
Translate this page into:
Effect of ultrasound-guided pes anserine bursa injection on knee scores: A comparative study
Address for correspondence: Dr. Richa, Room 421, All India Institute of Physical Medicine and Rehabilitation (AIIPMR), Haji Ali, Mumbai 400 034, Maharashtra, India. E-mail: richajjn@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Choudhary M, Richa, Gupta S, Gaur AK. Effect of ultrasound-guided pes anserine bursa injection on knee scores: A comparative study. J Orthop Spine 2022;10:24-9.
Abstract
INTRODUCTION:
Pes anserine bursitis is a common clinical finding in patients with knee osteoarthritis. This causes significant disability and functional hindrance. Management includes medication, physiotherapy, and local steroid injection. Though many studies have been done in relation to the management of pes anserine bursitis, a comparative study for two techniques of giving local steroid injection is the first of its kind.
AIM:
The aim of this study was to compare the effect of ultrasound-guided versus blind corticosteroid injection in pes anserine bursa.
MATERIALS AND METHODS:
A total of 84 patients (comprising 100 injection limbs) attending the outpatient department of Physical Medicine and Rehabilitation at a tertiary care center were selected. Detailed demographic data were collected and each patient was examined clinically. American College of Radiology clinical classification criteria for knee osteoarthritis were used to diagnose knee osteoarthritis. All the patients were injected with methylprednisolone 80 mg (2 mL), half of them under ultrasound guidance and the other half by clinical judgment. All the study participants were evaluated using a visual analog scale (VAS) score and knee injury and osteoarthritis outcome score (KOOS), pre-procedure and post-procedure at 1 week, 1 month, and 3 months, to assess pain and the functional improvement using paired t test for intra-group and unpaired t test for inter-group comparison.
RESULTS:
Both the groups with comparable baseline assessment showed a significant improvement in the VAS score after the injection at 1 week, 1 month, and 3 months duration. Also, there was a significant improvement in the functional status in patients of both groups as indicated by the KOOS after the injection at 1 week, 1 month, and 3 months duration. However, there was no statistically significant difference in the outcome measured on VAS score with the two techniques. This implies that both techniques led to comparable VAS outcomes statistically. However, the functional outcome as indicated by KOOS score was significantly higher in the group injected under ultrasound guidance.
CONCLUSION:
KOOS assessment indicated that ultrasound-guided injection technique is superior to the blind technique. On the basis of the VAS score, no statistically significant difference was found in outcomes using the two different techniques.
Keywords
Function
local corticosteroid
pain
rehabilitation

Introduction
The term “pes anserinus” (Latin for goose foot) refers to the common insertional tendon of sartorius, gracilis, and semitendinosus muscles on the anteromedial surface of the proximal tibia. As these three tendons approach their insertion site, they come together to form a conjoined tendon that anatomically resembles a goose’s webbed foot, which inserts 5–6 cm inferior to the knee along the anteromedial surface of the tibia.[1] The pes bursa is a synovial lined sac that lies deep to the pes anserinus and superficial to the tibial attachment of the medial collateral ligament. It does not communicate with the knee joint.[2,3,4]
The pes anserine bursa can often be the source of discomfort in patients experiencing knee pain.[5,6] On the basis of their study, Yoon et al.[7] reported that pes anserine bursitis had been clinically diagnosed in 46.8% of the patients with knee osteoarthritis (OA). In contrast, 83.3% of pes anserine bursitis or tendinitis patients were reported to have radiographic evidence of knee OA.
The hallmark features of pes anserine bursitis are knee pain, a palpable swelling of bursa, and tenderness over medial anterior aspect of tibia just below knee.[2,8,9] Patients typically present with knee pain, which is aggravated by climbing or descending stairs.
Inflammation of the anserine bursa has been attributed to excess valgus or rotatory stress causing increased friction and contusion of the bursa.[4] Chronic pes anserine bursitis is often reported in patients with underlying degenerative joint disease or rheumatoid arthritis. The incidence of pes anserine bursitis is higher in females, overweight patients, individuals with OA of the knee, valgus deformity and pes planus, and those of 50–80 years of age, although younger obese women can also be affected.[4,7] Women seem to be more predisposed to anserine bursitis because of the broad pelvic area, with resultant angulation at the knee joint, putting more pressure at the pes anserinus attachment.[5,10,11,12]
Ultrasound-guided technique enables the clinician to visualize as well as inject steroid into the bursal substance with better precision whereas in the blind technique the tender spot is clinically appreciated and injected. Hence, with the blind technique, the placement of injection into bursal sac cannot be ensured.
