
Translate this page into:
A comparative retrospective analysis of indoor patients between 50 to 85 years of age suffering from osteoarthritis to determine the effectiveness of epidural and intravenous tramadol in pain relief and functional recovery after total knee replacement surgery
Address for correspondence: Dr. Kedar Anil Parelkar, Department of Orthopaedics, D.Y. Patil Hospital and Research Centre, Nerul, Navi Mumbai, Maharashtra, India. E-mail: kedarparelkar@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Butala R, Parelkar KA, Pandey A. A comparative retrospective analysis of indoor patients between 50 to 85 years of age suffering from osteoarthritis to determine the effectiveness of epidural and intravenous tramadol in pain relief and functional recovery after total knee replacement surgery. J Orthop Spine 2021;9:17-24.
Abstract
BACKGROUND:
Total knee replacement surgery is among the most common major orthopedic surgery performed in cases of osteoarthritis on the knee joint. Total knee arthroplasty is considered to cause moderate-to-severe postoperative pain. No clear consensus in the available literature suggests a clear advantage between epidural tramadol and intravenous tramadol postoperatively due to the complications associated with an epidural catheter.
AIM:
This study aimed to determine the effectiveness of epidural tramadol and intravenous tramadol in pain relief and functional recovery in postoperative total knee replacement patients.
MATERIALS AND METHODS:
All cases operated for total knee replacement and postoperatively managed by epidural tramadol and intravenous tramadol were studied. This group included 20 patients of total knee replacement managed by epidural tramadol compared to 20 patients of total knee replacement managed by intravenous tramadol.
RESULTS:
Patients in the group managed postoperatively with intravenous tramadol for postoperative pain management showed a better functional outcome and pain relief as compared to patients managed with epidural tramadol. It was noted that in patients managed with intravenous tramadol, the knee range of motion and static and dynamic quadriceps exercises were started earlier and the patients were more compliant, which intern helped to achieve a better functional outcome posttotal knee replacement surgery.
CONCLUSION:
We would like to suggest in our limited 40 patient study group, the pain managed in patients by intravenous tramadol showed a better functional outcome as compared to the pain managed in the patients by epidural tramadol.
Within our study group of 40 patients, it was noted that patient compliance and comfort was better in cases where tramadol was administered through an intravenous line as compared to an epidural catheter with no statistically significant difference in postoperative pain as well as functional outcome and recovery.
Keywords
Epidural catheter
intravenous injection
total knee replacement surgery
tramadol

Introduction
In modern surgical practice analgesia and postoperative pain, management holds a very important place and should be given due importance. Total knee arthroplasty is considered to cause moderate to severe post-operative pain.[1] Inadequate or poorly treated postoperative pain after total knee replacement surgery not only significantly prolongs the rehabilitation process, increased risk of other complications, sometime progress as persistent postoperative pain into chronic pain and it also prolonged the overall length of hospitalization and cost.[2] Early joint mobilization with the initiation of physical therapy is one of the important aspects to achieve successful outcomes after total knee arthroplasty.[3]
The available analgesics options after total knee replacement surgery are as follows:-
-
Preoperative analgesia:
At least 1 h prior to incision use of analgesics opioid, nonsteroidal anti-inflammatory drugs (NSAIDs), cyclooxygenase (cox-2) inhibitor, and gabapentanoid (gabapentin and pregabalin) have been shown to reduce the central and peripheral sensitization of pain mechanism and thereby reduce short- and long-term postoperative pain level and decrease the need of rescue analgesics in postoperative period[4,5,6,7,8,9]
-
Intraoperative local infiltration:
Intra- and extra-articular injections of long-acting local anesthetic agents which may or may not include opioids can be used to reduce the pain significantly. Commonly used drugs are bupivacaine, ropivacaine, morphine, steroids, epinephrine, etc
-
Epidural analgesia:
An epidural catheter placed while giving spinal anesthesia before the surgery can be used to continuously provide analgesia 48 h after surgery. This method is compared by many as a gold standard, however, it does have many drawbacks as well such as the risk of bladder and bowel dysfunction, pruritus, and in some cases, respiratory depression. Due to these effects, its uses have reduced and alternative managements for postoperative analgesia are being studied and alternative methods looked into[10,3]
-
Systemic analgesics (opioid/nonopioid):
Opioids/nonopioids given through intravenous route are also being studied. Postoperative intravenous tramadol can be considered as tramadol is considered a low-risk opioid option for the treatment of moderate-to-severe pain
-
Regional blocks:
Multiple regional blocks can be considered as well such as femoral nerve block, adductor canal block, and sciatic and selective tibial nerve block. The main drawbacks to any block however are muscle weakness and impaired proprioception which can increase the risk of the patient falling
-
Multimodal analgesia:
The increasingly common trend followed by many orthopedic surgeons is to use one or more of the above-mentioned methods with one or more drug combinations to achieve the required results. These methods may have an additive and synergistic effect while minimizing the side effect of each drug.[11] It is a holistic approach for postoperative pain with a goal to maximize the analgesic effect and minimize the side effects of the medications.[12,13,14]
The considered gold standard for postoperative pain management is through the epidural catheter; however, the complications associated with the same are many such as the risk of respiratory depression, bladder and bowel dysfunction, pruritus, and in some cases, respiratory depression. The available literature suggests that intravenous tramadol can also be used for moderate-to-severe pain management and has fewer complications. Hence, we decide to raise a research question to analyze the effectiveness of epidural tramadol and intravenous tramadol in pain relief and functional recovery in postoperative total knee replacement patients.
