
Translate this page into:
Functional outcome of proximal tibia fractures (Shatzker’s type V and VI) fixed with open reduction and internal fixation with dual plate osteosynthesis
Address for correspondence: Dr. Vishal Singh, Department of Neurosurgery, Sher-i-Kashmir Institute of Medical Sciences (SKIMS), Room No. G17, Old SR Hostel, Soura, Srinagar 190011, Jammu and Kashmir, India. E-mail: dr.vishalsingh1689@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Singh Charan J, Singh V, Gundavarapu A, Shashi Kumar HK. Functional outcome of proximal tibia fractures (Shatzker's type V and VI) fixed with open reduction and internal fixation with dual plate osteosynthesis. J Orthop Spine 2022;10:6-12.
Abstract
INTRODUCTION:
Tibial plateau fractures occur when the proximal tibia bears an excessive axial load and commonly occur in road Traffic accidents and sports injuries. It constitutes 1% of all orthopedic fractures and 8% of fractures in the elderly. The treatment of tibial plateau fractures is continuously evolving. Various techniques have emerged over the last few decades. Many people have studied these fractures and their management modalities and no single consensus has been reached regarding the superiority of any modality.
MATERIALS AND METHODS:
Following institutional scientific and ethical committee approval, this study was undertaken in the patients with proximal tibia fractures (Shatzker’s type V and VI) reporting to the Department of Orthopedics at Apollo Hospital Bannerghatta Road, Bengaluru during the study period. This was a prospective observational study. A total of 30 consecutive patients were followed up as per the inclusion criteria. They were followed up for 6 months.
RESULTS:
There were a total of 30 cases of proximal tibia Shatzker type V and VI fractures followed up during the study period. The demographics constituted 73.33% males and 26.67% females with an age range of 23–64 years and a mean age of 41.66 years. The most common mode of injury was road traffic accidents amounting to 73.33% of fractures. The majority of patients were in the age group less than 40 years and men were involved more than women. The functional outcome measured via the Modified Rasmussen Score showed good to excellent results in 93.33% of cases in the postop period at 6 months.
CONCLUSION:
This study shows fixation with dual anatomical locking plate and screws for proximal tibia Shatzker type V and VI fractures gives good to excellent functional outcomes in the early postop period.
Keywords
Anatomical locking plate
articulate reduction
functional outcome
proximal tibia fractures

Introduction
Tibial plateau fractures occur when the proximal tibia bears an excessive axial load and commonly occur in road traffic accidents and sports injuries. It constitutes 1% of all orthopedic fractures and 8% of fractures in the elderly.[1] These fractures are intra-articular; therefore, their fixation is an important issue.[2] These fractures classically were described as bumper or fenders fractures. They gravely affect the biomechanics, stability, and range of motion of the knee joint.[3,4]
The pattern of the fracture correlates to the magnitude of the force imparted on that lower limb. The higher energy fractures (Schatzker 4–6),[5] or those in pathological bone, are associated with severe articular disruption through axial loading of the tibial plateau in combination with a varus or valgus force loading.[6] This results in articular surface depression, condyle separations, metaphyseal comminution, and diaphyseal extension.[7]
There is still controversy in selecting the type of surgical treatment. The goal of these types of fractures is to restore congruency, stability, alignment, and to attain full range of movement.[8] The blood supply of the tibia is precarious. Therefore, high-energy fractures are associated with compartment syndrome and neural or vascular injuries.[9]
Many people have studied these fractures and their management modalities and no single consensus has been reached regarding the superiority of any modality. The proposed study was a prospective, observational study of 30 cases of fracture of the proximal condyle of the tibia (Schatzker 5 and 6) fixed with dual plating.
Aims and objectives
Assessment of functional outcome of proximal tibial condyle fractures (Schatzker type V and VI) fixed with dual plating.
Functional outcome will be measured by the Modified Rasmussen criteria for clinical assessment score.
Materials and Methods
This prospective case series was carried out from April 2018 to June 2019 at the tertiary center Apollo Hospital Bannerghatta Road, Bangaluru (Karnataka) in the age group of 18–70 years. A total of 30 patients with proximal tibia fracture fitting the inclusion criteria planned for surgical fixation with dual plating were studied.
Study design
This was a prospective observational study.
Consent and Ethical clearance
Detailed written informed consent was taken from all the patients of interest after clearance from the ethical committee
(IECC no: ECR/320/inst/KA/2013/RR-16).
