
Translate this page into:
Comparison of surgical and nonsurgical treatment of lumbar disc herniation with motor deficit: A prospective study
Address for correspondence: Dr. Saurav Narayan Nanda, Department of Orthopaedics, Kalinga Institute of Medical Sciences, Bhubaneswar - 751 024, Odisha, India. E-mail: saurav.scb@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Arfaaz SK, Mohanty SN, Panda AP, Nanda SN, Kumar A, Biswas S. Comparison of surgical and nonsurgical treatment of lumbar disc herniation with motor deficit: A prospective study. J Orthop Spine 2021;9:31-8.
Abstract
INTRODUCTION:
Several studies had compared the differences between surgical and nonsurgical modalities of treatment for patients with herniated discs. Some studies announced several modalities for treating motor weakness caused by lumbar disc herniation but few randomized control trials had compared the efficacy of one treatment over the other treatment except cross-over treatment. This study excludes patients underwent cross over treatment. This study aims to assess outcomes of patients of lumbar disc herniation with motor deficit who underwent surgical treatment with a patient group who underwent nonsurgical treatment.
Subjects and Methods:
We included 75 cases of lumbar disc herniation with the motor deficit in our tertiary healthcare center. Thirty-six patients were treated with a microdiscectomy, and 39 patients were treated conservatively prospectively from June 2018 to June 2019. The minimum follow-up period was 1 year, i.e., at 1, 3, 6, and 12 months, respectively. Visual analog scale compares outcomes for pain evaluation, motor function by Medical Research Council scale and Oswestry Low Back Pain Questionnaire for overall health quality of life.
RESULTS:
Patients who undertook surgical treatment shown rapid recovery of the motor deficit, as well as rapid alleviation of symptoms in the first 6 months, postoperatively compared to the nonsurgical group. The difference was statistically significant between both groups in the initial period but the difference, was no longer significant during the final follow-up examination at 1 year.
CONCLUSION:
Early surgical treatment of properly selected patients of severe motor weakness and severe pain from disc herniation could provide a chance for rapid alleviation.
Keywords
Conservative treatment
lumbar disc herniation
microdiscectomy
motor deficit
nonsurgical treatment

Introduction
Humans have been plagued by low back pain since the beginning of recorded history. Up to 80% of people have experienced this symptom at some time in their lives. Impairments of the back are ranked as the most frequent cause of limitation of activity in people. Intervertebral disc herniations are most prominent in the 3rd and 5th decades of life.[1] It accounts for a significant share of cases of low backache seen in orthopedic clinical practice and is one of the significant contributors to functional disability.
Fortunately, only 3% to 6% of lumbar disc herniations become symptomatic,[2] and the management of lumbar disc herniation has a wide range of variable modality. Conservative treatment is primarily aimed at pain reduction, by either analgesics or decreasing pressure on the nerve root without conventional surgery. Microdiscectomy is now considered as the “gold standard” for operative intervention in patients with herniated limber discs whose conservative treatment has failed. However, the success rate of this surgery was between 51% and 89%, despite advances in investigations, operative technique and postoperative care.[3,4,5]
In 1934, Mixtar and Barr study concluded that surgery could improve suffering caused by sciatica.[6] However, the vast majority of patients with sciatica do not require surgical intervention due to favorable natural history. There seems to be a consensus that surgery is indicated in carefully selected patients with severe sciatica, patients with progressive neurologic deficits, patients not improving with conservative management, cauda equina syndrome.[7]
Many previous articles announced several modalities for treating motor weakness caused by lumbar disc herniation[1,8] such as rest, drugs, physical therapy, epidural steroid injection, and surgical intervention but few randomized controlled trials that had compared the efficacy of one treatment over another treatment except cross-over treatment. The objectives of this study were to compare the effectiveness of individual surgical and nonsurgical treatment of lumbar disc herniation and to compare recovery of motor deficit in patients who are treated surgically and nonsurgically.
We monitored the intensity of low back pain by visual analog scale (VAS), motor function evaluation by Medical Research Council (MRC) scale and Oswestry Low Back Pain Questionnaire was used to assess the outcome. Preoperative and postoperative VAS scores and grades of motor deficit were documented. Similarly, Oswestry Disability Index (ODI) scores were recorded, and the rate of improvement in terms of percentage was calculated.
