
Translate this page into:
Comparison between fluoroscopy-guided radiofrequency ablation of genicular nerves and intra-articular injection of steroid in relieving pain and improving function among candidates of knee replacement surgery: A randomized controlled trial
Address for correspondence: Dr. Kanti Rajkumari, Department of Physical Medicine & Rehabilitation, Churachandpur Medical College, Churachandpur 795128, Manipur, India. E-mail: kantiaarkay@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Chabungbam M, Singh AJ, Singh LN, Pilania C, Choorapra S, Swami T, et al. Comparison between fluoroscopy-guided radiofrequency ablation of genicular nerves and intra-articular injection of steroid in relieving pain and improving function among candidates of knee replacement surgery: A randomized controlled trial. J Orthop Spine 2022;10:35-9.
Abstract
BACKGROUND:
Osteoarthritis (OA) is the second most common rheumatologic problem in India. Prevalence of OA in India is 22–39% and knee OA alone contributes to 80% of OA burden. Despite the immense impact of this disease, very few effective non-surgical treatment options are available. The present study aims to compare fluoroscopy-guided radiofrequency ablation (RFA) of genicular nerves with intra-articular (IA) injection of methylprednisolone acetate in relieving pain and improving function in Grade 3 and 4 OA of knee.
MATERIALS AND METHODS:
A randomized controlled trial was done in the Department of Physical Medicine and Rehabilitation, Regional Institute of Medical Sciences for a period of 1 year on 76 patients with knee OA Kellgren–Lawrence (KL) grade 3 and 4. They were divided into two groups: study and control groups. The study group underwent RFA of genicular nerves of knee, whereas the control group received IA knee injection with methylprednisolone acetate 80 mg. Assessments of Visual Analog Scale (VAS) and Western Ontario McMaster University Osteoarthritis Index (WOMAC) were done at 1, 4, and 12 weeks.
RESULTS:
The study group showed a decrease in VAS score from 6.84 ± 0.638 at baseline to 2.61 ± 0.718 at 1 week and 2.97 ± 0.885 at 12 weeks. The control group showed a decrease in VAS score from 5.82 ± 0.563 at baseline to 2.18 ± 0.393 at 1 week and 4.03 ± 0.545 at 12 weeks. WOMAC function score improved from 44.79 ± 7.185 at baseline to 26.79 ± 4.375 at 12 weeks in the RFA group, whereas in the steroid group it improved from 41.26 ± 5.310 at baseline 24.89 ± 3.431 at 12 weeks (P<0.05).
CONCLUSION:
RFA of genicular nerve can be used as an effective modality for providing cost-effective and long-standing pain relief in patients with KL Grade 3 and 4 OA knee who are unable to undergo knee replacement surgery.
Keywords
Kellgren–Lawrence grade
osteoarthritis
radiofrequency ablation
WOMAC

Introduction
Osteoarthritis (OA) is a destructive joint failure, a condition in which all structures in the joint have undergone a pathologic change, often in concert. OA is the second most common rheumatologic problem in India. Prevalence of OA in India is 22–39% and knee OA alone contributes to 80% of OA burden. Despite the immense impact of this disease, very few effective non-surgical options are available to handle it.[1,2] Management of pain in knee OA requires a combination of non-pharmacologic and pharmacologic options such as non-steroidal anti-inflammatory drugs and intra-articular (IA) steroids or visco-supplementation. However, these drugs are associated with potential safety concerns, short half-life, and cost issues.[3] Newer, cost-effective non-surgical options to counteract the knee pain and improve function have always been of interest to physiatrists and pain physicians alike with radiofrequency ablation (RFA) of genicular nerves of knee being the most recent.
