
Translate this page into:
Posterior instrumented stabilization in the management of unstable thoracolumbar spine fractures with minimum 2 years follow-up
Address for correspondence: Dr. Pramod Nittur Kumaraswamy, Department of Orthopaedics, PD Hinduja National Hospital & MRC, Mahim, Mumbai 400016, Maharashtra, India. E-mail: drpramodnk@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kumaraswamy PN, Takhelmayum U, Singh LL, Chirom D, Maku PN, Lingaraju YM. Posterior instrumented stabilization in the management of unstable thoracolumbar spine fractures with minimum 2 years follow-up. J Orthop Spine 2022;10:49-55.
Abstract
BACKGROUND:
Thoracolumbar region (T11–L2) involvement is most common among the spinal injuries often associated with catastrophic neurodeficits. There are many classification systems to describe thoracolumbar fractures, but few have been useful in recommending surgical decision. The treatment of thoracolumbar fracture has been debated extensively. Optimal surgical approach to be used to treat thoracolumbar fractures remains controversial.
MATERIALS AND METHODS:
Thirty-four patients with thoracolumbar injury classification and severity score ≥5, who underwent posterior instrumentation, were studied prospectively between August 2018 and July 2021. Follow-up assessment was done using x-ray, American Spinal Injury Association (ASIA) impairment scale, Denis pain and work scale, and Oswestry disability index.
RESULTS:
Most of the patients were belonged to age group 31–40 years (44.1%, n = 15); L1 was the most common vertebra injured (61.8%, n = 21). Average kyphosis correction obtained by surgery was 10.53°, and the average loss of kyphosis correction at 2 years was 2.94°. Surgery duration and blood loss when compared between short-segment fixation (SSF) and long-segment fixation (LSF) showed a statistical significance (P < 0.0001). Associated injuries were seen in 11.76% (n = 4) of patients. At final follow-up, 85.71% (n = 24) of patients showed improvement to one higher ASIA grade; 82.4% (n = 28) of patients reported to have no pain or occasional minimal pain.
CONCLUSIONS:
Posterior pedicle screw-rod fixation is relatively safe, more familiar, and associated with less morbidity. Most of the fractures can be treated by SSF, but in patients with severe vertebral body comminution (AOtype A3) and AO type C fractures, LSF can be done.
Keywords
ASIA impairment scale
pedicle screws
posterior approach
spinal decompression
thoracolumbar spine
TLICS score

Introduction
The spinal fractures occur in 5%–10% of all polytrauma patients and in 4.58% of all trauma patients.[1,2,3] Thoracolumbar fractures are common in the young- and middle-aged males following high-energy blunt trauma injuries sustained after road traffic accidents (40%–50%) and fall from height (20%).[4] Neurological deficit occurs in around 20% of thoracolumbar fractures, and 1-year mortality rate in these patients is about 4%.[5]
The treatment of thoracolumbar fracture has been debated extensively. Operative treatment is considered to provide immediate stability to spine, to correct deformity, and to decompress neural elements either by direct or indirect means. Optimal surgical approach to be used to treat thoracolumbar fractures remains controversial. For this purpose, surgical procedures introduced are performed either through posterior or anterior or combined approaches. Most of the fractures are being treated by posterior fixation; however in case of severe vertebral body comminution, McCormack classification maybe considered for deciding requirement for additional anterior stabilization.[6]
Materials and Methods
This longitudinal study was carried out from August 2018 to July 2021 after obtaining approval from institutional ethical committee.
This study was done to assess the clinicoradiological findings in unstable thoracolumbar spine fractures treated by transpedicular screw-rod fixation procedure.
The sample size (a minimum number of cases required for our study) was calculated as below:

n = 26,
where,
Z = standard deviation set at 1.96 corresponds to 95% confidence interval
p = prevalence of primary outcome, taken as 2.5% (Liu et al.[3])
e = absolute allowable error, taken as 6%.