Sample size
Thirty patients were selected based on prevalence and average numbers of cases of interest in our institute annually.
Sampling technique
Purposive sampling method
Inclusion criteria
Isolated closed fractures of the tibial plateau (Schatzker type 5 and 6).
Schatzker type 5 and 6 tibial plateau fractures.
Age 18–70 years.
Exclusion criteria
Compound/open fracture.
Mid-shaft TIBIAL fracture.
Schatzker type 1, 2, 3, and 4.
Unmotivated patients.
Preoperative management
All patients fulfilling the above criteria and willingly motivated were enrolled to participate. All the information related to the management of patients was recorded in a designated case sheet. A detailed history was taken with particular emphasis on the mode of injury and associated comorbidities. Detailed clinical assessment was done in each case.
The affected lower limb was immobilized in above knee POP slab or knee immobilizer with window to evaluate skin condition and for ice pack application. Oral or parental NSAIDs were given to relieve the pain. Routine investigations such as CBC, blood grouping, blood sugar, LFT, KFT, urine routine, chest X-ray, ECG, and ECHO were done. Serology tests were done before surgery on all patients.
Detailed radiological investigations were offered (A) X-ray of knee joint with tibia––AP and lateral views were taken to assess the site of the fracture, the fracture type (displacement and comminution), and were classified according to Shatzker classification (5). (B) CT 3D knee with proximal tibia and other specific investigations whichever were needed like MRI knee or arteriogram were done [Figure 1].
All patients were operated as early as possible once their general condition was good and stable and the patients were fit for surgery as assessed by preanesthetic checkup (PAC) protocol.
Preoperative preparation of patients: Patients were kept fasting for 6 h before surgery. Written informed consent for surgery was taken. Single-dose intravenous inj. Cefuroxime 1.5 g was administered 30 min before surgery to all patients. In every case, spinal anesthesia was given with epidural anesthesia (SA+EA). Parts were prepared from groin to ankle.

- Preoperative radiographs (X-rays and CT)
Surgical procedure
(Open reduction and internal fixation with dual platting)
Position. Supine position on the radiolucent OT table with a bolster under the ipsilateral pelvic region for the anterolateral approach and was removed later while starting the posteromedial approach and contralateral limb was positioned on lithotomy post for better-undisturbed C arm movements and imaging. Tourniquet was used for all the surgeries.
Approach. Standard midline, anterolateral, anteromedial, and posteromedial approaches depending on fracture pattern were used. Submeniscal arthrotomy was done for visualization of articular reduction. An autogenous cancellous bone graft was taken from the ipsilateral iliac crest for severe communication and metaphyseal void.
Instrumenttion. Pre-contoured anatomical plates (T and L buttress plates and locking proximal tibial plates both lateral and medial from 4 holes to 10 holed), appropriate size screws (3.5 mm cortical screws, cancellous locking screws, cortical locking screws, and 6.5 mm cannulated cancellous screws) and kirschner wires were used.
After fixation, the tourniquet was released and hemostasis was achieved. The surgical incisions were closed over a suction drain and compression dressing was applied.
Postoperative management
Crepe bandage was applied on the operated leg and the knee was immobilized in a long knee brace with limb elevation over pillow. IV antibiotic Cefuroxime 750 mg and IV Amikacin 500 mg, both 12 hourly for the first 3 days were given. IV Paracetamol and IV Tramadol were given for pain management. Check X-ray was on postoperative day 0. Wound inspection and dressing were done on second, and eighth postoperative day.
Patients were taught non-weightbearing ambulation with a walker and advised not to put weight on the operated leg for at least 6 weeks. Also taught static quadriceps stretching, active ankle and toe pump movements, and active and passive straight leg rising. Patients were immediately put on CPM (passive knee flexion machine) to achieve passive knee flexion of at least 90° (0°–45° on POD 1° and 10° increase on subsequent days). Patients were discharged on oral analgesics for 10 days and SOS thereafter with DVT prophylaxis for 6 weeks.
Follow up
The patients were evaluated postoperatively and during follow-up (up to 6 months) based on functional outcome scores (Modified Rasmussen criteria for clinical assessment[10]) and X-ray knee joint was done on each follow-up to look for radiological union [Figures 2 and 3].