Subjects and Methods
This study was a prospective observational study conducted at our tertiary health care center after approval from research and ethical committee with reference no-KIMS/KIIT/IEC/169/2018. In this study, we compared the outcomes of patients with the motor deficit, who underwent surgery with the patients who took nonsurgical treatment. Both men and women between years of 20–40 age group with LDH and motor deficit were included in the study taking on account of high prevalence rate in this age group in our setup. As there is poor outcome of conservative management of patients with motor deficit for more than 6 months, we have included the patients with motor deficit of the duration of <6 months in our study. The treatment with in 1 month of onset of symptoms is considered as early and after 3 months as late. All magnetic resonance imaging (MRI) diagnosed cases of lumbar disc prolapse with signs of radiculopathy and associated neurological deficit with motor power in the range of 1/5–4/5 on MRC scale requiring hospitalization consenting to undertake, were included in the study. Patients with multiple level disc prolapse, spine infections, malignancies, low back pain other than mechanical origin and motor power of 0/5 on MRC scale were excluded.
Plain X-ray and MRI were carried out to confirm the diagnosis and know the level and type of the lesion. Patients were then counseled for both means of treatment and were explained all related complications. Surgical treatment in the form of standard lumbar open microdiscectomy was planned. The nonsurgical treatment protocol was the advice of a minimum of 3 weeks of strict bed rest. Mobilization was gradually instituted once the patient has had substantial relief of pain and muscle spasm. Bed rest was supplemented with NSAIDS or Opioids depending on the patient's tolerance and muscle relaxants. As the pain diminishes, the patient was encouraged to begin home-based spinal exercises, walking within limits of comfort was encouraged. Prolonged sitting, especially riding a car or bike was discouraged, interferential therapy and short-wave diathermy were also advised. The epidural injection of a long-acting steroid with epidural anesthetic was given if the pain has not subsided with drugs and bed rest.
We included 75 cases of lumbar disc herniation with the motor deficit after applying strict inclusion and exclusion criteria. Thirty-six patients were treated with a microdiscectomy, and 39 patients were treated conservatively prospectively from June 2018 to June 2019. All the patients were evaluated with a thorough assessment of previous history and clinical examination. MRC grade of the motor deficit, VAS Score, ODI Scores findings were documented and compared in both groups preoperatively and postoperatively at 1 month, 3 months, 6 months, and 1-year follow-ups. The ODI score was used to assess each patient's function at 1, 3, 6, and 12 months' postoperative follow-up. Good or excellent outcomes represented minimal to no disability scores of 15% or less. Fair outcomes represented levels of minimal to moderate disability scored between 15 and 30%. Poor outcomes represented levels of moderate-to-severe disability scores of>30%.[9]
In this study, we have taken MRI based three classification systems for the proper selection process of patients - (1) MSU classification (Michigan State University), (2) Pfirrmann grading system, (3) Modic Changes in endplate Classification. Statistical analysis was done using IBM Corp, released 2011, IBM SPSS Statistics for Windows, Version 20.0. (Armonk, NY: IBM Corp.) by an independent statistician. All assessments between two groups were performed by Chi-square test and RM-ANOVA noting down the P value. A P < 0.05 was considered statically significant.
Results
The mean age of all participants was 33.1 years (surgery: 33.2 years, nonsurgery: 33 years) and the ratio of male and female was 2.57-1 (male: 54, female: 21) with a mean duration of symptoms in the surgical group was 3.53 months and in nonsurgical was 3.92 months. There were no statistically significant differences recorded in patients' clinical profile relating to age, gender, and duration of symptoms between two groups.
The most common disc herniation level, disc herniation type, and disc location were at L4-L5 level (Surgical-75%, nonsurgical-82.1%), disc protrusion type (surgical-47.2%, nonsurgical-53.8%) at paracentral zone (Surgical-100%, nonsurgical-94.9%). There were no statistically significant differences on the distribution in disc herniation level, type, and location between two groups.
Events which precipitated the onset of pain were analyzed. History of lifting weights was present in 60% (45 cases), insidious onset was present in 26.6% (20 cases), and bending activity in 13.3% (10 cases). On examination, a positive SLRT (Lt sided) was the most common finding followed by restricted spinal movements.
In our study, we found that as per MCU classification, 2B type of disc herniation is common (54.7%) followed by 2AB type (42.7%). According to Pfirrmann classification, grade 3 (49.3%) being most common, followed by grade 2 (45.3%) and type 1 Modic changes are found in 28% of cases. There were no statistically significant differences in MRI findings as well as in MRI-based classification systems between the two groups. The sensory deficit was found in all patients with L5 being commonly affected dermatomes.