There have been studies on the management of pes anserine bursal pain using various modalities including diclofenac mesotherapy, polydeoxyribonucleotide, and physiotherapy. However, there are not enough studies in the literature regarding steroid injection given by the two techniques in pes anserine bursa. As the availability of ultrasound machines can limit the number of patients in whom the injection can be given by direct visualization, this study aims to explore whether such direct visualization has any added benefit in the first place.
In a similar study conducted on sample size of 47 patients, it was shown that ultrasound-guided pes anserine bursa injection was more accurate than blind technique as assessed by VAS scale, at 1 week and 4 weeks after the injection. However, this study had the limitations of small sample size and a short follow-up of 4 weeks which is lesser than the time advocated for the achievement of optimum outcome of the local corticosteroid injection.[13]
Another previous similar study conducted in lateral epicondylitis comparing the two techniques has shown that the ultrasound guidance for corticosteroid injection does not improve clinical outcome as compared with the injection given by blind technique.[14]
Materials and Methods
This was a randomized controlled clinical study conducted in the Department of Physical Medicine and Rehabilitation at a tertiary care center from October 2017 to December 2018. The institutional ethics committee approval was given vide letter number 2017-01.
A total of 84 diagnosed cases of pes anserine bursitis with knee OA fulfilling the criteria as mentioned below were included in the study. Sixteen of these patients had bilateral involvement, hence entailing the administration of 100 injections. This number of 100 injection limbs was selected based on a previous study where the sample size used was 47, and the participants were followed up for assessment till 4 weeks after injection.[13]
A detailed history was taken and patients were classified according to American College of Radiology (ACR) criteria[15] for OA. The diagnosis of pes anserine bursitis was made after a thorough clinical assessment of the patient. It included swelling seen over pes anserine area on inspection and severe palpatory tenderness in pes anserine area 1 inch below and anterior to medial tibial plateau.
Informed consent was taken from all the patients after explaining the study details in their own language.
Exclusion criteria
Cases of uncontrolled diabetes mellitus, skin infection at site of injection, pregnancy, knee effusion, hypersensitivity to methylprednisolone, any history of injection in the past 3 months, coagulopathy, surgical intervention or physical therapy in the past 3 months, other associated painful condition of lower extremities or knee.
Inclusion criteria
Knee OA as per ACR guidelines stages 1 to 3 (Kellgren Lawrence[16]).
Age at least 50 years.
Medial sided knee pain clinically correlating to pes anserine bursitis.
There were two outcome measures. First, the pain was indicated by the patient on a 10-point visual analog scale (VAS) where “1” indicated the minimum pain and “10” indicated the worst pain experienced by the patient. The second assessment was done using knee injury and osteoarthritis outcome score (KOOS).[17]
The KOOS’s five patient-relevant dimensions are scored separately:
Pain (9 items)
Symptoms (7 items)
ADL function (17 items)
Sport and recreation function (5 items)
Quality of life (4 items)
A Likert scale is used and all items have five possible answer options scored from 0 (no problems) to 4 (extreme problems) and each of the five scores is calculated as the sum of the items included. These scores are transformed to a 0–100 scale, with zero representing extreme knee problems and 100 representing no knee problems as common in orthopedic scales and generic measures.
Eighty-four patients were alternatively allocated into each of the two groups for two injection techniques. This random allocation technique ensured that there were 50 injection limbs in both the groups.
A single investigator administered the injection to all the patients, in both groups. All aseptic precautions were taken and the skin was prepared with a 5% betadine solution followed by spirit prior to the injection. 2-cc syringe with 22-gauge needle was put to use.
In group A, injection Methylprednisolone 80 mg was infiltrated at the point of maximal tenderness in the anserine bursa region by clinical assessment.
In group B, the patients were similarly injected with injection Methylprednisolone 80 mg in the pes anserine bursa but under ultrasound guidance [Figure 1]. Ultrasound machine used was Medison SONOACE X8 (made in Korea).
