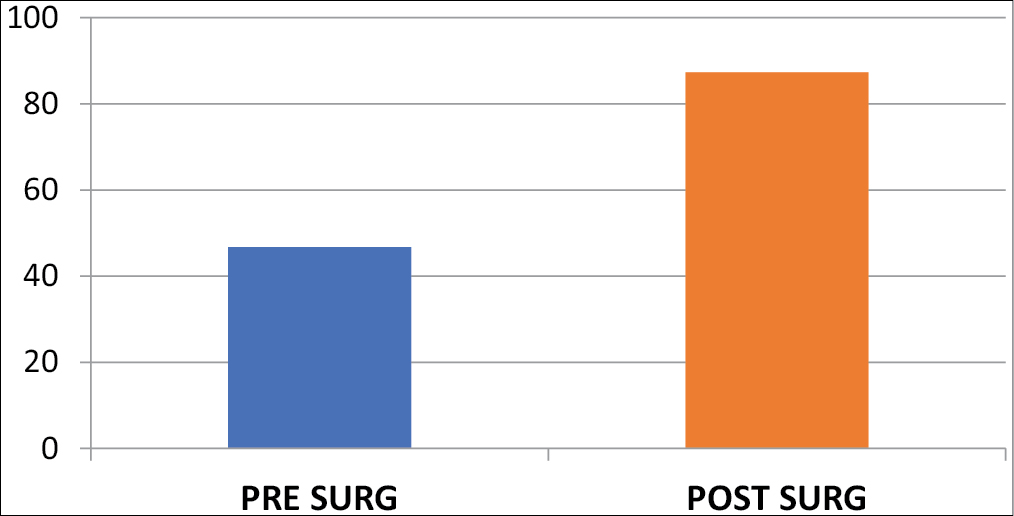
- Pre- and postoperative means of the Lysholm score
Stability scoring system
Lachman score
Before surgery, Lachman score was 3+ in 14 patients (70%), 2+ in four patients (20%), and 1+ in two patients (10%). After surgery, all Lachman tests were negative [Figure 13].
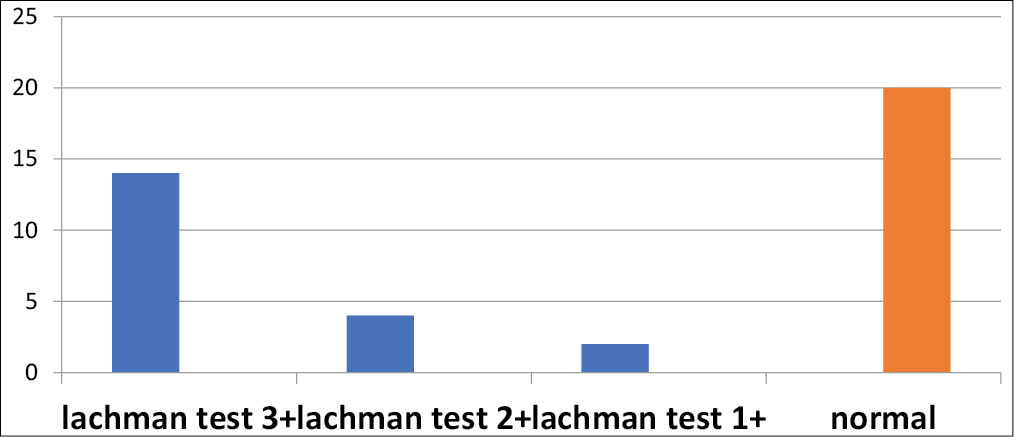
- Preoperative and postoperative means of the stability score
Pivot shift test
Before surgery, the pivot shift test was 3+ in 12 patients (60%), 2+ in six patients (30%), and 1+ in two patients (10%). After surgery, the pivot shift test was negative in 95%, and one patient had 1+ (5%) pivot shift test positive [Figure 14].