The knee joint receives sensory innervation from branches of the obturator, femoral, tibial, and common fibular nerve. There are a total of six genicular nerves with pure sensory supply. These are genicular branches from the tibial (superomedial, inferomedial, and middle genicular nerve) and common fibular nerves (superolateral, inferolateral, and recurrent genicular nerve). RFA uses a high frequency alternating current to generate heat that will cause thermal injury to genicular nerves. An electrode is placed on the target nerve and thermocoagulation induces tissue destruction by producing heat up to 60–80°C.[4,5]
Till date, no comparison study has been done between IA knee with methylprednisolone acetate and RFA genicular nerves in chronic OA knee patients who are candidates for knee replacement surgery, i.e., with KL grades 3 and 4. The present study tries to see the efficacy of RFA over the wonder drug “steroid” in reducing pain and delaying surgery in severe knee pain of OA.
Materials and Methods
A randomized controlled trial was done in the Department of Physical Medicine and Rehabilitation, Regional Institute of Medical Sciences for a period of 1 year starting from March 2019. Patients diagnosed with KL grade 3 and 4 OA knee were recruited for the study from the OPD patients. Informed consent was taken from all participants before starting the study.
Patients with OA of knee as per 2016 revised ACR criteria for early diagnosis of OA and those with radiologic tibiofemoral OA (KL grades 3 an d4) with positive diagnostic block (>50% improvement in pain) were included in the study.
Patients with bilateral OA knee of grade 3 or more, prior knee surgery/injury, arthritis due to other causes, serious neurologic/psychiatric disorder, injection with steroids/hyaluronan in the last 3 months, on pacemaker, uncontrolled diabetes, coagulation disorder, Visual Analog Scale (VAS) score <5, local or systemic infection, allergy to anesthetic medication used, uncooperative patients were excluded from the study.
Sample size
The sample size was calculated using the formula

where u = 0.84, at 80% power (1–β),
v = 1.96 at 5% level of significance (α).
Taking into consideration, Jain and Jain[6] study titled comparison of efficacy of methylprednisolone and triamcinolone in OA of the knee; we took
m1 (mean VAS score in the control group) = 5.61,
m2 (mean VAS score in the study group) = 6.30,
s1 (standard deviation of VAS score in the control group) = 1.12,
s2 (standard deviation of the study group) = 1.03.
Therefore,

Hence, 38 patients were studied per group giving a total of 76 patients.
The 76 eligible participants were assigned randomly to two groups: study and control groups using the block method. Since there are two treatment options involved, block size of four was used. Possible treatment allocations within each block are (1) AABB, (2) BBAA, (3) ABAB, (4) BABA, (5) ABBA, and (6) BAAB. Using random number table, a list of blocks was used. For each selected block, there was a sequence of treatment options. The sequence of treatment options was put in a sealed envelope and corresponding envelopes were labeled 1, 2, 3, 4,…, according to the appearance in the list. The sealed envelope with label 1 was opened only when we had the first eligible patient and the treatment was allocated. This continued till the required sample was enrolled. Allotment of numbers and patient enrollment were done by an OT nurse not involved in the procedure.
The study group underwent continuous RFA of superolateral, superomedial, and inferomedial genicular nerves under fluoroscopic guidance following a successful diagnostic block (>50% improvement in pain within 2–4 h) of genicular nerves with 2% lignocaine.
The patient was positioned supine with knee slightly flexed by keeping a pillow underneath. Under C-arm guidance, bony landmarks of the knee where shaft of femur and tibia meets their condyles were identified [Figure 1]. Under strict aseptic and antiseptic conditions, 22G RF cannula with 10 mm active was inserted perpendicular to the skin at these three points until bone contact was made [Figure 2]. After hitting bone, stylet was removed and RF probe was inserted. To confirm the sensory nerve position, stimulation was done with 50 Hz at 0.3–0.5 V. In order to avoid motor nerve ablation, it was made sure that no fasciculation of lower limb muscles occur by stimulation with 2 Hz at 1 V.
