
Translate this page into:
Ulnar nerve injury post Cubitus varus correction by lateral closing wedge osteotomy: Lessons learnt
Address for correspondence: Dr. Shubham Siddheshwar Zade, Department of Orthopaedics, Dr. Vasantrao Pawar Medical College, Hospital & Research Centre, Adgaon, Nashik 422003, Maharashtra, India. E-mail: shubhamz05123@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Challawar N, Zade SS, Chudasama VD. Ulnar nerve injury post Cubitus varus correction by lateral closing wedge osteotomy: Lessons learnt. J Orthop Spine 2022;10:19-23.
Abstract
BACKGROUND:
Supracondylar fractures of the humerus are the most common elbow injuries in skeletally immature children between 5 and 15 years of age. Managed conservatively or treated inadequately these fractures result in malunion-producing Cubitus varus deformity.
MATERIALS AND METHODS:
We retrospectively studied a 9-year-old male patient who presented to us with cubitus varus deformity owing to the conservative management of previous Supracondylar humerus fracture. Patient was operated by Lateral closing wedge osteotomy. Pre operative and post operative assessment was done clinically and with the help of radiographs.
RESULT:
Patient developed ulnar nerve palsy owing to the overcorrection of deformity which ultimately required ulnar nerve release and anterior transposition. Complete functional recovery was achieved 6 months post index surgery.
CONCLUSION:
Lateral closing wedge osteotomy provides an effective and relatively simple way for correcting cubitus varus deformity yet can result in ulnar nerve palsy in the event of overcorrection.
Keywords
Anterior ulnar nerve transposition
Cubitus varus
lateral closing wedge osteotomy
ulnar neuropraxia

Introduction
Elbow injuries are considerably common in skeletally immature children between 5 and 15 years of age.[1,2] Metaphyseal area of distal end humerus is the weakest area around the elbow joint and hence supracondylar fractures of humerus are the most common injuries around the elbow joint.[3]
Cubitus varus deformity is a three-dimensional deformity with varus, extension, and internal rotation of the distal humeral fragment.[4] Earlier Cubitus varus was considered a cosmetic deformity with no functional impairment.[5] Although the main presentation of the deformity is due to the unsightly appearance of the limb, Cubitus varus is now considered a factor for long-term functional impairment such as chronic pain, ulnar nerve palsy,[6,7] tardy posterolateral rotatory instability,[8] snapping elbow,[9] and an increased risk of lateral condyle prominence.[10,11] Moreover, the concept that the deformity can remodel with time has changed.[3]
The deformity can develop due to plethora of factors of which neglected or undertreated supracondylar fractures of the humerus are the most common ones rest being growth disturbances, and osteonecrosis of the medial humeral condyle with or without growth arrest.[12]
Treatment options include the following:
Observation with expectant remodeling––varus deformity not being in the plane of motion of elbow joint has very little potential for remodeling and hence this treatment modality is not recommended.
Corrective osteotomies––considered as a standard treatment.
Options include the following:
Medial open wedge osteotomy that causes lengthening of medial aspect of humerus causing stretching of ulnar nerve.[13]
Lateral closing wedge (LCW) osteotomy with or without simultaneous correction of rotation, also known as French osteotomy.[14]
Step cut osteotomy.
Arch osteotomy.[15]
Penta lateral osteotomy.[16]
Dome osteotomy.[17]
Materials and Methods
This was a retrospective study wherein a single male patient of 9 years and 0 months with right-hand dominance presented with left Cubitus varus deformity. It was first noticed by the parents of the patient with prior history of trauma which was managed nonoperatively by an above elbow cast 9 months ago [Figure 1].