The assessment of differences in VAS score on back between two groups was performed using an RM-ANOVA. The effect of treatment type at each monitoring point of the follow-up period was presented in the table. There were statistically significant differences at initial follow-ups at 1 month, 3 months, and 6 months respectively between two groups and interaction between time and groups. We found that there was a tendency of rapid decrease of pain score in a surgical group within first 1-month postoperatively compared to the surgical group but at final follow-up at 12 months, no statistically significant difference is found between two groups [Table 1 and Figure 1].
| Treatment modality | Mean | Std. deviation | n | Postop_VAS_Score | Postop_VAS_Score* treatmentmodality | |
|---|---|---|---|---|---|---|
| VAS PreOp | S | 7.42 | 0.554 | 36 | P=0.000 | P=0.000 |
| NS | 6.92 | 0.580 | 39 | |||
| Total | 7.16 | 0.616 | 75 | |||
| VAS 2 month | S | 3.36 | 0.543 | 36 | ||
| NS | 5.28 | 0.647 | 39 | |||
| Total | 4.36 | 1.135 | 75 | |||
| VAS 4 months | S | 1.50 | 0.697 | 36 | ||
| NS | 3.97 | 0.584 | 39 | |||
| Total | 2.79 | 1.398 | 75 | |||
| VAS 6 months | S | 1.31 | 0.525 | 36 | ||
| NS | 2.90 | 0.754 | 39 | |||
| Total | 2.13 | 1.031 | 75 | |||
| VAS 12 months | S | 1.19 | 0.624 | 36 | ||
| NS | 1.62 | 0.847 | 39 | |||
| Total | 1.41 | 0.773 | 75 | |||
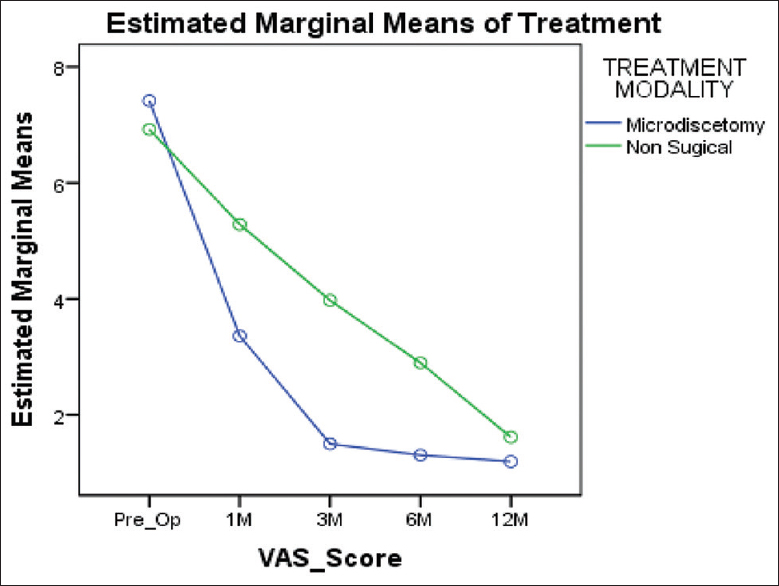
- Visual analog rating scale-showing statistically significant interaction between time and groups in early stage of follow-up period but without much difference at final follow up
The assessment of differences in ODI score between two groups was performed using an RM-ANOVA. There were statistically significant differences at initial follow-ups at 1, 3, 6 months, respectively between two groups and interaction between time and groups. At final follow-up, it was found that there is no statistically significant difference between the two groups. The results reveal that the ODI score was affected by treatment modality at the initial period. Still, it is not affected by any sort of treatment during the final follow-up period [Table 2 and Figure 2].