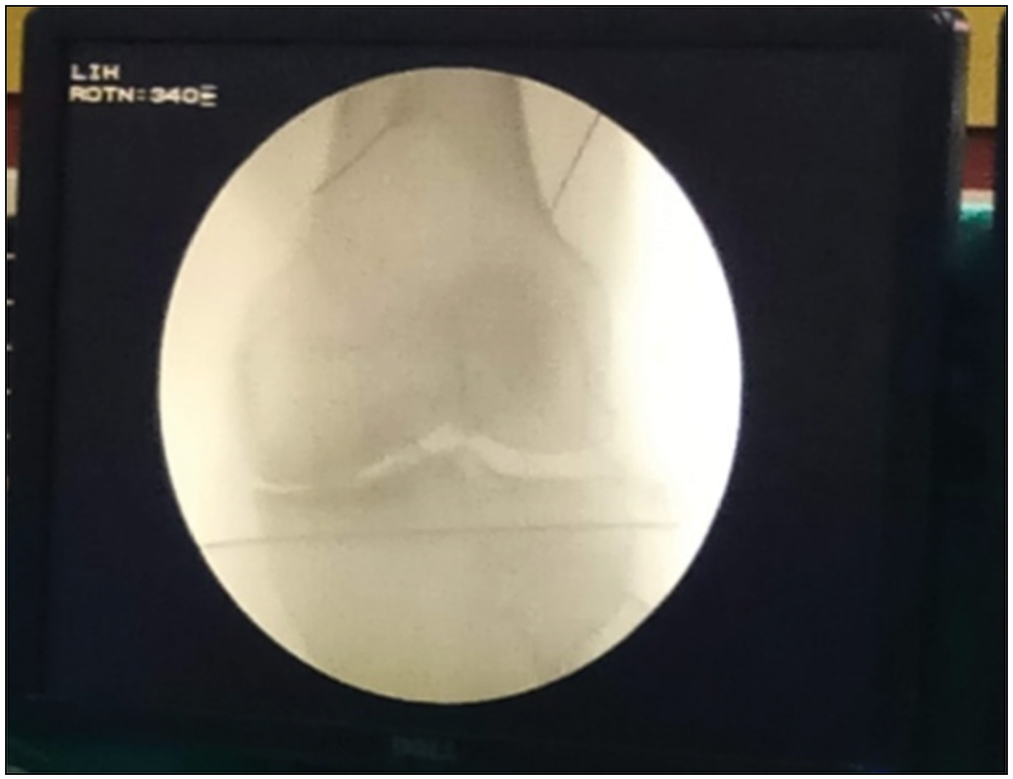
- Fluoroscopic image in AP view showing RF cannula placement at the junction of shaft of femur with the femoral condyles where the superomedial and superolateral genicular nerves traverse
![Placement of 22G RF cannula at superolateral, superomedial, and inferomedial genicular nerves followed by insertion of RF probes to confirm needle position at the target nerves by sensory stimulation (50 Hz at 0.3–0.5 V) and to avoid motor nerve ablation (stimulation with 2 Hz at 1 V). Continuous RF ablation of the three genicular nerves is then done at 70°C for 90 min, as shown in [Figure 3]](/content/178/2022/10/1/img/JOAS-10-35-g004.png)
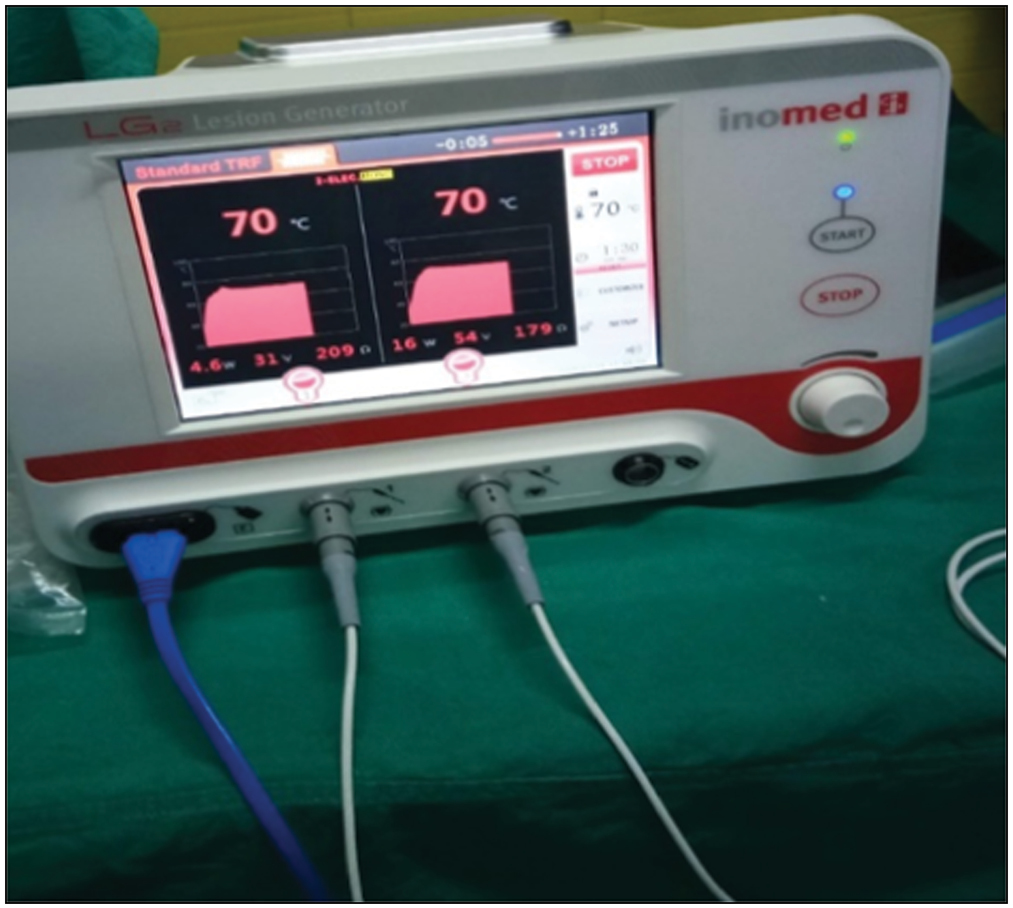
- Placement of 22G RF cannula at superolateral, superomedial, and inferomedial genicular nerves followed by insertion of RF probes to confirm needle position at the target nerves by sensory stimulation (50 Hz at 0.3–0.5 V) and to avoid motor nerve ablation (stimulation with 2 Hz at 1 V). Continuous RF ablation of the three genicular nerves is then done at 70°C for 90 min, as shown in [Figure 3]
An aliquot of 1 mL of 2% lignocaine was given at these sites before starting the lesion. RF lesion was performed over 90 s with temperature raised to 70–75°C. One RF lesion was made for each genicular nerve [Figure 3].
- Image shows RFA of two Genicular nerves being performed simultaneously using unipolar two electrodes
The control group received IA knee injection with methylprednisolone acetate 80 mg. The patient was placed in the sitting position with knees flexed to 90°. The patellar tendon was palpated and the middle of the patellar tendon was marked. The patient was prepared in a standard aseptic and antiseptic fashion over an area large enough to allow palpation of landmarks, and a sterile technique was used throughout the procedure. A 21G needle was inserted horizontally and advanced to the intercondylar notch and injected with 2 mL of 80 mg of methylprednisolone acetate and local anesthetic.
Follow-up assessments were done at 1, 4, and 12 weeks post procedure to see changes in pain and function using the primary and secondary outcome variables VAS and WOMAC, respectively.
Statistical analysis
Analysis was done using Statistical Package for the Social Sciences, SPSS 21 version. For descriptive statistics, mean and standard deviation were used. For analytical statistics, paired t-test, independent t-test and analysis of variance were used for numerical data; and the χ2 test was used for categorical data. P-value less than 0.05 was taken as significant. Clinical trial registration no.: CTRI/2019/10/021626.
Results
There was no drop out from the study or cases lost to follow-up in the study. All 76 patients were followed up till 12 weeks [Figure 4]. Only one case of knee hematoma was reported following RFA knee in the study; otherwise, no adverse effects were reported during the study.