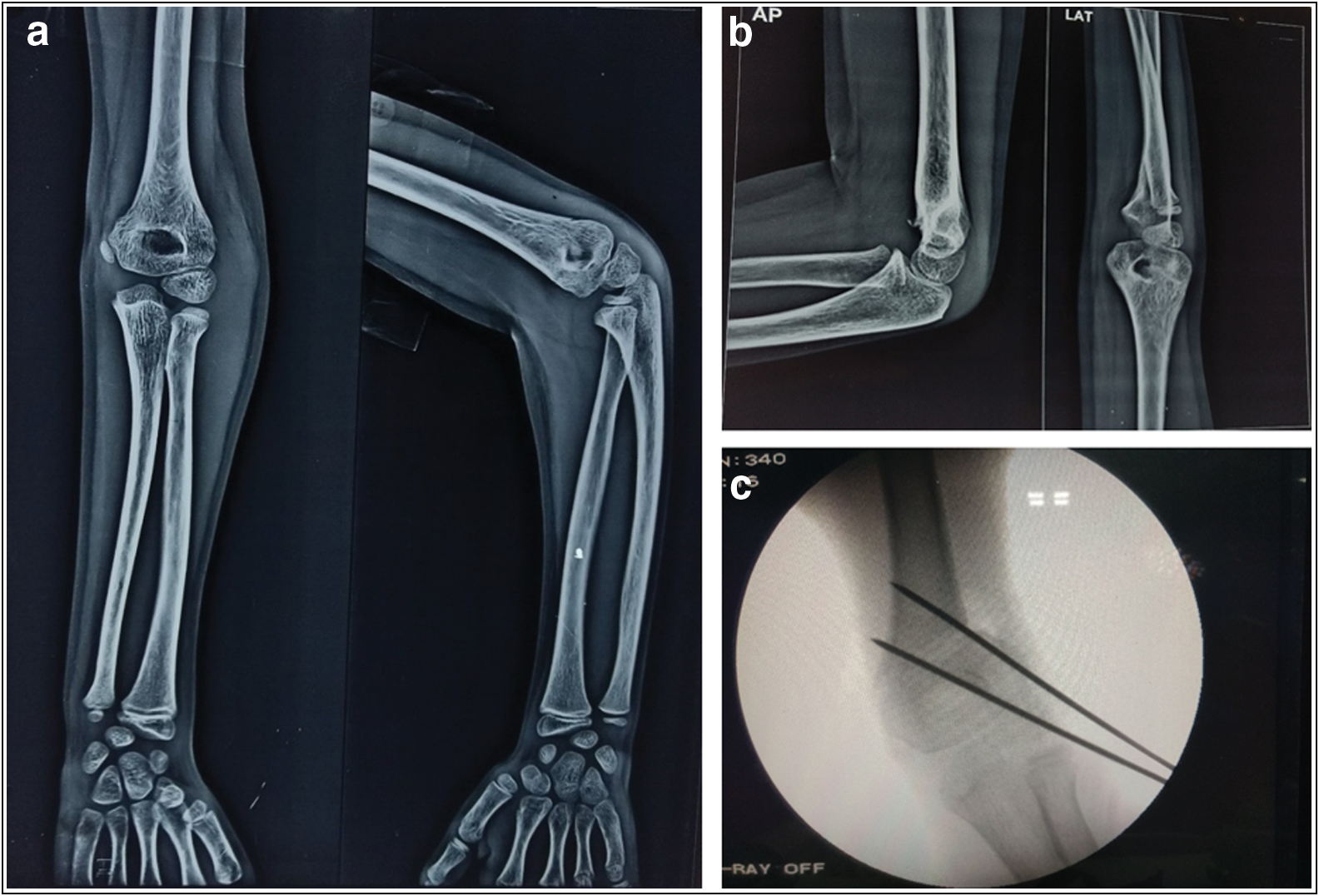
- (A) Index trauma radiograph suggestive of supracondylar fracture of humerus. (B) Radiograph showing mal united supracondylar fracture humerus 9 months post index trauma. (C) Intraoperative C-ARM image
Preoperative assessment of the patient included standard anteroposterior and lateral radiographs of affected elbow [Figure 1]. Neurology, range of movement [Figure 2], and carrying angle [Figure 3] were assessed clinically.