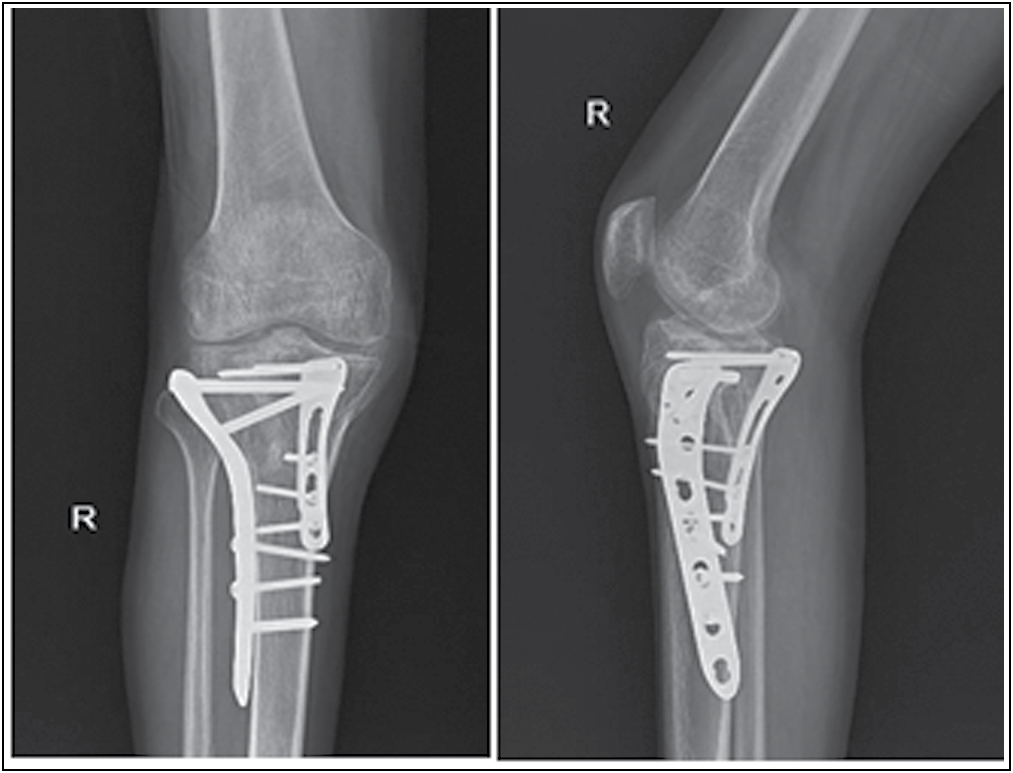
- Postoperative radiographs at 6 month

- Flexion and extension at 6 month
First follow up at 3 weeks, second follow up at 3 months, and third follow up at 6 months were done.
Statistical methods:
Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements were presented on mean ± SD (Min–Max) and results on categorical measurements were presented in Number (%). Significance is assessed at 5% level of significance. Dependent variables were normally distributed, Samples drawn from the population were random, and Cases of the samples were independent. Chi-square/ Fisher Exact test was used for the significance of study parameters on a categorical scale between groups in, Non-parametric setting for Qualitative data analysis. Fisher exact test was used when cell samples were very small.
Results
The following results were observed in 30 consecutive patients fitting in inclusive criteria, treated for proximal tibia (Schatzker‘s V and VI) fracture with dual plating. Tables 1 and 2 show the age, gender, mode of injury (MOI), the side affected, and type of fracture distribution among the study population along with flexion ROM [Table 1] and Modified Rasmussen score [Table 2] at 6 months. Tables 3 and 4 show injury to surgery time taken and use of bone graft, respectively. Extension lag and post-operative complications are depicted in Tables 5 and 6, respectively.