| Treatment modality | Mean | Std. deviation | n | PostopODI_Score | PostopODI_Score * treatmentmodality | |
|---|---|---|---|---|---|---|
| ODI PreOp | S | 68.4194 | 9.93569 | 36 | P=0.000 | P=0.000 |
| NS | 54.8956 | 11.90942 | 39 | |||
| Total | 61.3871 | 12.87602 | 75 | |||
| ODI 1 month | S | 33.9900 | 5.69285 | 36 | ||
| NS | 38.6915 | 10.03413 | 39 | |||
| Total | 36.4348 | 8.52189 | 75 | |||
| ODI 3 months | S | 22.6803 | 4.42297 | 36 | ||
| NS | 28.1641 | 6.33392 | 39 | |||
| Total | 25.5319 | 6.12058 | 75 | |||
| ODI 6 months | S | 18.1750 | 3.25507 | 36 | ||
| NS | 20.9572 | 4.82415 | 39 | |||
| Total | 19.6217 | 4.34974 | 75 | |||
| ODI 12 months | S | 12.5436 | 3.50646 | 36 | ||
| NS | 12.1905 | 4.43994 | 39 | |||
| Total | 12.3600 | 3.99622 | 75 | |||
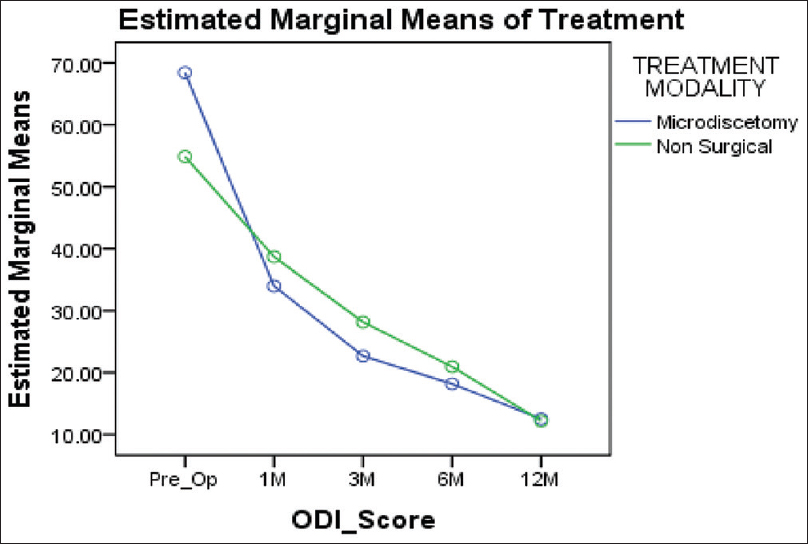
- Oswestry Disability Index score-showing statistically significant interaction between time and groups in early stage of follow up period but without much difference at final follow up
The assessment of differences in motor recovery between two groups was performed using an RM-ANOVA. The effect of treatment type at each monitoring point of follow-up period are presented in [Tables 3–5] for L4, L5, S1 myotomes, respectively, and the interaction between time course and group are shown in respective graphs following tables. There were statistically significant differences at the 1, 3-, and 6-month monitoring point of follow-up period between two groups and considerable interaction between time and group. The results reveal that a rapid motor recovery could be obtained with surgical treatment at the early stage of the follow-up period, even though the degree of motor recovery at 12th month has no significant difference. L4, L5, S1 myotomes were individually studied and found the same results in all three [Tables 3–5 and Figures 3–5]. MRC score with ≤3/5 deficit patients shown partial recovery whereas MRC ≥3/5 shown complete recovery. We did not find complete sensory recovery in any patient of our study.
| Treatment modality | Mean | Std. deviation | n | Postop_MD-L4_Score | Postop_MD-L4 * treatmentmodality | |
|---|---|---|---|---|---|---|
| Pre op MD - L4 | S | 2.75 | 0.500 | 4 | P=0.000 | P=0.045 |
| NS | 3.33 | 0.577 | 3 | |||
| Total | 3.00 | 0.577 | 7 | |||
| 1 M Post op- L4 | S | 3.75 | 0.500 | 4 | ||
| NS | 3.33 | 0.577 | 3 | |||
| Total | 3.57 | 0.535 | 7 | |||
| 3 M Post op -L4 | S | 4.25 | 0.500 | 4 | ||
| NS | 4.00 | 0.000 | 3 | |||
| Total | 4.14 | 0.378 | 7 | |||
| 6 M Post op -L4 | S | 4.75 | 0.500 | 4 | ||
| NS | 4.33 | 0.577 | 3 | |||
| Total | 4.57 | 0.535 | 7 | |||
| 12 M Post op -L4 | S | 4.75 | 0.500 | 4 | ||
| NS | 4.67 | 0.577 | 3 | |||
| Total | 4.71 | 0.488 | 7 |
| Treatment modality | Mean | Std. deviation | n | Postop_MD-L5_Score | Postop_MD-L5 * treatmentmodality | |
|---|---|---|---|---|---|---|
| Pre op MD -L5 | S | 1.81 | 0.921 | 27 | P=0.000 | P=0.000 |
| NS | 2.97 | 1.098 | 30 | |||
| Total | 2.42 | 1.164 | 57 | |||
| 1 M Post op- L5 | S | 3.11 | 0.801 | 27 | ||
| NS | 3.07 | 1.015 | 30 | |||
| Total | 3.09 | 0.912 | 57 | |||
| 3 M Post op -L5 | S | 3.81 | 0.834 | 27 | ||
| NS | 3.33 | 0.758 | 30 | |||
| Total | 3.56 | 0.824 | 57 | |||
| 6 M Post op -L5 | S | 4.33 | 0.784 | 27 | ||
| NS | 3.80 | 0.761 | 30 | |||
| Total | 4.05 | 0.811 | 57 | |||
| 12 M Post op -L5 | S | 4.67 | 0.734 | 27 | ||
| NS | 4.73 | 0.640 | 30 | |||
| Total | 4.70 | 0.680 | 57 |
| Treatment modality | Mean | Std. deviation | n | PostopS1_Score | PostopS1_Score * treatmentmodality | |
|---|---|---|---|---|---|---|
| Pre op MD -S1 | 1 | 3.40 | 0.548 | 5 | P=0.000 | P=0.031 |