The patients with thoracolumbar fractures of traumatic etiology with thoracolumbar injury classification and severity (TLICS) score ≥5, unstable fracture with complete or incomplete neurodeficits necessitating neuronal decompression, and spinal stabilization were included in this study, and the patients with age > 60 years, TLICS score ≤ 3, pathological fractures, and who are medically unfit for surgery or not willing for surgery or not willing to give consent to participate in the study were excluded from this study.[7]
Initial management of all spinal injury patients was carried out as per Advanced Trauma Life Support guidelines, neurological examination of the patient using American Spine Injury Association (ASIA) impairment scale, and methylprednisolone therapy as per National Acute Spinal Cord Injury Study 3 protocol.[8,9] X-ray, computerized tomography (CT) scan ± magnetic resonance imaging (MRI) of thoracolumbar spine were done, and TLICS score was calculated. For all patients with TLICS score ≥5, spinal decompression (direct or indirect) and pedicle screw fixation (short segment or long segment) procedures by posterior approach under general anesthesia were done, and a total of 34 patients who underwent this procedure were included in our study. All patients were followed up at 3 weeks, 3 months, 6 months, 1 year, and the last follow-up at 2 years postoperatively, and patients were assessed using x-ray thoracolumbar spine, Denis pain scale, Denis work scale, and Oswestry disability index (ODI).[10,11]
Results
This study includes 34 patients (males = 29 and females = 5) who underwent posterior instrumented fusion for unstable thoracolumbar spine injury. A maximum number of patients were belonged to the age group 31–40 years (44.1%, n = 15) with a mean age of 39.32 years ± 9.78 years. L1 was the most common vertebral level injured (61.8%, n = 21), and flexion distraction injury (Arbeitsgemeinschaft für Osteosynthesefragen [AO] type B2) was the most frequent fracture type (44.1%, n = 15) [Table 1]. Eighteen cases (52.9%) were operated between 2 and 7 days after injury, and 26.5% (n = 9) of patients were operated within 24 h following injury. Associated injuries were seen in 11.76% (n = 4) of patients, which includes fractures of both bones of leg, ribs, calcaneus, distal radius, and fracture dislocation of elbow.
| Parameters | Number of patients Percent | Percent |
|---|---|---|
| Level of vertebral injury | ||
| T11 | 1 | 2.9 |
| T12 | 9 | 26.5 |
| L1 | 21 | 61.8 |
| L2 | 3 | 8.8 |
| AO* fracture type | ||
| A3 | 6 | 17.6 |
| B1 | 3 | 8.8 |
| B2 | 15 | 44.1 |
| C1 | 7 | 20.6 |
| C3 | 3 | 8.8 |
*AO = Arbeitsgemeinschaft für Osteosynthesefragen
Mean duration of surgery of those who underwent short-segment fixation (SSF, n = 19) was 200 ± 14.9 min and that of long-segment fixation (LSF, n = 15) was 258 ± 13.73 min, and mean blood loss during SSF was 410.79 ± 24.96 mL and that during LSF was 653 ± 34.21 mL. Both parameters (surgery duration and blood loss) when compared between SSF and LSF showed statistical significance (P < 0.0001) [Table 2].
| Parameter | SSF* (n = 19) | LSF* (n = 15) | P value | |
|---|---|---|---|---|
| Surgery duration(in min) | Mean | 200 | 258 | <0.0001 |
| SD* | 14.9 | 13.73 | ||
| Blood loss (in mL) | Mean | 410.79 | 653 34.21 | <0.0001 |
| SD* | 24.96 | 34.21 |
*SSF: short segment fixation, †LSF: long segment fixation, ¥SD: standard deviation
Average kyphosis correction obtained by surgery was 10.53°, and the average loss of kyphosis correction at 1 year was 1.69° and at 2 years was 2.94°. At final follow-up, among the patients (n = 28) who sustained spinal cord injury, 85.71% (n = 24) of patients showed improvement to one higher ASIA grade, and patients with residual neurodeficits were 75% (n = 21) [Table 3]. Bowel and bladder were involved in 28 patients (82.4%), out of which 17 patients (60.71%) recovered bowel and bladder function, and a mean duration for recovery was 26.06 ± 24.81 days.