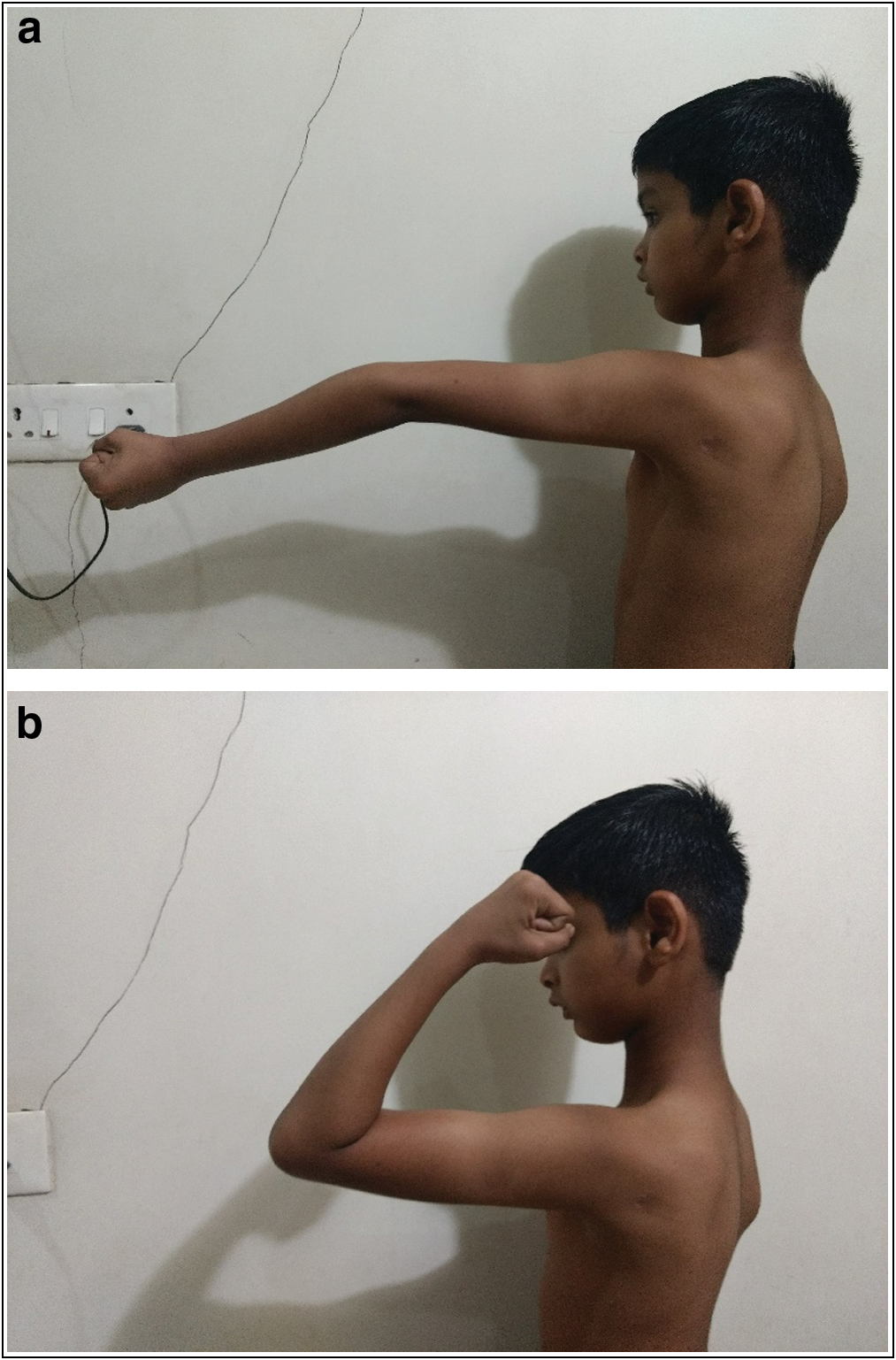
- (A and B) Hyperextension of elbow with limited flexion

- Preoperative carrying angle: right side 7.50° and left side –15.69°
The patient was operated on by LCW osteotomy because of its ease, simplicity, and proven functional outcomes. Size of the wedge was 1.5 cm and fixation was done with two lateral entry divergent k wires.
Results
The patient developed ulnar nerve palsy with sensory-motor involvement in the immediate postoperative period. Injury was not due to hardware as due precautions were taken. It was suspected that nerve injury is neuropraxia secondary to overstretching of nerve. The patient was advised electromyography-nerve conduction velocity (EMG-NCV) study at 3 weeks postoperatively; however, due to noncompliance it was performed 3 months post-surgery owing to persistent complaints.
EMG-NCV study at 3 months was suggestive of severe left ulnar sensorimotor axonal mononeuropathy. The patient was advised a second surgery for nerve exploration that was done 3 months post-surgery wherein ulnar nerve was released at the level of elbow joint behind medial humeral condyle and was transposed anteriorly [Figure 4]. Complete functional recovery was achieved 6 months post index surgery.