The aim of the study was to analyze the effectiveness of epidural and intravenous tramadol in pain relief and functional recovery.
Primary objective was to study the effects of intravenous tramadol in postoperative total knee replacement patients based on the questionnaires of verbal rating pain scale and the hospital of special surgery knee score submitted by patients.
Secondary objective was to compare and analyze the effectiveness of intravenous tramadol to intravenous tramadol and study the advantages and disadvantages of each.
Materials and Methods
All cases admitted at tertiary care center with osteoarthritis (OA) of knee joint and operated with a total knee replacement surgery were studied.
All cases admitted at the tertiary care center with OA of the knee joint and operated with a total knee replacement surgery were contacted and asked to fill out a questionnaire based on the hospital special surgery (HSS) and verbal rating scale (VRS) scoring system and the data collected was retrospectively compared and studied.
The eligibility criteria were based on the inclusion and exclusion criteria mentioned below:
Inclusion criteria included
Unilateral total knee replacement patients
Age 50–85 years old
Nontraumatic cases.
Exclusion criteria
Bilateral total knee replacement patients
Age younger than 50 and older than 85 years' old
Known cases of rheumatoid arthritis
Known cases of scoliosis, kyphosis, and lordosis
Known cases of ankylosing spondylitis.
A total of 40 patients admitted with a diagnosis of primary OA of the knee and those who required a total knee replacement surgery were included in the study after obtaining informed written consent from each subject based on the inclusion and exclusion criteria mentioned above. Patients of either gender were included in the study and a retrospective comparative analysis was done between 20 cases of postoperative total knee replacement patients managed postoperatively with epidural tramadol against 20 cases of postoperative total knee replacement patients managed postoperatively with intravenous tramadol injections for 48 h.
All procedures were performed by surgeons of similar levels of training. The study protocol was approved by the department of orthopedics and was conducted as per the good clinical practice guidelines and the principles laid down in the Declaration of Helsinki.
Preoperative data such as age, sex, weight, preoperative deformity, and preoperative knee function were collected.
Steps for spinal and epidural anesthesia
All patients were given spinal +epidural anesthesia in the sitting position on the OT table. The lumbar region was scrubbed painted and draped. The L4 level was located with the reference to the iliac crest and two levels above, that is the L2–L3 levels, were selected, and with the help of the Tuohy needle, the epidural space was breached as negative pressure within the space was felt and 1 cc normal saline was injected to expand the space. The epidural catheter (16G) was inserted at this level (L2–L3). Spinal anesthesia was given at the level of L4–L5 with 3 to 3.5 ml of 0.5 bupivacaine which also contained 0.8% dextrose. The expected time for the spinal to last was estimated between 2 and 2 and ½ h. The patient was asked to lie in the supine position for 5 to 10 min for the spinal anesthesia to act, after which the surgeon was given a go-ahead to start.
Surgery
Tourniquet was applied and scrubbing, painting, and draping of the operative limb were done.
A median parapatellar incision was taken which extended from the tendinous insertion of the quadriceps femoris on the patella to the medial aspect of the tibial tuberosity. The knee was kept in a flexed position while taking the incision. The femoral cuts are taken using an intermeduallary guiding system and a conventional total knee replacement surgery was done. A negative pressure drain was fixed for 48 h. In patients where the epidural catheter was to be kept in situ for 48 h postoperatively, the epidural catheter was activated by injecting 3cc lignocaine with adrenaline, on injecting this, two parameters were monitored, namely the BP to watch for fall of BP, incase the catheter was in the subarachnoid space, and the heart rate to watch for tachycardia, in case the catheter was communicating with some vascular structure.