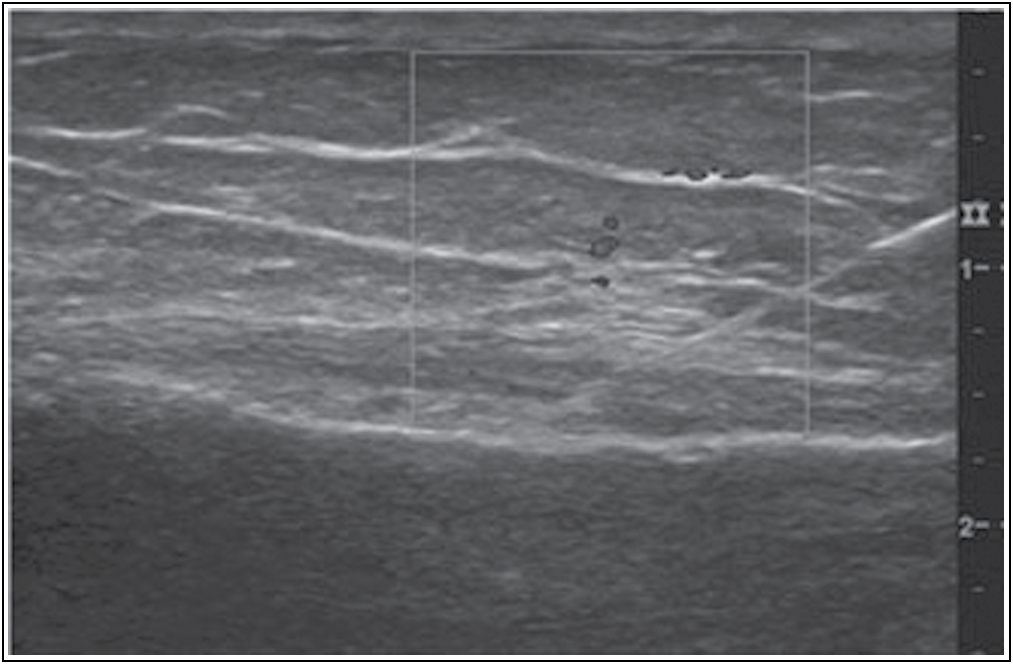
- Ultrasound image showing the needle in the inflamed pes anserine bursa
The patients were prescribed tab Diclofenac 50 mg to be taken if they experienced any pain after the injection. Outcome variables were measured at the baseline before the intervention and follow-up assessment was performed at 1 week, 1 month, and 3 months after the injection. The rehabilitation protocol takes around 6 to 8 weeks for getting a definitive improvement in function. Hence, 3 months was chosen as the last and final follow-up.
Injection procedure
Positioning
The patient was made to lie supine with the hip externally rotated with the knee in slight flexion.
Blind technique
Blind injection was given by clinically ascertaining the point of maximum tenderness in the location of pes anserine bursa, which is usually 1 inch anteroinferior to medial joint line.
Ultrasound-guided technique
The transducer was placed in two planes: oblique coronal and coronal planes. The semitendinosus tendon was identified and traced in distal posteromedial thigh till it converges with gracilis and sartorius tendon. All the tendons were traced till their attachments on tibia. The pes anserine bursa lies in plane deep to tendons. The inflamed bursa was identified. As per clinical correlation of findings, the corticosteroid injection was given in the plane relative to the position of transducer.
Statistical analysis
All the data were collected in a pretested proforma. The statistical analysis was performed by an external expert using the statistical program SPSS software program, version 25.0. The P value was set as 0.05 for all the evaluations across both groups. To analyze the effect of steroid injection in each group, paired t Student test was performed on the data collected at baseline and at 3 months after the injection. For the comparison of two techniques, unpaired Student t test was performed between two groups.
Results
No statistically significant differences were observed between the two groups in baseline characteristics [Table 1].
| Group A (injection given by blind technique) | Group B (injection given under ultrasound guidance) | |
|---|---|---|
| Gender | Females 30 (69.7 %) | Females 31 (75.6%) |
| (N,%) | Males 13 (30.2 %) | Males 10 (24.3%) |
| Total 43 | Total 41 | |
| Gender | Females 34 (68%) | Females 37 (74%) |
| (number of injections administered) | Males 16 (32%) | Males 13 (26%) |
| Total 50 | Total 50 | |
| Mean ± SD (age in years) | 54.2 ± 8.4 | 58.2 ± 8.2 |
| Side of affection | Right 20 (F 14, M 6) | Right 17 (F 13, M 4) |
| Left 16 (F 12, M 4) | Left 15 (F 12, M 3) | |
| Bilateral 7 (F 4, M 3) | Bilateral 9 (F 6, M 3) |
Table 2 shows the outcome measures, that is, VAS score and KOOS at baseline and at the end of study. In this study, mean improvement seen in patients was significant after both the techniques.