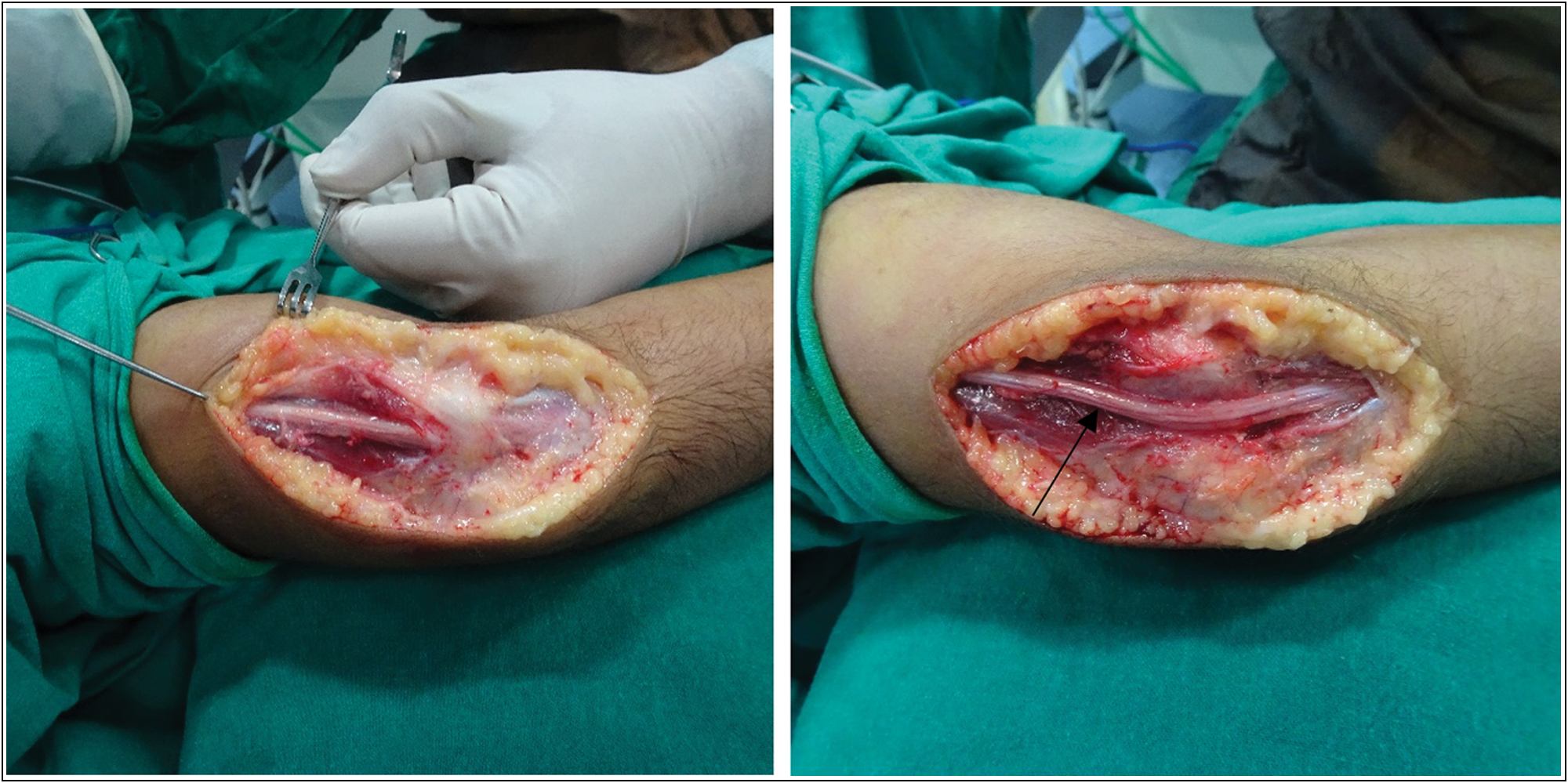
- Marked arrow showing atrophied ulnar nerve below medial condyle, which was subsequently transposed anteriorly
Osteotomy had united uneventfully at 6 weeks [Figure 5] and k wires were removed at 6 weeks post-surgery with initiation of range of motion exercises of elbow and wrist. The correction we achieved was of 37.82° (preoperative 15.69° varus [Figure 3]; postoperative 23.13° valgus [Figure 6).