Data of 20 patients in whom the epidural catheter was left in situ and 20 patients in whom the epidural catheter was removed were collected from the records kept and were analyzed.
A record of all patients operated is maintained in the operation theater register with surgeries performed and patient details, a list of total knee replacement patients was made based on the eligibility criteria and the patients were contacted and after proper consent, a questionnaire based on the HSS and VRS scoring system was sent to them and after completion of the questionnaire, the data were analyzed and studied. We do not keep and measure all HSS subscores and VRS scores).
Postoperative management
All patients were administered iv antibiotic doses to prevent infections, also to prevent deep-vien thrombosis, all patients were given low-molecular weight heparin (0.4/0.6 clexane) postoperatively after 8 h, after which the patients were started on rivaroxaban (Xarelto) for 14 days and after this, all patients were started on ecosprin 75 mg for 3 months.
For analgesia patients with the epidural catheter, injection tramadol through the epidural catheter with intravenous ondansetron was given at intervals of 12 h with intravenous analgesics in case required. The dose of tramadol given through the epidural catheter was 1cc diluted in 9cc normal saline. The drug was injected through the catheter after negative aspiration was done to check for blood or cerebrospinal fluid.
For analgesia in patients without epidural catheters, intravenous injection tramadol was given at 12-h intervals. Depending on the patients build either 50 mg diluted in 100 ml normal saline or 100 mg diluted in 500 ml normal saline slowly was given.
Postoperative data such as
Postoperative pain was evidenced by verbal rating pain score, postoperative passive flexion, postoperative nonassisted straight leg raising, length of hospital stay, amount of blood loss (drain in first 24-h), length of incision, and tourniquet time. In addition, postoperative knee functional HSS scores including postoperative range of motion (ROM) was also recorded.
Statistical analysis
Statistical analysis was done using Windows-based program Statistical Package for the Social Sciences version 17. The age and other measurement data (blood loss, surgery duration, and incision length) were compared between the two groups using an independent sample t-test, whereas the scores for the VRS and HSS subscales and total scores were compared between the two groups using Mann–Whitney: “U” test (nonparametric). Discrete data for the VRS scale and HSS subscales were analyzed using the Chi-square test, all analyses were done using two-sided tests at alpha 0.05 (95% confidence level), and the verbal rating pain scores were compared as well.
VRS: In this particular scale, various adjectives are used to describe the various levels of pain. Similar to the visual analog pain scale, two endpoints were decided at two extremes as follows:-
No pain
No pain at rest and slight pain on movement.
Slight pain at rest and moderate pain on movement
Moderate pain at rest and severe pain on movement
Severe pain at rest and on movement.
HSS:-HSS scale evaluated the following:
The HSS knee score is based on a total of 100 points [Table 1]. The score is divided into seven categories, which include pain, function, ROM, muscle strength, flexion deformity, instability, and subtractions as mentioned below:
| Pain on walking |
| No pain on walking-15 |
| Mild pain-10 |
| Moderate pain-5 |
| Severe pain-0 |
| Pain at rest |
| No pain at rest-15 |
| Mild pain-10 |
| Moderate pain-5 |
| Severe pain-0 |
| Function |
| Walking and standing unlimited-12 |
| Walking 5-10 blocks/standing<2-10 h |
| Walking 1-5 blocks/standing 1/2-8 h |
| Walking<1 block-4 |
| Climbing stairs |
| Without support-5 |
| With support-2 |
| Transfer activity |
| Without support-5 |
| With support-2 |
| Range of motion (degrees) |
| 18 points (144)-18 |
| 17 points (136)-17 |
| 16 points (128)-16 |
| 15 points (120)-15 |
| 14 points (112)-14 |
| 12 points (96)-12 |
| 10 points (80) 10 |
| 8 points (64)-8 |
| Strength |
| Excellent-10 |
| Good-8 |
| Fair-4 |
| Poor-0 |
| Flexion deformity |
| No deformity-10 |
| <5 degree deformity-8 |
| 5-10 degree deformity-5 |
| >10 degree deformity-0 |
| Instability (degrees) |
| No instability-10 |
| Mild instability (0-5)-8 |
Moderate instability (5-10)-5
Results
In all postoperative patients, injection pantacid and injection emeset were given in the first 24 h and no episode of vomiting was noted.