| Variables | Flexion range movement 6 months | Total (n=30) | P value | |||
|---|---|---|---|---|---|---|
| Excellent (n=18) | Good (n=8) | Fair (n=3) | Poor (n=1) | |||
| Age in years | ||||||
| 21-30 | 3(16.7%) | 1(12.5%) | 0(0%) | 0(0%) | 4(13.3%) | <0.001** |
| 31-40 | 11(61.1%) | 0(0%) | 0(0%) | 0(0%) | 11(36.7%) | |
| 41-50 | 4(22.2%) | 3(37.5%) | 0(0%) | 0(0%) | 7(23.3%) | |
| 51-60 | 0(0%) | 4(50%) | 2(66.7%) | 0(0%) | 6(20%) | |
| >60 | 0(0%) | 0(0%) | 1(33.3%) | 1(100%) | 2(6.7%) | |
| Gender | ||||||
| Female | 4(22.2%) | 4(50%) | 0(0%) | 0(0%) | 8(26.7%) | 0.370 |
| Male | 14(778%) | 4(50%) | 3(100%) | 1(100%) | 22(73.3%) | |
| MOI | ||||||
| FALL | 2(11.1%) | 4(50%) | 2(66.7%) | 0(0%) | 8(26.7%) | 0.048* |
| RTA | 16(88.9%) | 4(50%) | 1(33.3%) | 1(100%) | 22(73.3%) | |
| Side affected | ||||||
| B/L | 0(0%) | 1(12.5%) | 0(0%) | 0(0%) | 1(3.3%) | 0.616 |
| Left | 8(44.4%) | 2(25%) | 1(33.3%) | 0(0%) | 11(36.7%) | |
| Right | 10(55.6%) | 5(62.5%) | 2(66.7%) | 1(100%) | 18(60%) | |
| Type of Fracture | ||||||
| V(both knee) | 0(0%) | 1(12.5%) | 0(0%) | 0(0%) | 1(3.3%) | 0.160 |
| V | 14(778%) | 5(62.5%) | 1(33.3%) | 0(0%) | 20(66.7%) | |
| VI | 4(22.2%) | 2(25%) | 2(66.7%) | 1(100%) | 9(30%) | |
| variables | Modified Rasmussen score 6 months | Total (n=30) | P value | |||
|---|---|---|---|---|---|---|
| Excellent (n=25) | Good (n=3) | Fair (n=1) | Poor (n=1) | |||
| Age in years | ||||||
| 21-30 | 4(16%) | 0(0%) | 0(0%) | 0(0%) | 4(13.3%) | <0.001** |
| 31-40 | 11(44%) | 0(0%) | 0(0%) | 0(0%) | 11(36.7%) | |
| 41-50 | 7(28%) | 0(0%) | 0(0%) | 0(0%) | 7(23.3%) | |
| 51-60 | 3(12%) | 3(100%) | 0(0%) | 0(0%) | 6(20%) | |
| >60 | 0(0%) | 0(0%) | 1(100%) | 1(100%) | 2(6.7%) | |
| Gender | ||||||
| Female | 8(32%) | 0(0%) | 0(0%) | 0(0%) | 8(26.7%) | 0.754 |
| Male | 17(68%) | 3(100%) | 1(100%) | 1(100%) | 22(73.3%) | |
| MOI | ||||||
| FALL | 6(24%) | 1(33.3%) | 1(100%) | 0(0%) | 8(26.7%) | 0.651 |
| RTA | 19(76%) | 2(66.7%) | 0(0%) | 1(100%) | 22(73.3%) | |
| Side affected | ||||||
| B/L | 1(4%) | 0(0%) | 0(0%) | 0(0%) | 1(3.3%) | 0.355 |
| Left | 10(40%) | 0(0%) | 1(100%) | 0(0%) | 11(36.7%) | |
| Right | 14(56%) | 3(100%) | 0(0%) | 1(100%) | 18(60%) | |
| Type of Fracture | ||||||
| V (Both knee) | 1(4%) | 0(0%) | 0(0%) | 0(0%) | 1(3.3%) | 0.021* |
| V | 19(76%) | 0(0%) | 1(100%) | 0(0%) | 20(66.7%) | |
| VI | 5(20%) | 3(100%) | 0(0%) | 1(100%) | 9(30%) | |
| Injury Surgery Time | No. of patients | % |
|---|---|---|
| 1 Day | 5 | 16.7 |
| 2 Days | 10 | 33.3 |
| 3 Days | 10 | 33.3 |
| 4 Days | 3 | 10.0 |
| 5 Days | 2 | 6.7 |
| Total | 30 | 100.0 |
| Bone Grafting | No. of patients | % |
|---|---|---|
| No | 26 | 86.7 |
| Yes | 4 | 13.3 |
| Total | 30 | 100.0 |
| Extension lag 6months | No. of patients | % |
|---|---|---|
| <5degree | 4 | 13.33 |
| 6-10degree | 1 | 3.33 |
| No | 25 | 83.33 |
| Total | 30 | 100.0 |
| Complications | No. of patients (n=30) | % |
|---|---|---|
| No | 29 | 96.7 |
| Yes | 1 | 3.3 |
| Knee Stiffness | 1 | 3.3 |
| Knee Infection | 1 | 3.3 |
Discussion
Dual osteosynthesis has become a universally accepted method of internal fixation for complex bi-condylar tibial plateau fractures. The present study was planned to assess the functional outcome of single and dual plating in bi-condylar tibia fractures.