| Cobb angle | Preop | Immediate postop | Postop 1 year | At final follow-up |
|---|---|---|---|---|
| Mean | 20.74 | 10.21 | 11.9 | 13.15 |
| Minimum | 3 | 1 | 3 | 3 |
| Maximum | 40 | 25 | 28 | 30 |
| ASIA grade* | Preop | Postop third week | Postop 1 year | At final follow-up |
| A | 10 | 8 | 3 | 3 |
| B | 10 | 7 | 8 | 6 |
| C | 5 | 8 | 6 | 6 |
| D | 3 | 2 | 6 | 6 |
| E | 6 | 9 | 11 | 13 |
*ASIA grade: American spinal cord injury association grade
Nine patients (26.47%) had postoperative complications. Five patients had urinary tract infection which was the most common complication and bedsore was seen in three patients which was managed by regular dressings. One patient had disseminated intravascular coagulation requiring fresh frozen plasma transfusion and hematoma evacuation by repeat surgery.
At final follow-up, 82.4% (n = 28) of patients reported to have no pain or occasional minimal pain. Fifteen patients (44.1%) were unable to work and were completely disabled, and remaining 19 patients (55.9%) returned to work in previous employment or in a new job either full time or part time [Table 4]. ODI score at final follow-up showed minimal disability in 85.3% (n = 29) of patients and moderate disability in 14.7% (n = 5) of patients. But a majority of our patients were disabled more due to paralysis, which was not considered in ODI score.
| Parameter | Frequency | Percent |
|---|---|---|
| Denis pain scale | ||
| P1 | 11 | 32.4 |
| P2 | 17 | 50 |
| P3 | 6 | 17.6 |
| P4 | 0 | 0 |
| Denis work scale | ||
| W1 | 3 | 8.8 |
| W2 | 7 | 20.6 |
| W3 | 3 | 8.8 |
| W4 | 6 | 17.6 |
| W5 | 15 | 44.1 |
Discussion
Among spinal injury patients, an involvement of thoracolumbar region is very common as it is the transition region. The injuries can have potentially devastating consequences such as neurologic injury.
Even though the evaluation and treatment of thoracolumbar spine fractures have evolved over the past decade, there exists controversies regarding the management of these injuries, viz., which injuries are best treated operatively and nonoperatively; if operative treatment is considered, then the optimal approach that should be used, whether the operative treatment should include direct decompression or indirect decompression.
We observed that thoracolumbar spine injury is common in males belonged to young age, frequently involving L1 vertebra, and these findings are comparable to studies by Basheer et al., Rajaiah et al., and Sen and Patro.[12,13,14] The thoracolumbar spine injuries are usually a result of high-energy trauma. Fall from height was the most common mode of injury, which is similar to studies conducted by several authors.[14,15,16] Associated injuries reported by Basheer et al. were 32%.[12] A less number of patients with associated injuries in our study maybe due to a small sample size.
Many classifications have been proposed for thoracolumbar spine injury and are still evolving. We have used AO classification system for fracture classification, and distraction injury (AO type B2) was the most frequent fracture type observed. Yung and Thng reported burst fracture (AO type A3) and flexion distraction (type B1) injury as common fracture types in their study.[17] Tian et al. reported compression fractures (AO type A) as the most common fracture type of all traumatic spine injuries.[18]
Mean duration from injury to surgery was 5.91 ± 6.55 days and that of Basheer et al. was 11 ± 5.6 days and of Rajaiah et al. was 5.1 days.[12,13] The delay in surgery of our patients was due to late presentation as many are from far-flung areas.
Stancic et al. in their study recommended posterior approach for the decompression and fixation of unstable thoracolumbar fractures because of less blood loss and shorter operating time.[19] Xu et al. in their review article concluded that posterior approach maybe more effective than anterior.[20] In our study, all patients (n = 34) were treated by posterior decompression and pedicle screw fixation.