| 2 | 3.83 | 0.408 | 6 | |||
| Total | 3.64 | 0.505 | 11 | |||
| 1 M Post op -S1 | 1 | 4.40 | 0.548 | 5 | ||
| 2 | 3.83 | 0.408 | 6 | |||
| Total | 4.09 | 0.539 | 11 | |||
| 3 M Post op -S1 | 1 | 5.00 | 0.000 | 5 | ||
| 2 | 4.33 | 0.516 | 6 | |||
| Total | 4.64 | 0.505 | 11 | |||
| 6 M Post op -S1 | 1 | 5.00 | 0.000 | 5 | ||
| 2 | 5.00 | 0.000 | 6 | |||
| Total | 5.00 | 0.000 | 11 | |||
| 12 M Post op -S1 | 1 | 5.00 | 0.000 | 5 | ||
| 2 | 5.00 | 0.000 | 6 | |||
| Total | 5.00 | 0.000 | 11 |
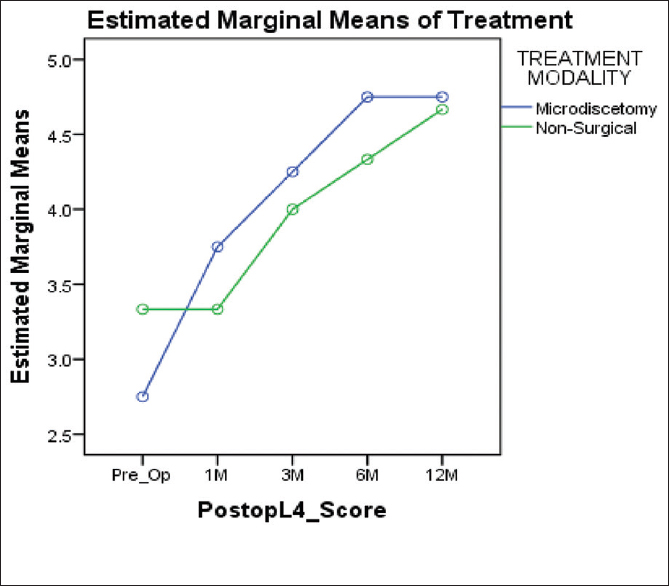
- Motor recovery of L4 myotome-a rapid motor recovery could be obtained with surgical treatment at the early stage of follow-up period, even though the degree of motor recovery at 12 months has no significant difference in L4 myotome
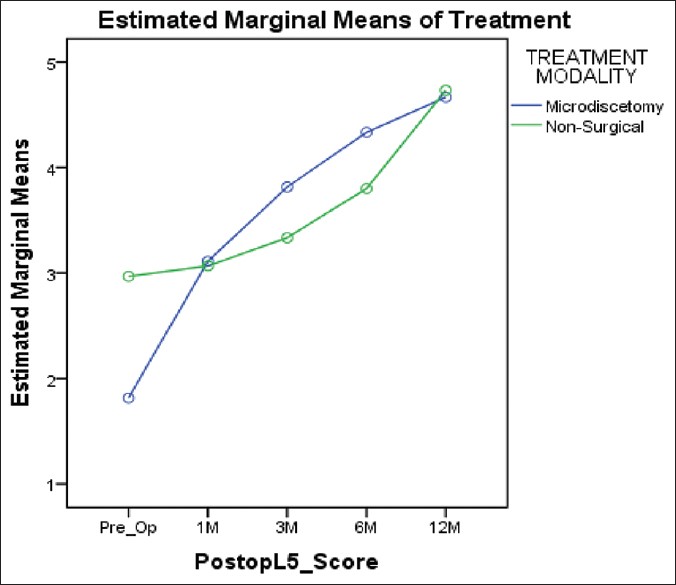
- Motor recovery of L5 myotome-a rapid motor recovery could be obtained with surgical treatment at the early stage of follow-up period, even though the degree of motor recovery at 12 months has no significant difference in L5 myotome
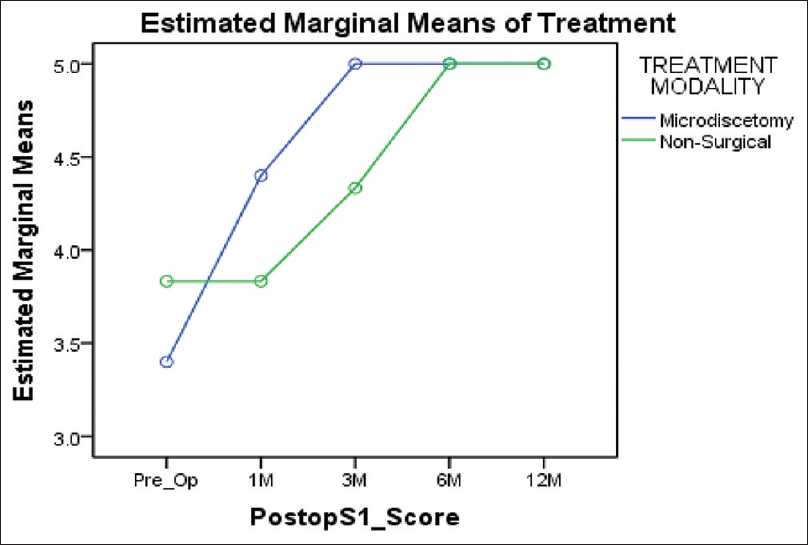
- Motor recovery of S1 myotome-a rapid motor recovery could be obtained with surgical treatment at the early stage of follow-up period, even though the degree of motor recovery at 12 months has no significant difference in S1 myotome
Discussion
For decades, the different recommendations and comparisons among surgical and conservative treatment for patients with lumbar disc herniation were published. Patients with mild symptoms did well, regardless of the treatment. Patients, who presented with mild weakness were tried with a wide variety of nonoperative treatment such as bed rest, lumbar braces, oral analgesics, muscle relaxants, spinal manipulation, physiotherapy, behavioral therapy, and epidural steroid injection.[10,11,12,13] For those with moderate or severe symptoms, surgery may facilitate recovery and result in better outcomes compared with nonsurgical treatment. In addition, some patients need surgical intervention due to progressive neurological deficit and prolonged or uncontrolled pain.[14]
In 2001, the larger Maine Lumbar Spine Study, from their 5-year study, showed that 15% of patients who initially received conservative treatment would undergo surgical intervention within 3 months.[15] In 2002, Postacchini et al., in his study found, complete recovery of motor deficits after microdiscectomy for lumbar disc herniation in 76% of patients, with a mild deficit in 16% of patients and with a severe deficit in 39% of patients. With exception to four patients, all other remaining patient had grade 4 muscle power.[16]
In 2004, Buttermann in his study of treatment of lumbar disc herniation compared epidural steroid injection with discectomy. The study concluded that the patients who had undergone discectomy had shown early recovery from both motor and sensory symptoms with a success rate of 92% to 98%. In only 42% to 56% of patients, epidural steroid injection was reported to be effective, and rest who did not obtain relief from the epidural injection had a subsequent discectomy.[17] In 2008, Peul et al. randomly assigned 141 patients with sciatica to early surgery (at a mean of 2.2 weeks) and 142 patients with the same symptom to conservative management. Of those managed conservatively, 55 patients (38.7%) were converted to surgery after a mean of 18.7 weeks. They found that those patients who undertaken an early operation were relieved in their leg pain more quickly than another one with the delayed operation.[18]