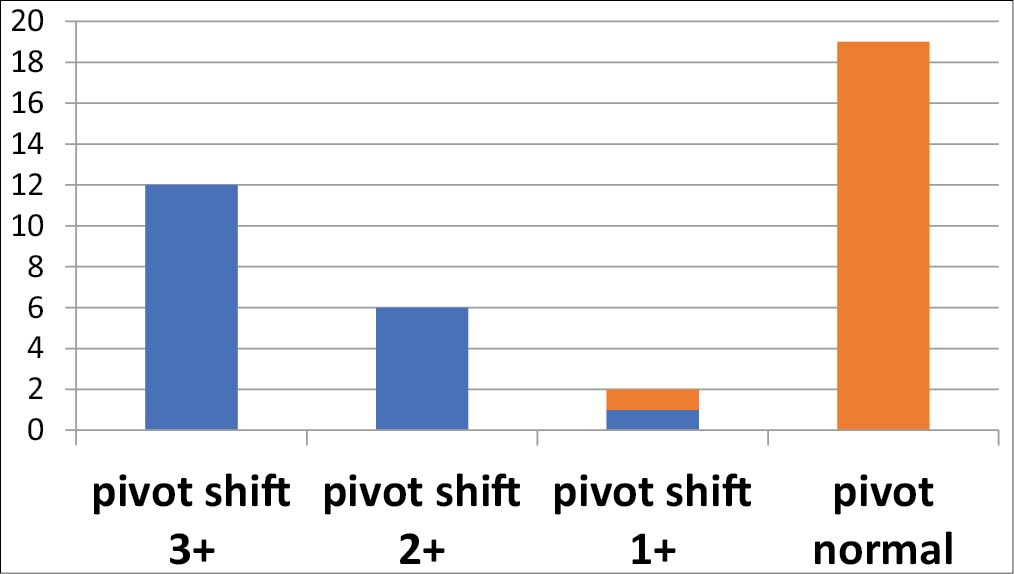
- Preoperative and postoperative means of the pivot shift test
MRI evaluation: The average inclination was found to be less than 75° on coronal section [Table 1], and the femoral graft was found to be at near-accurate location at the intersection of the line connecting the posterior condyle of the femur and lateral wall of the intercondylar notch[7] when evaluated on coronal and sagittal sections, respectively. All grafts were behind the Blumensaat line [Figure 10].
| S. no. | Femoral tunnel location on the MR images | |
|---|---|---|
| Sagittal inclination | Coronal inclination | |
| 1 | 54 | 72 |
| 2 | 49.8 | 74 |
| 3 | 53 | 70.5 |
| 4 | 54.7 | 73.2 |
| 5 | 55.2 | 74 |
| 6 | 52.3 | 73.2 |
| 7 | 54.4 | 73.2 |
| 8 | 53.8 | 74 |
| 9 | 54.3 | 72.8 |
| 10 | 53.8 | 70 |
| 11 | 52.9 | 73.4 |
| 12 | 54.6 | 74.3 |
| 13 | 55 | 73.5 |
| 14 | 52.8 | 73.8 |
| 15 | 54 | 74 |
| 16 | 53.6 | 73.2 |
| 17 | 55.5 | 71 |
| 18 | 54.4 | 72 |
| 19 | 53.9 | 74.2 |
| 20 | 52.8 | 73 |
Discussion
Most authoritative textbooks report that the most common portals used routinely in arthroscopically assisted ACL reconstruction procedures are the standard anterolateral portal and anteromedial portal.[6,8] The anteromedial portal is in general used as a working portal or a diagnostic portal, and the variation in the position of this portal may either help us in meniscal repair procedures or ACL reconstruction. The surgical failure of the procedure is mainly due to nonanatomical reconstruction of the ACL. The femoral tunnel position influences not only knee kinematics but also graft length much more than the tibial tunnel position; hence, the accurate positioning of the femoral tunnel is critical, because of its close proximity to the center of axis of knee motion.[4,5]
The most common complication associated with ACL reconstruction is erroneous tunnel placement, and this is mainly due to the improper visualization of the anatomical footprint of the ACL. Various portals have been described as and when unanticipated needs arise, like the medial midpatellar portal, which offers a wider view of the intercondylar notch almost directly from below rather than sideways.[7] The use of high portals has also been advocated to attain the widest view and least instrument crowding.[8] Cohen and Fu[3] in their study have advocated the use of a central AM viewing portal to determine the femoral origin of the AM and posterior medial bundles of the ACL on the femur. Thus, the accessory AM portal was used as the working portal for drilling the femoral tunnel. Hence, we propose the routine use of an accessory anteromedial portal in single-bundle ACL reconstruction too, which is in accordance with the above-mentioned study for double-bundle ACL reconstruction, and this also helps prevent notchplasty, thereby improving our viewing/accessibility of the interested area.