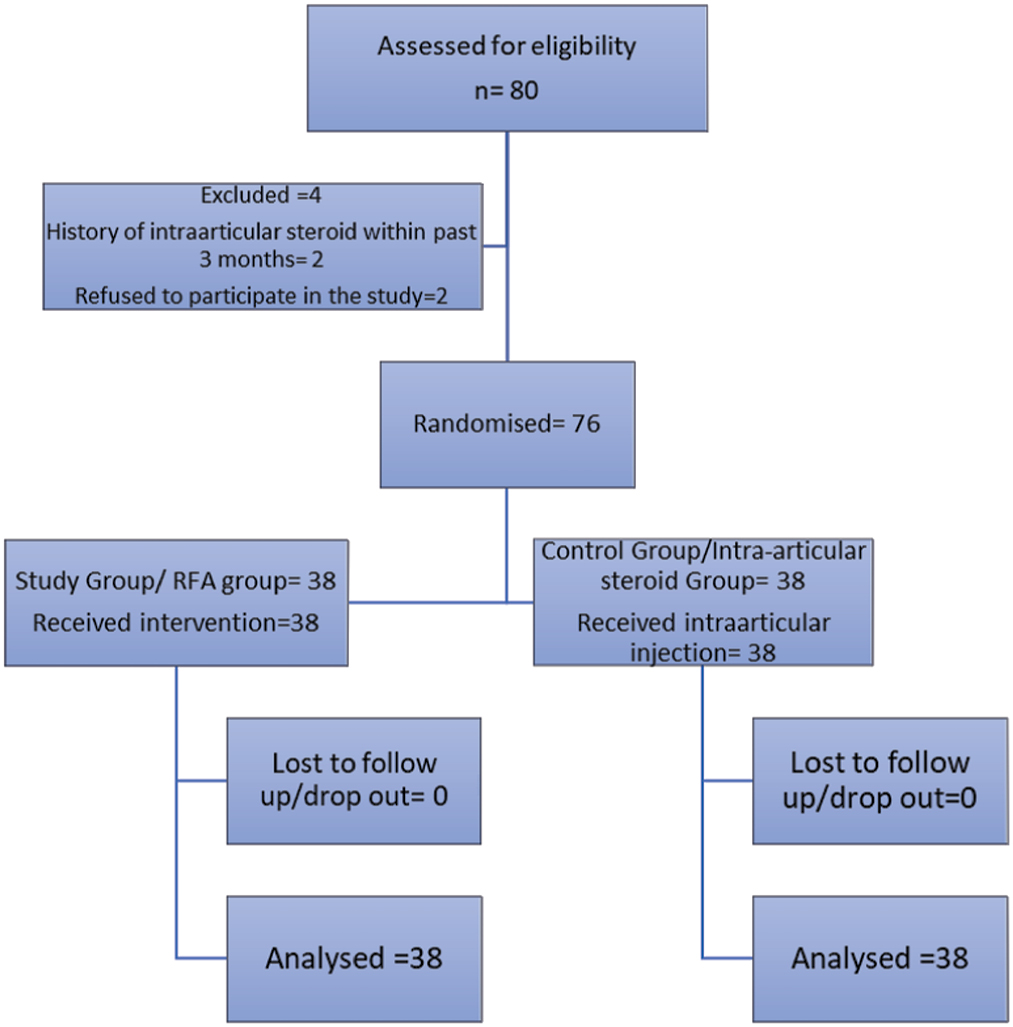
- CONSORT flowchart of recruitment and allotment of participants
Table 1 shows that there is no statistical differences in the baseline characteristics between the groups. Tables 2 and 3 show significant improvement in both VAS and WOMAC in both the groups during all follow-ups; however improvement in pain and function was more in the RFA group than in the steroid group.