With posterior approach, adequate neuronal decompression can be carried out by using either indirect or direct or by both methods of decompression combined. The retropulsed fragments in burst fractures can be either removed by direct methods or pushed anteriorly into the native fractured vertebra and difficult to remove fragments can be left behind. There are reports proving the spontaneous remodeling and reconstitution of spinal canal taking place within 12 months after injury, with approximately 50% of retropulsed fragment being resorbed.[21]
In our study, SSF [Figure 1] was done in 19 patients, and LSF [Figure 2] was done in 15 patients. Tezeren and Kuru compared SSF and LSF for thoracolumbar burst fracture in level 2 study and concluded that better correction can be obtained by a long segment than short segment.[22] Dai et al. (level 1) and Alanay et al. (level 2) reported that in SSF, bone grafting was not necessary.[23,24] Tezeren et al. also observed that fusion in LSF did not change clinical or radiological outcomes.[25]
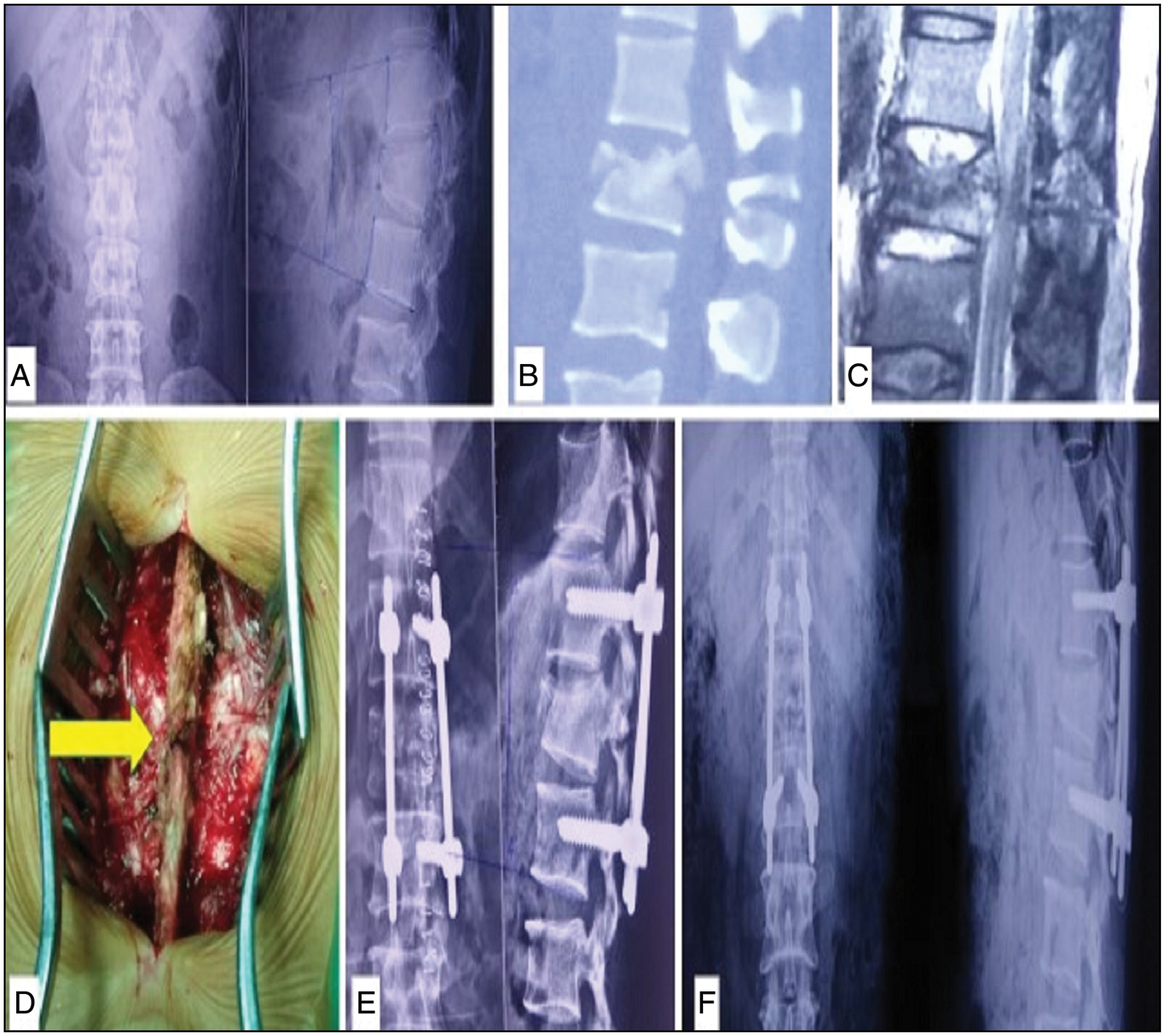