In this study of 30 patients, mean age of the patients was 41.66 years with range of 23–64 years. There were 22 males (73.3%) and 8 females (26.7%) showed there was a higher incidence in younger people and males. The higher incidence in males and Youngers indicated that they had more outdoor activities and also were more exposed to road traffic accidents. The majority of females, being housewives, were less exposed to high-energy trauma. Prasad et al.[11] had conducted a study on the functional outcome of Schatzker V and VI fractures treated with dual plating. 40 patients were treated and followed up. The mean age of their study was found to be 40 years. There was a high incidence of males (33) than females (7). Yong Zhang et al.[12] reported the outcome of dual plating in 79 patients. The mean age was found to be 37 years and there was a higher incidence in males (74) when compared to females (5). Thus, our study on age and sex incidence matched with other series.
In this study, most of the injuries were caused by road traffic accidents. We had 22(73.3.%) patients with RTA injuries and 8(26.7%) patients with fall. Prasad GT et al,[13] in their series had almost all cases with road traffic accidents. Devdatta Neogi et al,[14] in their series of 32 patients treated with dual plating, had a maximum number of patients with RTA injuries (24) as compared to fall (8).
In our study of 30 patients, 20 patients (66.67%) belonged to type V of the Schatzker classification,1 patient with B/L Type V (3.33%), whereas 9 patients (30%) belonged to type VI. There was no statistically significant difference (P = 0.061) in the number of patients between type V and VI fractures. In 2014 Dumbre Patil et al[15] presented a series of 21 patients with posteromedial tibia condyle fragments (19 males, 2 females), there were 6 type IV, 10 type V and 5 type VI Schatzker fractures. Prasad GT et al,[13] in their study of 40 patients, had equal number of patients with type V and VI fractures (20 type V, 20 type VI). Thus, our study on type of fractures as per Schatzker classification matched with other series.
In the present study, the majority of the patients (up to 93.3%) were operated on within 4 days of injury. Mean duration between injury and surgery was 2.6 days. All patients were operated on between 1 and 5 days. Long duration between injury and surgery was attributed to late presentation to our institution after the injury, severity of injury, edema, associated injuries, and further evaluation of fracture using higher modalities of investigations like 3D CT SCAN. Thus, our study on time interval between injury and surgery matched with other studies.
In this study, 4 out of 30 cases (13.3%) had undergone additional bone grafting. Bone grafting was done due to severe postero-medial communition and metaphyseal bone defect. We observed that satisfactory reduction and bone grafting is required in patients with extensive communition and metaphysio-diaphyseal dissociation. Yong Zhang et al.,[12] in their study of a total of 79 patients, 51 patients have undergone primary bone grafting.
Devadatta neogi et al.[14] reported that 44 out of 61 cases had undergone bone grafting.
In this study, the majority of the patients achieved a good range of knee flexion (above 1100) which accounted for 80%. Range of movement varied from 750 to 1350. Mean range of movement was 113.670. Prasad GT et al,[13] in their study of 40 patients, reported mean range of flexion of about 1280 ranging from 1200–1350. Devadatta neogi et al.,[14] reported a mean range of flexion of about 1240 ranging from 500- 1350 in 32 cases. Yong Zhang et al.,[12] in their study had reported a mean range of flexion of 1210. Range of movement was found to be less in type VI patients due to severe communition and soft tissue damage. Rigorous physiotherapy plays an important role in the functional outcome of type V and VI fractures.
We had 1 case of superficial infection out of 30 cases in this study. We had 3.3% infection rate in this series. The infection subsided completely after thorough debridement and IV antibiotic therapy according to culture and sensitivity. Low infection rate in our series may be attributed to gentle soft tissue handling, and perioperative antibiotic cover. We used third-generation cephalosporin (ceftriaxone + sulbactam 1.5gm) half hour prior to surgery and 3 days postoperatively. An Aminoglycoside antibiotic (Amikacin 500 mg) was also given for 3 postoperative days. Yong Zhang et al.,[12]in their study of 79 cases, reported a total of 9 infected cases with 6 being superficial and three being deep. Devadatta neogi et al.[14] reported four cases of superficial infections out of 32 cases.