The records of a total of 40 total knee patients were retrospectively analyzed. The age group of the patients ranged from 50 to 85 years of age, with a mean age calculated to be 63.65 years [Table 2 and Table 3]. The patients were divided into two groups. The group of postoperative total knee replacement patients managed with intravenous tramadol (n = 20) showed a better HSS score and a better VRS verbal pain rating score as compared to the group of postoperative total knee replacement patients managed with epidural tramadol (P = 0.0618) on HSS score and (P = 0.5408) on the verbal pain rating scale [Figures 1–3, Table 4 and Table 5]. The study conducted by us indicated few complications in intravenous tramadol as compared to epidural tramadol patients with a similar result in pain management and patient comfort with an intravenous line was more as compared to an epidural catheter. Hence even though the “P” value may not be statistically significant, the patient comfort and compliance was more for tramadol administered through intravenous line as compared to epidural catheter. Most patients had adequate pain relief postoperatively through both intravenous and epidural route of tramadol, one patient among the patients managed with intravenous tramadol and two patients managed with epidural tramadol complained of severe pain at rest. Among the intravenous tramadol group in 14 patients and among the epidural tramadol group in 12 patients, complaints ranged from no pain-to-moderate pain on movement. No case of postoperative infection or incision site-related complications was noted in either group. In the group manage with epidural tramadol, one patient complained of mild dizziness and burning sensation over bilateral lower limbs for about 5 min, all vital parameters were monitored and a mild drop in blood pressure was noted; however, all parameters returned back within normal range after 5 min and before the next dose of epidural tramadol in this patient, the patient was reassured and no significant changes in parameter or no similar complaints were noted. Patients in both the groups were given postoperative intravenous antibiotics for 5 days and in the group managed with intravenous tramadol, the same intravenous line was used to administer all antibiotics, analgesics, and other drugs when required.