- SSF for AO type B1 fracture. (a) Preoperative x-ray and (b) CT scan images showing the fracture line through L1 vertebral body and its spinous process, (c) MRI scan and (d) intraoperative images showing posterior ligamentous complex (PLC) injury, (e) immediate and (f) final follow-up postoperative x-rays showing in situ pedicle screw-rod construct
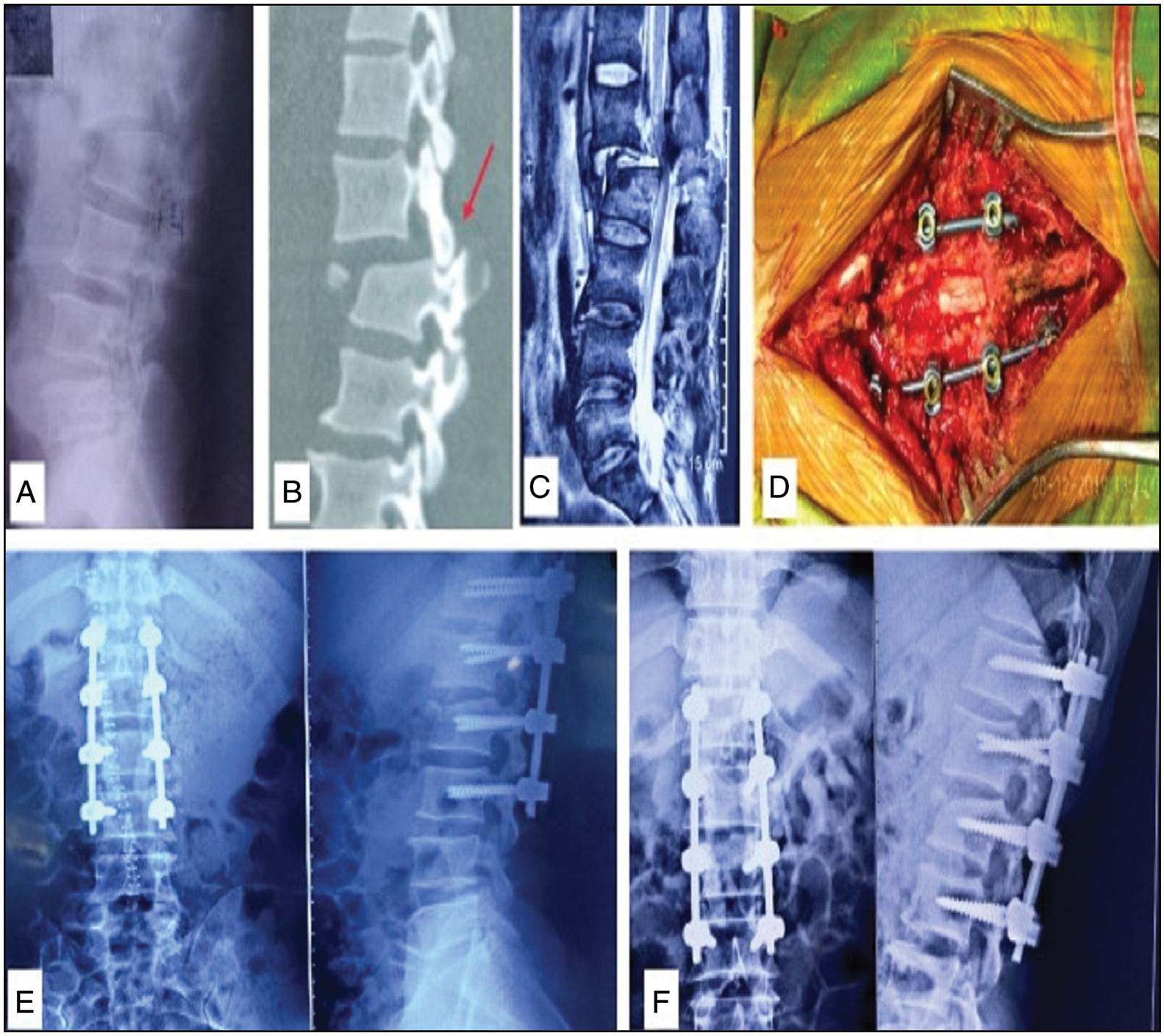
- LSF for AO type C fracture. (a) Preoperative x-ray and (b) CT scan images showing anteriorly translated L1 over L2 with locked dislocated facet, (c) MRI image showing severe canal stenosis between L1 and L2 with injured posterior ligamentous complex (PLC), (d) intraoperative image showing spinal canal decompression by laminectomy with in situ screw-rod construct, (e) immediate postop, and (f) final follow-up x-rays
Postoperative rehabilitation including bowel and bladder care plays a vital role in preventing complications. Basheer et al. reported bed sore in 17.6% of patients. Rajaiah et al. reported complications in six patients (30%), out of which two had bedsores and two had urinary tract infection.[12,13] Jun et al. in their study reported that neurological improvement was seen in 92% of patients.[26] Curt et al. in their study of 70 patients with acute spinal cord injury observed that 27% patients with acute tetraplegia had bladder function recovery and only 10% of patients with acute paraplegia had bladder function recovery.[27]