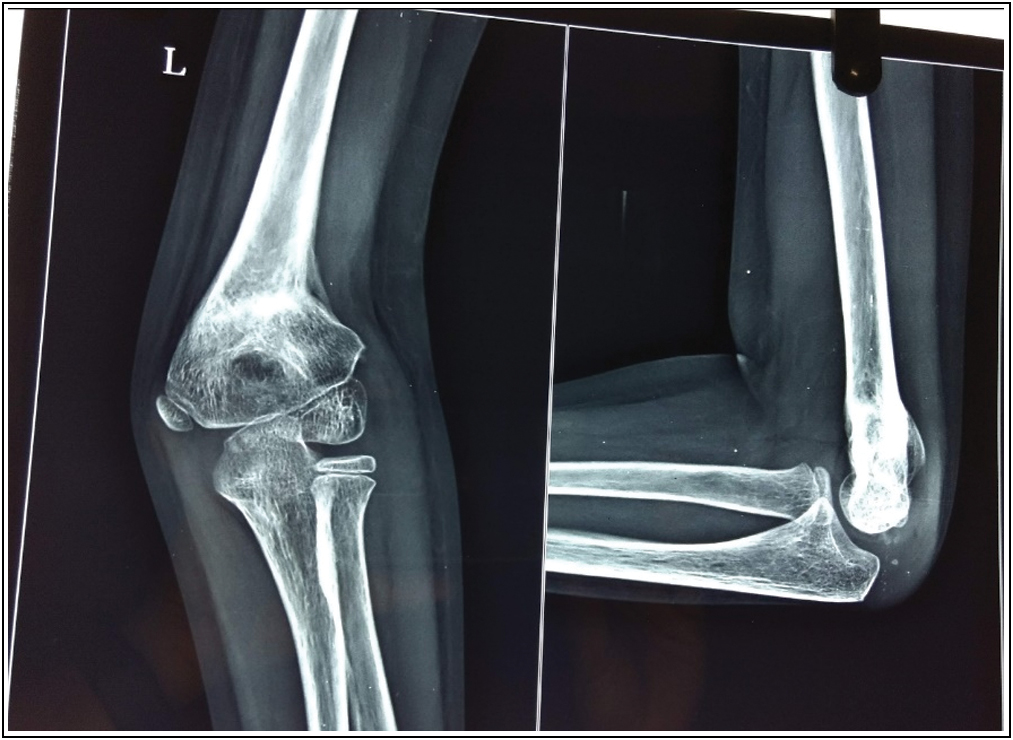
- Three-month postoperative radiograph showing completely united osteotomy

- Postoperative carrying angle: right side 7.50° and left side 22.13° (overcorrection)
| Preoperative | Postoperative | |
|---|---|---|
| Carrying angle | -15.69° | 23.13° |
| Range of motion | -15°-110° (patient had hyperextension) | 0°-130° |
Lateral condyle prominence was noted; however, we did not encounter pin tract infection, loss of fixation, stiffness, or unsightly scarring. Outcome of the procedure in this patient is considered as poor in the early postoperative period as per the following mentioned criteria put forth by Solfelt et al.[18]
| Excellent | Good | Poor |
|---|---|---|
| Described as excellent | Described as good, satisfactory, fair. | Described as poor or unsatisfactory |
| - No recurrence of symptoms | - Valgus | - Severe limitation in movement. |
| - Correction of the varus deformity to within 5° of the contralateral elbow. | correction or neutral but within 5° of the contralateral elbow. | - Significant pain. - Major perioperative complications. |
| - Movement to within 5° of the preoperative movement arc. | elbow. | Residual varus or neutral position but greater than 5° from contralateral elbow. |
| - No major perioperative complications. | Movement to within 10° of preoperative arc. | Loss of more than 10° of movement in any plane compared to contralateral elbow. |
Major complications were defined as residual varus deformity, nerve injury, infection, loss of fixation leading to reoperation, and growth arrest.
Minor complications included loss of fixation not leading to varus deformity or reoperation, unsightly scarring, stiffness, or a prominent lateral condyle. Pin tract Infection was considered as a major complication enough to downgrade a surgical outcome owing to the risk of deep or late infection.
Discussion
The conditions were not ideal when this study was performed owing to the patient noncompliance. Preoperative planning for wedge resection was done by measuring the carrying angle clinically of both affected and unaffected extremities.[19]
All variants of corrective osteotomy have an associated complication of nerve injury among which LCW osteotomy has minimal association.[20] Ulnar nerve injuries are commonly encountered with the posterior approach and seldomly with the lateral approach[21] owing to which nerve injury was suspected due to over correction.