In this prospective study, all the 20 patients who had a complete ACL injury underwent anatomic single-bundle ACL reconstruction using a hamstring autograft using the triportal technique. All the patients had an excellent result with the routine use of the three portals, further substantiating the need for the routine use of this portal to help us identify and approach the native ACL. This accessory anteromedial portal thus provides intraoperative advantages such as proper visualization of the lateral cortex of the femur and also the native femoral footprint of the ACL; anatomical reconstruction of femoral footprint, targeting the AM bundle of the native ACL; visualizing the femoral canal postreaming after reaming and also assessing the integrity of the intact lateral cortex; easy accessibility for femoral drilling. The accessory anteromedial portal is also helpful for the direct visualization of the passage of the implant and to confirm the flipping of the implant overt the lateral cortex. In order to check the position and accuracy of using the accessory anteromedial portal, we performed an MRI after 12 months to assess the position, integrity, and inclination of the graft. It is widely accepted that the ideal femoral tunnel in single-bundle ACL reconstruction should be located at the intersection of the posterior femoral cortex and the lateral wall of the intercondylar notch,[9] which was seen in all our cases. The average graft inclination of the graft was less than 75 degrees on coronal plane, which correlates with the study by Grassi et al.[5] showing less chances of rotational-related failure of graft.
The drawback of the study includes a smaller number of patients included in the study, we did not assess the integration of the graft on the MRI, and we did not check for any long-term changes such as early osteoarthritis, graft loosening, and changes/widening of the tunnel.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Biomechanics and anterior cruciate ligament reconstruction. J Orthop Surg Res. 2006;1:2.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic examination of the posteromedial compartment of the knee joint. Int Orthop. 1979;3:13-8.
- [CrossRef] [PubMed] [Google Scholar]
- Three-portal technique for anterior cruciate ligament reconstruction: Use of a central medial portal. Arthroscopy. 2007;23:325.e1-5.
- [CrossRef] [PubMed] [Google Scholar]
- Tunnel placement in anterior cruciate ligament reconstruction: MRI analysis as an important factor in the radiological report. Skeletal Radiol. 1997;26:409-13.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging after anterior cruciate ligament reconstruction: A practical guide. World J Orthop. 2016;7:638-49.
- [CrossRef] [PubMed] [Google Scholar]
- Accelerated rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med. 1990;18:292-9.
- [CrossRef] [PubMed] [Google Scholar]
- Management of acute anterior cruciate ligament injuries. The Adult Knee. 2003;1:663-706.
- [Google Scholar]
- A view from above: A modified Patel’s medial midpatellar portal for anterior cruciate ligament arthroscopic surgery. Arthroscopy. 2007;23:324.e1-5.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopy of the lower extremity. In: Canale ST, Beaty JH, eds. In: Campbell's Operative Orthopaedics (12th ed.). Philadelphia, PA: Elsevier;; 2013. p. :2395.
- [Google Scholar]