In 2009, Ghahreman et al., in his study, concluded that younger patients made a better recovery of ankle dorsiflexion weakness, following decompressive lumbar surgery.[19] In 2013, Overdevest et al., in his study concluded that although a faster recovery of the motor deficit was achieved by the surgical intervention, compared with prolonged conservative treatment but the difference between the two modalities were not significant during the follow-up examination at 1 year.[20]
In 2013, Choi et al. conducted a prospective cohort study on surgical versus conservative treatment option for lumbar disc herniation with motor weakness. As per their observation, proper surgical treatment in a case of motor weakness from disc herniation could be a good way for providing a chance for rapid alleviation.[1] In 2014 Balaji et al. reviewed the literature related to the recovery of severe motor deficit secondary to herniated lumbar disc prolapse and found that complete recovery was seen in 38.4% of patients following surgery and 32% following nonoperative treatment. Based on literature review, they identified that there is a 6.4% difference in recovery rate between the collective operative and nonoperative groups.[21] In 2019, Ondra et al. in his study advocated considering immediate surgery for neurological recovery in acute moderate/severe herniated lumbar disc prolapse.[22]
There are several reasons that long-term outcomes of patients with a herniated lumbar disc were similar to surgical and conservative treatment. A study reported in 2006 by Autio et al., in which 68 of 160 enrolled patients (42.5%) documented by lumbar MRI revealed a diminished volume of herniated lumbar disc 2 months later since the occurrence of the disease.[23,24,25] In the other studies, the occurrence rate of spontaneous regression of herniated lumbar disc was around 35%–63% on average, from 6 months to 1 year.[23,25,26] This phenomenon may be related to dehydration or shrinkage, retraction of herniated discs, and inflammation-related resorption of the herniated disc.[8,25,27,28]
Compared to the above studies, the findings of our research in terms of various factors related to the outcome were similar. In our study, we found that there was no significant correlation between outcome and the sex in both modalities of treatment. The age group in inclusion criteria was 20–40 years. There was no significant difference in age-wise outcome found, but younger population shows faster recovery compared to elder groups in both modalities of treatment. In our series, we found that there is no statistical difference between outcomes early and late treatment at final follow-up. However, patients who took early surgical treatment shown faster recovery. In our research, the surgical group has shown speedier recovery of motor deficit both mild (MRC ≥3) and severe (MRC ≤3) irrespective of age, sex and duration at 1st month, 3rd month, and 6th month compared to a conservative group. We found that 97.2% who underwent surgical modality recovered motor deficit by at least one grade at the end of 1 month compared to 7.7% in the nonsurgical group. At the end of 3 months, all patients recovered by at least one grade whereas 38.4% in the nonsurgical group. At 6 months, 61.1% recovered entirely in the surgical group compared to 15.9% in the nonsurgical group. The results reveal that a rapid motor recovery could be obtained with surgical treatment at the early stage of the follow-up period. However, in the final follow-up at 12 months, the outcome shown no significant difference. Complete recovery of severe deficits was found in the surgical group compared to only mild deficits recovered entirely in the conservative group.