Management of a neuropathy in immediate postoperative period aims at a trial of expectant management for 3 weeks provided one is confident of meticulous precautions taken to avoid nerve injury. If injury is suspected to be of iatrogenic origin, immediate exploration is warranted. At 3 weeks if no improvement is seen, an EMG-NCV should be performed based on which surgical decision can be taken at 3 weeks.
Conclusion
Lessons learned from this study are as follows:
LCW is a proven established method of Cubitus varus correction. Nerve injury is very rarely reported with this approach. Ulnar nerve palsy can occur in this approach with overcorrection. Hence the wedge taken should not be overestimated.
In case of larger wedge resection, it would be prudent to do a prophylactic anterior transposition of ulnar nerve.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Not applicable.
Conflicts of interest
There are no conflicts of interest.
References
- Supracondylar fracture of the humerus in children: A late review of end-results with special reference to the cause of deformity disability and complications. Acta Chir Scand Suppl. 1966;369:1-72.
- [Google Scholar]
- Fracture and dislocations in the region of the elbow. Surg Gynecol Obstet. 1933;56:335-59.
- [Google Scholar]
- Management of Cubitus varus deformity in children by closed dome osteotomy. J Clin Diagn Res. 2017;11:RC08-12.
- [CrossRef] [PubMed] [Google Scholar]
- Translation step-cut osteotomy for the treatment of posttraumatic Cubitus varus. J Pediatr Orthop. 2011;31:353-65.
- [CrossRef] [PubMed] [Google Scholar]
- Translation step-cut osteotomy for the treatment of posttraumatic Cubitus varus. J Pediatr Orthop. 2011;31:353-65.
- [CrossRef] [PubMed] [Google Scholar]
- Posterolateral rotatory instability of the elbow after posttraumatic Cubitus varus. J Shoulder Elbow Surg. 1997;6:405-9.
- [CrossRef] [PubMed] [Google Scholar]
- Internal rotation deformity and tardy ulnar nerve palsy after supracondylar humeral fracture. J Shoulder Elbow Surg. 1995;4:23-9.
- [CrossRef] [PubMed] [Google Scholar]
- Tardy posterolateral rotatory instability of the elbow due to Cubitus varus. J Bone Joint Surg Am. 2001;83:1358-69.
- [CrossRef] [PubMed] [Google Scholar]
- Snapping of the medial head of the triceps and recurrent dislocation of the ulnar nerve: Anatomical and dynamic factors. J Bone Joint Surg Am. 1998;80:239-47.
- [CrossRef] [PubMed] [Google Scholar]
- Lateral condylar fracture of the humerus following posttraumatic Cubitus varus. J Pediatr Orthop. 1994;14:466-70.
- [CrossRef] [PubMed] [Google Scholar]
- Second fracture of the distal humerus after varus malunion of a supracondylar fracture in children. J Bone Joint Surg Br. 1998;80:791-7.
- [CrossRef] [PubMed] [Google Scholar]
- Recurrent supracondylar humerus fracture following prior malunion. Iowa Orthop J. 2001;21:8-12.
- [Google Scholar]
- Lateral closing wedge supracondylar osteotomy of humerus for post-traumatic Cubitus varus in children. Injury. 1997;28:643-7.
- [CrossRef] [PubMed] [Google Scholar]
- Arc osteotomy of the humerus to correct Cubitus varus. Clinical Orthopaedics and Related Research®. 1997;336:111-5.
- [CrossRef] [PubMed] [Google Scholar]
- Pentalateral osteotomy for Cubitus varus: Clinical experiences of a new technique. J Bone Joint Surg Br. 1989;71:667-70.
- [CrossRef] [PubMed] [Google Scholar]
- Osteotomy of distal humerus for correction of Cubitus varus, Tachdjian’s Paediatric Orthopaedics. . 1972;1:1290.
- [Google Scholar]
- Supracondylar osteotomy for the treatment of Cubitus varus in children: A systematic review. Bone Joint J. 2014;96B:691-700.
- [CrossRef] [PubMed] [Google Scholar]
- Evolution of the carrying angle of the elbow: A clinical and radiographic study. Acta Ortopedica Brasileira. 2011;19:79-82.
- [CrossRef] [Google Scholar]
- Supracondylar osteotomy for the treatment of Cubitus varus in children: A systematic review. Bone Joint J 2014:96-B.:691-B.
- [CrossRef] [PubMed] [Google Scholar]
- Complications of supracondylar osteotomies for Cubitus varus. J Pediatr Orthop. 2012;32:232-40.
- [CrossRef] [PubMed] [Google Scholar]