| Group A (injection given by blind technique) | Group B (injection given under ultrasound guidance) | Inter-group comparison | ||||||
|---|---|---|---|---|---|---|---|---|
| Before intervention | After 3 months of intervention | P Value | Before intervention | After 3 months of intervention | P Value | Before intervention (P Value) | After 3 months of intervention (P Value) | |
| VAS score | 6 (3-9) | 4 (1-7) | P < 0.05 | 7 (6–9) | 4 (2–7) | P < 0.0001 | P < 0.05 | p>0.05 |
| KOOS | 09 (4–16) | 80 (74–90) | P < 0.05 | 08(4–15) | 82(74–91) | P < 0.0001 | P < 0.05 | P < 0.05 |
At the final assessment at 3 months, there was no statistically significant difference seen in the outcome using the two different techniques, based on the VAS scores. This signifies that both the techniques were equally effective in producing improvement in VAS scores.
The KOOS data indicated that the ultrasound-guided injection technique was superior to the blind technique.
No patient in this study reported any major side effect after the injection procedure. There was slight pain reported at the injection site by five patients of study group A and eight patients in study group B. There were no withdrawals or dropouts in this study and all the registered patients kept a follow-up up to 3 months as had been advised.
Discussion
Studies have found that knee OA and pes anserine bursitis can coexist and clinical pes anserine tendino-bursitis (PATB) may be cause of knee pain. PATB is an easily treatable cause of knee pain. Its early detection and management are crucial and can significantly improve pain and function which can positively impact the patient’s quality of life.
This study was conducted to investigate whether a corticosteroid injection given in pes anserine bursa under ultrasound guidance was more effective as compared with an injection administered blindly.
It was found that irrespective of the technique of administration of corticosteroid injection, patients reported significant improvement in both VAS score and KOOS measured at 3 months compared with the baseline in each individual group.
When inter-group comparison was done, it was found that there was no statistically significant difference in improvement in VAS scores. However, the data collected on KOOS showed that the improvement in functional outcome was better when the injection was administered under ultrasound guidance as compared with the blind technique, at 3 months.
In a recent paper published by Mohamed Mortada et al.,[18] authors have studied the impact of ultrasonography detected pes anserine on pain and function in patients with primary knee OA. They concluded that presence of pes anserine bursitis on ultrasound is associated with increased pain and disability in knee OA.
Previously, Yoon et al.[7] conducted a study to assess the ultrasonographic findings in patients with knee OA with pes anserinus tendinitis or bursitis syndrome and to determine the correlation between the ultrasonography findings and the response to local corticosteroid injection. 26 patients with knee OA with clinically diagnosed PATBsyndrome were studied. They concluded that ultrasound can serve as a useful diagnostic tool for guiding treatment in PATB syndrome of patients with OA.
Finnoff et al.[19] conducted a study to compare the accuracy of ultrasound-guided versus unguided pes anserinus bursa injections in a 24 cadaveric model study. They concluded that unguided pes anserinus bursa injections rarely placed the injection within the pes anserinus bursa, whereas ultrasound-guided pes anserine bursa injections have a high degree of accuracy. Ultrasound guidance showed effectiveness in cadaveric studies, increasing accuracy from 17% (unguided) to 92%. However, the sample size was small in this study. And since it was conducted on cadavers, there is no question of functional outcome measurement or assessment of benefit perceived by the patient.
There are several other modalities in consideration for the management of pes anserine bursitis as well.
Saggini et al.[20] conducted a study to evaluate the effects of mesotherapy with diclofenac for anserine bursitis and found it to be effective in managing anserine bursitis in knee OA in the short term and mid-term.
Saeid Khosrawei et al.[21] conducted a study to investigate the effect of extracorporeal shock wave therapy (ESWT) on reducing chronic pain in patients with pes anserine bursitis. The results showed that ESWT could be effective in reducing the pain and treating PATB.
A study by Sarifakioglu et al.[22] indicated that physical therapy and corticosteroid injection are similarly effective in the treatment of PATB.
Mun et al.[23] published a case report claiming good relief with injection of polydeoxyribonucleotide injection on pes anserine bursitis.
The present study emphasizes the outcomes of steroid injection in pes anserine bursa comparing blind versus ultrasound-guided technique. Though ultrasound-guided injection is expected to administer steroid at the exact location and offer prompt and better pain relief that is long-standing avoiding the tendinous structure and preventing steroid-induced tendon degeneration, clinical efficacy measured with the help of one of the two outcome measures, that is, VAS score mentioned above does not yield any statistically significant difference. KOOS data however showed the superiority of injection under ultrasound guidance in improving the functional status of the patient as compared with the blind technique over a follow-up of 3 months.