In ODI score comparison, the statistically significant difference seen in initial follow-ups at 1, 3, 6 months respectively between two groups with better improvement of overall health quality of life shown by the surgical group. In the final follow-up, 76.9% showed good/excellent outcome in the surgical group, 80.5% in the nonsurgical group. At the end of 12 months, it was found that there is no statistical difference in outcome measures in both the groups. The pain was reduced to minimal pain with VAS score 2-3 in 66.7% of patients, who were treated with surgical intervention. In the nonsurgical group, none of the patients reported a reduction in pain to VAS score 2-3 at the end of 1 month. 97.2% of patients reported a decrease in pain with VAS to score 2-3 at the end of 3 months in the surgical group whereas 7.7% patients showed similar results at the end of 3 months in the nonsurgical group. Results show that there was a tendency of rapid decrease of pain score in a surgical group in initial follow-ups compared to the nonsurgical group but at final follow-up at 12 months, no statistically significant difference is seen.
The patients were treated surgically in this study had better outcomes of motor weakness than the nonsurgical group at the early stage of the follow-up period, even though the degree of motor recovery at 12th month has no significant difference. In addition, the improvement of pain symptoms and functional status was better seen in the surgical group at 1, 3, 6 months' follow-ups compared to the nonsurgical group but shown similar outcomes at the end of 1 year. The motor recovery was prompt in the surgical group compared to the nonsurgical group initially but showed a similar result in the end. Besides, there were also the alleviation for pain on back and leg from a surgical modality, even if we could not find out statistically significant differences at the end. The limitations of this study were inadequate to follow-up and relatively small sample size.
Conclusion
Several conclusions can be drawn from our study. Surgical treatment showed more benefits on the recovery of motor function in the short-term period, especially 1 month and 3 months compared to the conservative one statistically. We can also expect to obtain a rapid recovery on pain symptom with surgical modality within the first 1 month postoperatively. We believe that early surgical treatment in a case of motor weakness from disc herniation could be the right way for providing a chance for rapid alleviation. Faster recovery of the motor deficit was achieved by the surgical intervention, compared with prolonged conservative treatment but the difference between the two modalities were not significant during the follow-up examination at 1 year. At the end of the final follow-up, both modalities of treatment showed almost the same results. ODI scores also showed better improvement in the quality of life at the initial 3 months' period in the surgical group compared to the nonsurgical group. Still, they showed similar results in both groups in the final follow-up. The surgical group has shown faster recovery of motor deficit.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Surgical versus conservative treatment for lumbar disc herniation with motor weakness. J Korean Neurosurg Soc. 2013;54:183-8.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of bad and good outcomes of lumbar disc surgery. A prospective clinical study with recommendations for screening to avoid bad outcomes. Spine (Phila Pa 1976). 1995;20:460-8.