In our study, one screw in a patient had breached medial cortex of the pedicle, which was seen in repeat CT scan [Figure 3]. The repeat surgery was done the next day and the malpositioned screw removed and changed to normal trajectory. Screw malposition rate was not calculated in our study, as repeat CT scan was not done routinely in all postoperative patients.
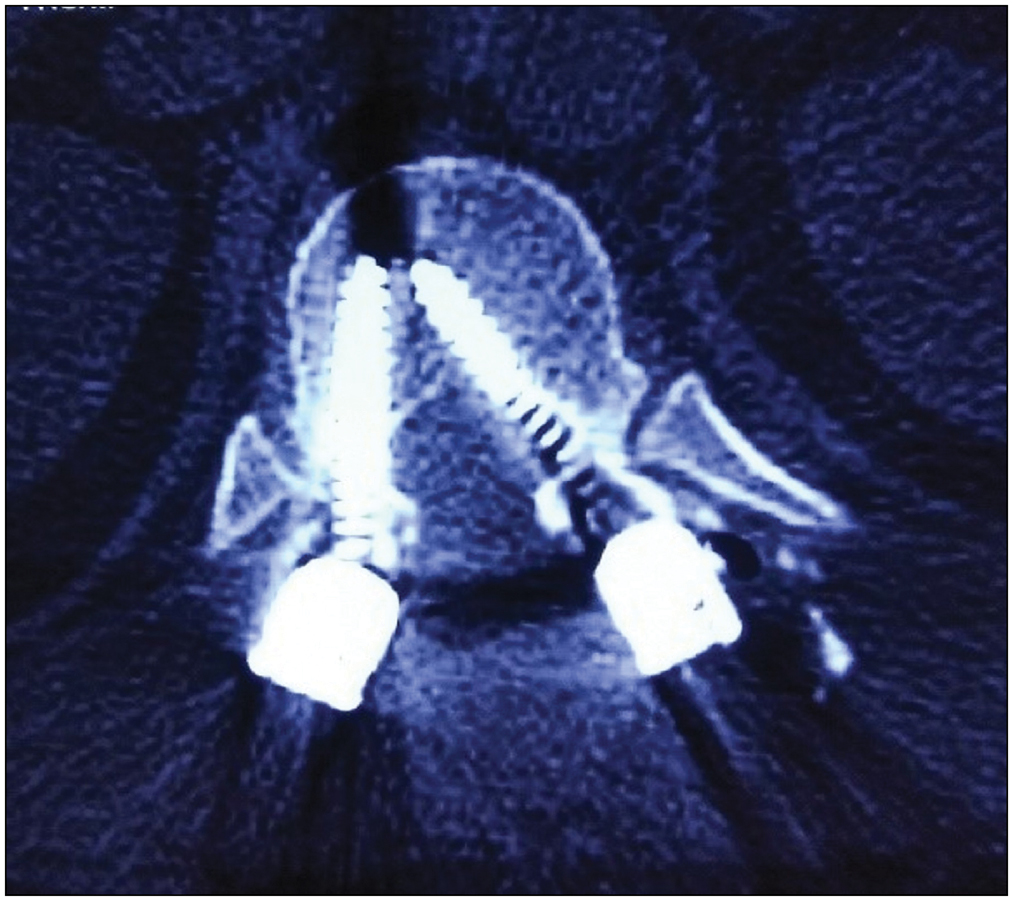
- Axial CT image showing breach in medial cortex of the left pedicle
Loss of correction and failure of fixation are very important complications. Gaines et al. in their study of 52 patients with thoracolumbar fractures treated by pedicle screws observed a loss of correction of more than 5° in 10 patients out of which eight patients had more than 10°. The loss of correction was attributed to failure of fixation by bending or breakage of screw, screw pullout.[28] Carl et al. reported in their study that average kyphosis correction was 7.3°, and an average loss of correction during follow-up was 6.5°.[16] After 2 years of follow-up, we did not encounter any screw breakage or instrumentation failure.