| Characteristics | Group | P-value | |
|---|---|---|---|
| Study (n, %) | Control (n, %) | ||
| Age (years) | 65.26 ± 6.85 | 58 ± 8.94 | 0.385 |
| 41–50 | 3 (50) | 3 (50) | |
| 51–60 | 10 (37) | 17 (63) | |
| 61–70 | 17 (56.7) | 13 (43.3) | |
| 71–80 | 8 (61.5) | 5 (38.5) | |
| Sex | 0.574 | ||
| Male | 7 (43.8) | 9 (56.2) | |
| Female | 31 (51.7) | 29 (48.3) | |
| Place of residence | 0.361 | ||
| Plain area | 33 (52.4) | 30 (47.6) | |
| Hilly area | 5 (38.5) | 8 (61.5) | |
| Side of knee OA | 0.226 | ||
| Right side | 28 (56.0) | 22 (44.0) | |
| Left side | 10 (38.5) | 16 (61.5) | |
| Kellgren–Lawrence grading | 0.637 | ||
| Grade 4 | 13 (44.8) | 16 (55.2) | |
| Grade 3 | 25 (53.2) | 22 (46.8) | |
| Duration of knee OA | 0.448 | ||
| <1 year | 2 (50.0) | 2 (50.0) | |
| 1–3 years | 18 (43.9) | 23 (56.1) | |
| >3–5 years | 12 (52.2) | 11 (478) | |
| >5 years | 6 (75.0) | 2 (25.0) | 0.227 |
| VAS score | 0.227 | ||
| Mild (1–3) | 4 (40.0) | 6 (60.0) | |
| Moderate (4–6) | 18 (43.9) | 23 (56.1) | |
| Severe (7–9) | 16 (64.0) | 9 (36.0) | |
| Parameters | Groups mean (SD) | P-value* | |
|---|---|---|---|
| Study (n=38) | Control (n=38) | ||
| VAS scores | 0.001 | ||
| Baseline | 6.84 ± 0.638 | 5.82 ± 0.563 | |
| 1 week | 2.61 ± 0.718 | 2.18 ± 0.393 | |
| 4 weeks | 2.61 ± 0.718 | 2.18 ± 0.393 | |
| 12 weeks | 2.97 ± 0.885 | 6.03 ± 0.545 | |
| Parameters | Groups mean (SD) | P-value* | |
|---|---|---|---|
| Study (n=38) | Control (n=38) | ||
| Total WOMAC scores | |||
| Baseline | 59.47 ± 7490 | 4792 ± 6.780 | 0.001 |
| 1 week | 33.95 ± 5.146 | 35.58 ± 3.561 | |
| 4 weeks | 30.32 ± 3.480 | 31.34 ± 3.257 | |
| 12 weeks | 22.13 ± 4.783 | 28.03 ± 4.365 | |
*P-value <0.05 is taken as significant
Discussion
To our knowledge, this is the first study in which the effect of conventional RFA of genicular nerves was tried in severe grades of OA—KL grade 3 and 4 OA, who were candidates for knee replacement surgery. For many years, knee replacement was thought to be the only option to reduce pain in such severe grades of OA knee. However, few drawbacks of surgery are: many have recurrence of pain following the surgery, many are physically not fit to undergo surgery, and full knee ROM cannot be achieved with knee arthroplasty.
Sarı et al.[7] first compared RFA with IA injections in a trial. Seventy-three patients with at least grade 2 KL OA were randomized to receive either RFA of the SL, SM, and IM genicular nerves at 80°C for 90 s or IA injection of bupivacaine, morphine, and betamethasone. Results obtained were in favor of RFA in terms of VAS.
Qudsi-Sinclair et al.[8] in a trial with 28 participants with knee pain following total knee replacement evaluated between traditional radiofrequency (n = 14) or local anesthetic and corticosteroid block of genicular nerves in the knee (n = 14). They found similar results with both.
Davis et al.[9] conducted the largest study on RFA knee. One hundred and fifty patients with at least KL grade 2 were randomized to receive either conventional RFA (C-RFA) or intra-articular steroid (IAS) injection. Pain relief with C-RFA was superior to that obtained with IAS at all time periods.