- [CrossRef] [PubMed] [Google Scholar]
- Outcome analysis in 654 surgically treated lumbar disc herniations. Neurosurgery. 1992;30:862-6.
- [CrossRef] [PubMed] [Google Scholar]
- A long-term outcome analysis of 984 surgically treated herniated lumbar discs. J Neurosurg. 1994;80:415-21.
- [CrossRef] [PubMed] [Google Scholar]
- Rupture of the intervertebral disc with involvement of the spinal canal. N Engl J Med. 1934;211:210-5.
- [CrossRef] [Google Scholar]
- CT demonstration of disk regression after conservative therapy. AJNR Am J Neuroradiol. 1984;5:632-3.
- [Google Scholar]
- Surgery versus conservative management of sciatica due to a lumbar herniated disc: A systematic review. Eur Spine J. 2011;20:513-22.
- [CrossRef] [PubMed] [Google Scholar]
- MSU classification for herniated lumbar discs on MRI: Toward developing objective criteria for surgical selection. Eur Spine J. 2010;19:1087-93.
- [CrossRef] [PubMed] [Google Scholar]
- Herniated lumbar disc. BMJ Clin Evid. 2009;2009:1118. PMID: 19445754; PMCID: PMC2907819
- [Google Scholar]
- Surgery versus prolonged conservative treatment for sciatica. N Engl J Med. 2007;356:2245-56.
- [CrossRef] [PubMed] [Google Scholar]
- Radiculopathy and the herniated lumbar disc. Controversies regarding pathophysiology and management. J Bone Joint Surg Am. 2006;88:2070-80.
- [CrossRef] [PubMed] [Google Scholar]
- The management of weakness caused by lumbar and lumbosacral nerve root compression. J Bone Joint Surg Br. 2012;94:1442-7.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: Five-year outcomes from the Maine Lumbar Spine Study. Spine (Phila Pa 1976). 2001;26:1179-87.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical and non-surgical management of sciatica secondary to a lumbar disc herniation: Five-year outcomes from the Maine Lumbar Spine Study. Spine (Phila Pa 1976). 2001;26:1179-87.
- [CrossRef] [PubMed] [Google Scholar]
- Recovery of motor deficits after microdiscectomy for lumbar disc herniation. J Bone Joint Surg Br. 2002;84:1040-5.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of lumbar disc herniation: Epidural steroid injection compared with discectomy. A prospective, randomized study. J Bone Joint Surg Am. 2004;86:670-9.
- [CrossRef] [PubMed] [Google Scholar]
- Leiden-The Hague Spine Intervention Prognostic Study Group. Prolonged conservative care versus early surgery in patients with sciatica caused by lumbar disc herniation: Two year results of a randomized controlled trial. BMJ. 2008;336:1355-8.
- [CrossRef] [PubMed] [Google Scholar]
- Recovery of ankle dorsiflexion weakness following lumbar decompressive surgery. J Clin Neurosci. 2009;16:1024-7.
- [CrossRef] [PubMed] [Google Scholar]
- Recovery of motor deficit accompanying sciatica - Subgroup analysis of a randomized controlled trial. Spine J. 2014;14:1817-24.
- [CrossRef] [PubMed] [Google Scholar]
- Recovery of severe motor deficit secondary to herniated lumbar disc prolapse: Is surgical intervention important? A systematic review. Eur Spine J. 2014;23:1968-77.
- [CrossRef] [PubMed] [Google Scholar]
- Immediate versus delayed surgical treatment of lumbar disc herniation for acute motor deficits. Spine. 2019;44:454-63.
- [CrossRef] [PubMed] [Google Scholar]
- Determinants of spontaneous resorption of intervertebral disc herniations. Spine (Phila Pa 1976). 2006;31:1247-52.
- [CrossRef] [PubMed] [Google Scholar]
- The natural history of lumbar degenerative spinal stenosis. Joint Bone Spine. 2002;69:450-7.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous regression of lumbar herniated disc. J Chin Med Assoc. 2009;72:650-3.
- [CrossRef] [PubMed] [Google Scholar]
- The natural history of herniated nucleus pulposus with radiculopathy. Spine (Phila Pa 1976). 1996;21:225-9.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous regression of a large lumbar disc herniation: Report of an illustrative case. Surg Neurol. 2001;56:333-6.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous regression of herniated nucleus pulposus. Am J Roentgenol. 1985;145:371-5.
- [CrossRef] [PubMed] [Google Scholar]