This may be attributed to the fact that KOOS is a composite score comprising of pain, symptoms, ADLs, sports and recreation function and knee-related quality of life.
Limitations of the study
This study has its own limitations related with the study design, mainly due to the limited sample size. The relatively short follow-up is another limitation and would be important to consider in future designs. Furthermore, these results are only applicable to patients of similar characteristics to those of our sample, which may not be applicable to other population.
Conclusion
Our study suggests that ultrasound-guided steroid injection in pes anserine bursa is a more accurate and effective method of pain management than blind injection. Future studies involving larger sample size with longer follow-up may be needed to further compare the two techniques.
Financial support and sponsorship
Not applicable.
Conflicts of interest
There are no conflicts of interest.
References
- Acute pes anserine bursitis: Mr imaging. Radiology. 1995;194:525-7.
- [CrossRef] [PubMed] [Google Scholar]
- The MRI appearance of cystic lesions around the knee. Skeletal Radiol. 2004;33:187-209.
- [CrossRef] [PubMed] [Google Scholar]
- Anserina bursitis: A treatable cause of knee pain in patients with degenerative arthritis. Calif Med. 1973;119:8-10.
- [Google Scholar]
- Knee pain: Osteoarthritis or anserine bursitis? J Am Med Dir Assoc. 2003;4:164-6.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation between ultrasonographic findings and the response to corticosteroid injection in pes anserinus tendinobursitis syndrome in knee osteoarthritis patients. J Korean Med Sci. 2005;20:109-12.
- [CrossRef] [PubMed] [Google Scholar]
- Pes anserinus and anserine bursa: Anatomical study. Anat Cell Biol. 2014;47:127-31.
- [CrossRef] [PubMed] [Google Scholar]
- Pes anserine bursitis: An underdiagnosed cause of knee pain in overweight women. Am Fam Physician. 2016;93:170..
- [Google Scholar]
- Pay attention to the pes anserine in knee osteoarthritis. Curr Sports Med Rep. 2018;17:41..
- [CrossRef] [PubMed] [Google Scholar]
- Clinics in diagnostic imaging (77): Pes anserine bursitis. Singapore Med J. 2002;43:485-91.
- [Google Scholar]
- Accuracy and efficacy of ultrasound-guided pes anserinus bursa injection. J Clin Ultrasound. 2019;47:77-82.
- [CrossRef] [PubMed] [Google Scholar]
- USG-guided injection of corticosteroid for lateral epicondylitis does not improve clinical outcomes: A prospective randomised study. Arch Orthop Trauma Surg. 2017;137:601-6.
- [CrossRef] [PubMed] [Google Scholar]
- Development of criteria for the classification and reporting of osteoarthritis: Classification of osteoarthritis of the knee. Arthritis Rheum. 1986;29:1039-49.
- [CrossRef] [PubMed] [Google Scholar]
- Radiological Assessment of Osteoarthritis, Rheumatisme Research Center; 1957. :498-9.
- [Google Scholar]
- The knee injury and osteoarthritis outcome score (KOOS): From joint injury to osteoarthritis. Health Qual Life Outcomes. 2003;1:64..
- [CrossRef] [PubMed] [Google Scholar]
- Impact of ultrasonography-detected pes anserine bursitis on pain and function in patients with primary knee osteoarthritis. Indian J Rheumatol. 2020;15:73..
- [CrossRef] [Google Scholar]
- Accuracy of ultrasound-guided versus unguided pes anserinus bursa injections. Pm R. 2010;2:732-9.
- [CrossRef] [PubMed] [Google Scholar]
- Pes anserine bursitis in symptomatic osteoarthritis patients: A mesotherapy treatment study. J Altern Complement Med. 2015;21:480-4.
- [CrossRef] [PubMed] [Google Scholar]
- Investigating the effect of extracorporeal shock wave therapy on reducing chronic pain in patients with pes anserine bursitis: A randomized clinical-controlled trial. Adv Biomed Res. 2017;6:70..
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the efficacy of physical therapy and corticosteroid injection in the treatment of pes anserine tendino-bursitis. J Phys Ther Sci. 2016;28:1993-7.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of multiple intra-articular injections of polynucleotides on treatment of intractable knee osteoarthritis: A case report. Medicine (Baltimore). 2017;96:e9127..
- [CrossRef] [PubMed] [Google Scholar]