El-Hakeim et al.[10] compared RFA with oral drugs: acetaminophen and diclofenac. Patients were evaluated at baseline, 2 weeks, 3 months, and 6 months. Results showed statistically superior pain relief with RFA at all follow-up intervals. Patient satisfaction as measured on a Likert scale was significantly higher at 3 and 6 months follow-up in the RFA group.
The above studies are in concert with the findings of the present study in which we found that both RFA of genicular nerves and IASs can result in significant reduction of pain with improvement in function in grade 3 and 4 OA knee. However, at 12 weeks, effect of steroids starts wearing off with increase in VAS from 2.18 ± 0.393 at 4 weeks to 6.03 ± 0.545 at 12 weeks, whereas in the RFA group the pain relief achieved at 1 week was sustained till 12 weeks.
It can thus be concluded that RFA of genicular nerve provides longer and sustained pain relief in grade 3 and 4 OA knee than IAS. It can hence be used as an effective modality for managing severe pain and delaying surgery in knee OA patients. They can be a boon for those who are unfit for knee replacement surgery, unwilling to undergo surgery, or who have recurrence of pain following knee replacement surgery.
Lack of larger sample size, lack of blinding, short-term follow-up, hospital-based study, and evaluation based totally on questionnaire were some of the limitations in the study. Frequency of RFA of genicular nerves required or allowed in a year, treatment cost comparison with steroid, and late sequelae of RFA on knee joint are some important areas that could not be assessed in the present study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Osteoarthritis. In: Fauci S, Kasper L, Longo DL, Joseph L, Larry J, Stephen L, eds. Harrison’s Principles of Internal Medicine (18th). New York: McGraw-Hill; 2008. p. :2828-36.
- [Google Scholar]
- Prevalence of knee osteoarthritis patients in Mysore city Karnataka. Int J R Sci. 2015;6:3316-20.
- [Google Scholar]
- Clinical Practice Guideline: Treatment of osteoarthritis of the knee: Evidence-based guideline. J Am Acad Orthop Surg. 2013;21:577-9.
- [CrossRef] [PubMed] [Google Scholar]
- Radiofrequency treatment relieves chronic knee osteoarthritis pain: A double-blind randomized controlled trial. Pain. 2011;152:481-7.
- [CrossRef] [PubMed] [Google Scholar]
- Osteoarthritis. In: Frontera WR, Delisa JA, Bruce M, Nicolas E, Lawrence R, Jeffrey R, eds. Delisa’s Physical Medicine and Rehabilitation (5th). Philadelphia: Lippincott Williams and Wilkins; 2010. p. :781-809.
- [Google Scholar]
- Comparison of efficacy of methylprednisolone and triamcinolone in osteoarthritis of the knee: A prospective randomized double blind study. Int J Sci Stud. 2015;3:58-62.
- [Google Scholar]
- Kurt Ömürlü İ Which one is more effective for the clinical treatment of chronic pain in knee osteoarthritis: Radiofrequency neurotomy of the genicular nerves or intra-articular injection? Int J Rheum Dis. 2018;21:1772-8.
- [Google Scholar]
- comparison of genicular nerve treatment using either radiofrequency or analgesic block with corticosteroid for pain after a total knee arthroplasty: A double-blind randomized clinical study. Pain Pract. 2017;17:578-88.
- [CrossRef] [PubMed] [Google Scholar]
- Prospective, multicenter, randomized, crossover clinical trial comparing the safety and effectiveness of cooled radiofrequency ablation with corticosteroid injection in the management of knee pain from osteoarthritis. Reg Anesth Pain Med. 2018;43:84-91.
- [CrossRef] [PubMed] [Google Scholar]
- Fluoroscopic guided radiofrequency of genicular nerves for pain alleviation in chronic knee osteoarthritis: A single-blind randomized controlled trial. Pain Physician. 2018;21:169-77.
- [CrossRef] [Google Scholar]