In the present study, we had 1 case of knee stiffness out of 30 cases. Rate of knee stiffness that occurred in our study was 3.33%. Knee stiffness has been defined by Kim et al. 94, as a flexion contracture >15° and a maximum flexion <75°. In our study, 1 patient had a knee flexion of 75 degrees due to lack of proper physiotherapy even after training. He also had associated co-morbidity which made us to immobilize him for prolonged period.
In our study, no patient had post-operative degenerative joint diseases on follow up. 83.3% (25) patients in our study had no extensor lag, 13.3% (4) patients had 1–5 degree lag and 3.33% (1) had 6–10 degree lag postoperative measured on the 6th month. This parameter is related to postoperative physiotherapy session and at home exercise.
Time to union is the time taken for the fracture to unite completely, indicated clinically by no tenderness on palpation, painless full weight-bearing walking, and radiologically by good consolidation of fracture site. In the present study, there were significantly more patients whose union rate was 2.5-6months. Teriparatide 8IU daily used in 4 patients postoperatively for 3 months showed union at 2.5 month. Prasad GT et al,[13] in their study of 40 patients, reported an average time to union as 14 weeks (3.5 months) ranging from 8–22 weeks. Devadatta Neogi et al,[14] reported an average time to union of about 5 months. We observed that type VI fractures had taken longer time to unite than type V fractures.
Conclusion
We conclude that dual plating for proximal tibia bi-condylar fracture (Schatzker’s V and VI) fractures has improved functional outcomes in postop period with low complication rate.
Skin and soft-tissue conditions should be assessed pre-operatively and it is important to understand that one should wait for edema to settle down and wrinkle signs to appear before operating these fractures. Adequate imaging studies including proper X-ray views and 3D CT scan are a must for the planning of surgical fixation. Availability of good quality AO-type implants and sophisticated operation theatre equipped with C-arm and quality instruments as well as expert surgeons and assistants are of paramount importance. Surgical approaches and skills need to be developed and mastered for achieving the best results. In case of depressed fractures, a cortical window should be made and articular cartilage should be elevated with help of various small curved punches and cortico- cancellous bone grafting should be done to fill up the void whenever necessary. Particular attention should be paid to the articular reduction, plate position, length of locking screws, and stability of the whole construct. Early aggressive knee range of movements has to be started as soon as the fracture is fixed. Full weight-bearing mobilization should be allowed only after the radiological union.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Not applicable.
Conflicts of interest
There are no conflicts of interest.
References
- Guidelines in Fracture Management Proximal Tibia. (1st). Noida: Thieme Medical and Scientific Publishers Private Limited; 2014. p. :61. Chapter 3.
- [CrossRef] [Google Scholar]
- The treatment of fracture of the external tibial condyle:(Bumperfracture) J Ame Med Assoc. 1940;115:1683-7.
- [CrossRef] [Google Scholar]
- Clin Orthop Related Res. 1979;138:94..
- The Chertsey classification of tibial plateau fractures–How reliable is it? Orthop Proc. 2006;88:173-4.
- [Google Scholar]
- Treatment of high-energy tibial plateau fractures. Strategies Trauma Limb Reconst. 2006;1:18-28.
- [CrossRef] [Google Scholar]
- Fractures of the tibial plateau: A review of ninety-five patients and comparison of treatment methods. J Trauma. 1981;21:376-81.
- [CrossRef] [PubMed] [Google Scholar]
- Fractures of the lateral condyle of the tibia. J Bone Joint Surg Br 1956:38-B.:612-B.
- [CrossRef] [PubMed] [Google Scholar]
- Tibial condylar fractures Impairment of knee joint stability as an indication of surgical treatment. J Bone Joint Surg Am. 1973;55:1331-50.
- [CrossRef] [Google Scholar]
- Three-column fixation for complex tibial plateau fractures. J Orthop Trauma. 2010;24:683-92.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of complicated tibial plateau fractures with dual plating via a 2-incision technique. Orthopedics. 2012;35:e359-64.
- [CrossRef] [Google Scholar]
- VI tibial plateau fractures treated with dual plates. Indian J Orthop. 2013;47:188-94.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative study of single lateral locked plating versus double plating in type C bicondylar tibial plateau fractures. Indian J Orthop. 2015;49:193-8.
- [CrossRef] [PubMed] [Google Scholar]
- Posteromedial tibial plateau fractures: Fixation with antiglide plate using posteromedial supine approach, Retrospective series of 21 patients. J Maharashtra Orthop Assoc. 2014;9:6-11.
- [Google Scholar]