In Andalib et al. study, operative group (n = 21) showed that 16 patients (76.2%) reported to have no pain or occasional pain and five patients (23.8%) reported moderate pain, whereas in nonoperative group (n = 28), 71.5% of patients had no pain or occasional pain and 10.7% patients had moderate-to-severe pain.[29] The study of thoracolumbar burst fractures by Sadatsune et al. reported that out of 27 patients, five were free from pain, 11 had minimal pain not requiring medications, and 10 patients had moderate pain requiring occasional use of medications.[30]
In Andalib et al. study, in nonoperative group, 42.8% (n = 12) were unemployed, nine of these (32.1%) were capable of working and three patients (10.7%) were disabled and couldn’t work.[29] Sadatsune et al. observed that out of 21 patients with burst fracture, eight had returned to heavy work, six had returned to sedentary work without any restriction, nine had returned to work but with some limitations, and two had returned to work part time.[30]
At final follow-up, 64.7% (n = 22) were able to walk and 35.3% (n = 12) were wheel chair bound. Among those who can walk, patients requiring support were 14.7% (n = 5) and who can walk without support were 50% (n = 17). Eleven patients were still voiding through urinary catheterization.
Limitations of our study are small sample size, CT scan was not done routinely in all postoperative patients, and ODI scale when used during follow-up assessment showed minimal disability in a majority of patients, but they were disabled more due to neurodeficit.
Conclusions
Thoracolumbar spine fractures can cause potentially devastating consequences including neurologic injury, chronic pain, and varying degrees of disability. The stabilization of unstable spine helps in early mobilization, prevention or correction of deformity, and early neuro-rehabilitation, thereby preventing complications of prolonged recumbence.
All our patients were treated by posterior pedicle screw-rod fixation as it is relatively safe, more familiar, and associated with less morbidity compared with anterior approach. Pedicle screw obtained three-column fixation allowing stable control of vertebra in axial, coronal, and sagittal planes during reduction maneuvers, intraoperative deformity correction.
Most of the fractures can be treated by SSF, but in patients with severe vertebral body comminution (AO type A3) and AO type C fractures, LSF can be done. LSF also negates a need for grafting and fusion procedures.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Epidemiology and predictors of spinal injury in adult major trauma patients: European cohort study. Eur Spine J. 2011;20:2174-80.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of traumatic spinal fractures: Experience from medical university-affiliated hospitals in Chongqing, China, 2001-2010. J Neurosurg Spine. 2012;17:459-68.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal trauma in Mainland China from 2001 to 2007: An epidemiological study based on a nationwide database. Spine (Phila Pa 1976). 2012;37:1310-5.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal cord injury (SCI)—Prehospital management. Resuscitation. 2005;66:127-39.
- [CrossRef] [PubMed] [Google Scholar]
- Life expectancy after spinal cord injury: A 50-year study. Spinal Cord. 2012;50:803-11.
- [CrossRef] [PubMed] [Google Scholar]
- The load sharing classification of spine fractures. Spine (Phila Pa 1976). 1994;19:1741-4.
- [CrossRef] [PubMed] [Google Scholar]
- The thoracolumbar injury severity score: A proposed treatment algorithm. J Spinal Disord Tech. 2005;18:209-15.
- [Google Scholar]
- International Standards for Neurological Classification of spinal cord injury (revised 2011) J Spinal Cord Med. 2011;34:535-46.
- [CrossRef] [PubMed] [Google Scholar]
- Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. Results of the third national acute spinal cord injury randomized controlled trial. National Acute Spinal Cord Injury Study. JAMA. 1997;277:1597-604.
- [CrossRef] [PubMed] [Google Scholar]
- Acute thoracolumbar burst fractures in the absence of neurologic deficit. A comparison between operative and nonoperative treatment. Clin Orthop Relat Res. 1984;189:142-9.
- [CrossRef] [Google Scholar]
- The Oswestry disability index. Spine (Phila Pa 1976). 2000;25:2940-52. discussion 2952.
- [CrossRef] [PubMed] [Google Scholar]
- Unstable dorsolumbar fractures: A prospective series of 94 cases. Indian J Neurotrauma. 2010;7:55-9.
- [CrossRef] [Google Scholar]
- A study of clinical and radiological outcome in dorsolumbar spine fractures stabilised by pedicle screw fixation. J Evid Based Med Healthc. 2017;4:3672-5.
- [CrossRef] [Google Scholar]
- Management of unstable spine fracture with segmental spinal instrumentation (VSP system): Result at 5 years follow up. Indian J Orthop. 2005;39:232-6.
- [CrossRef] [Google Scholar]
- Late results of thoracolumbar fractures after posterior instrumentation and transpedicular bone grafting. Spine (Phila Pa 1976). 2001;26:88-99.
- [CrossRef] [PubMed] [Google Scholar]
- Pedicle screw instrumentation for thoracolumbar burst fractures and fracture dislocations. Spine (Phila Pa 1976). 1992;17:S317-24.
- [CrossRef] [PubMed] [Google Scholar]
- Radiological outcome of short segment posterior stabilisation and fusion in thoracolumbar spine acute fracture. Ann Acad Med Singap. 2011;40:140-4.
- [CrossRef] [PubMed] [Google Scholar]
- Age- and gender-specific clinical characteristics of acute adult spine fractures in china. Int Orthop. 2016;40:347-53.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior decompression and fixation versus posterior reposition and semirigid fixation in the treatment of unstable burst thoracolumbar fracture: Prospective clinical trial. Croat Med J. 2001;42:49-53.
- [Google Scholar]
- Anterior versus posterior approach for treatment of thoracolumbar burst fractures: A meta-analysis. Eur Spine J. 2013;22:2176-83.
- [CrossRef] [PubMed] [Google Scholar]
- Conservative treatment of fractures of the thoracic and lumbar spine. Orthop Clin North Am. 1986;17:161-70.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior fixation of thoracolumbar burst fracture: Short-segment pedicle fixation versus long-segment instrumentation. J Spinal Disord Tech. 2005;18:485-8.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures: A five to seven-year prospective randomized study. J Bone Jt Surg—Ser A. 2009;91:1033-41.
- [CrossRef] [PubMed] [Google Scholar]
- Short-segment pedicle instrumentation of thoracolumbar burst fractures: Does transpedicular intracorporeal grafting prevent early failure? Spine (Phila Pa 1976). 2001;26:213-7.
- [CrossRef] [PubMed] [Google Scholar]
- Long segment instrumentation of thoracolumbar burst fracture: Fusion versus nonfusion. J Back Musculoskelet Rehabil. 2009;22:107-12.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior direct decompression and fusion of the lower thoracic and lumbar fractures with neurological deficit. Asian Spine J. 2011;5:146-54.
- [CrossRef] [PubMed] [Google Scholar]
- Recovery of bladder function in patients with acute spinal cord injury: Significance of Asia scores and somatosensory evoked potentials. Spinal Cord. 1997;35:368-73.
- [CrossRef] [PubMed] [Google Scholar]
- Current concepts review: The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. JBJS Am. 1984;82-A:1458-76.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of functional and radiographic outcomes of thoracolumbar fractures. Glob Spine J. 2016;6(1_suppl) s-0036-1583157
- [CrossRef] [Google Scholar]
- Thoracolumbar burst fracture: Correlation between kyphosis and function after surgical treatment. Rev Bras Ortop. 2012;47:474-8.
- [CrossRef] [Google Scholar]