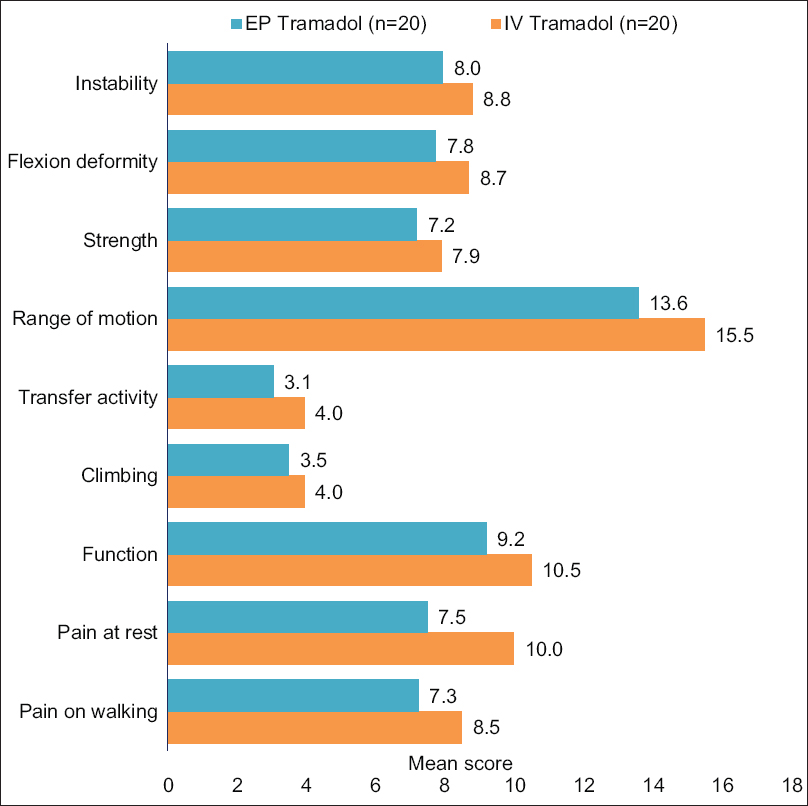
- Mean scores for hospital special surgery subscales
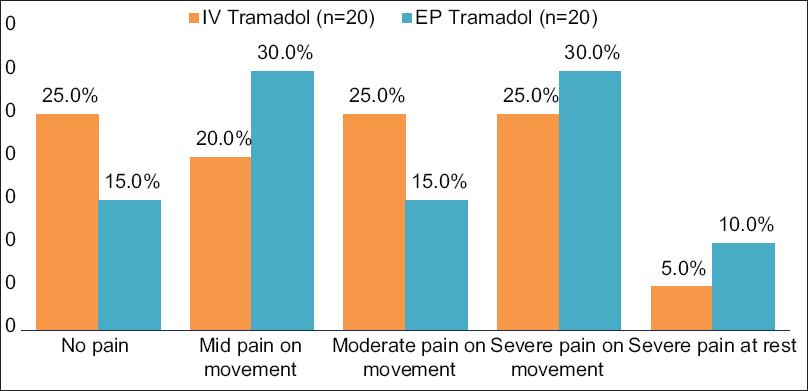
- Verbal rating scale ratings for post-operative pain
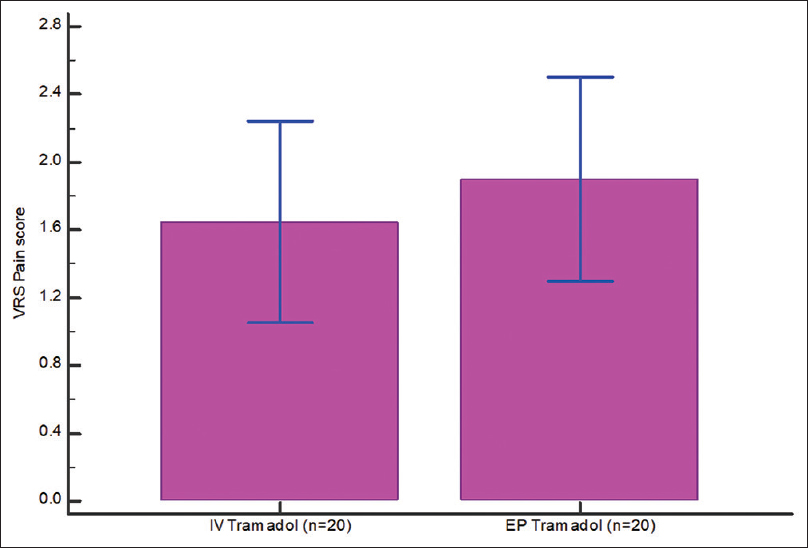
- Verbal rating scale Pain score (IV Tramadol vs. EP Tramadol)
| Intravenous tramadol | Epidural tramadol | P t-test | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age (years) | 63.65 | 6.88 | 62.60 | 6.64 | 0.6264 |
| Blood loss (ml) | 347.60 | 9.72 | 293.35 | 6.69 | <0.0001 |
| Surgery duration (min) | 65.60 | 3.73 | 85.00 | 4.66 | <0.0001 |
| Intravenous tramadol, n (%) | Epidural tramadol, n (%) | Chi-square test | |||
| Gender | |||||
| Male | 11 (55.0) | 9 (45.0) | 0.5323 | ||
| Female | 9 (45.0) | 11 (55.0) | |||
| Operated side | |||||
| Left | 12 (60.0) | 8 (40.0) | 0.2117 | ||
| Right | 8 (40.0) | 12 (60.0) | |||
SD: Standard deviation
| VRS rating | Intravenous tramadol, n (%) | Epidural tramadol, n (%) | Chi-square test (P) |
|---|---|---|---|
| No pain | 5 (25.0) | 3 (15.0) | 0.768 |
| Mid pain on movement | 4 (20.0) | 6 (30.0) | |
| Moderate pain on movement | 5 (25.0) | 3 (15.0) | |
| Severe pain on movement | 5 (25.0) | 6 (30.0) | |
| Severe pain at rest | 1 (5.0) | 2 (10.0) |
VRS: Verbal Rating Scale
| Intravenous tramadol | Epidural tramadol | Mann-Whitney U-test (nonparametric) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | SD | Mean | Median | SD | Differences | 95% CI | P | |
| Pain on walking | 8.5 | 10 | 4.3 | 7.3 | 5 | 4.7 | −1.25 | −4.15-1.65 | 0.3992 |
| Pain at rest | 10.0 | 10 | 4.3 | 7.5 | 7.5 | 3.4 | −2.50 | −4.99-−0.01 | 0.0423 |
| Function | 10.5 | 11 | 2.0 | 9.2 | 10 | 2.3 | −1.30 | −2.68-0.08 | 0.0321 |
| Climbing | 4.0 | 5 | 1.5 | 3.5 | 3.5 | 1.5 | −0.45 | −1.41-0.51 | 0.3434 |
| Transfer activity | 4.0 | 5 | 1.5 | 3.1 | 2 | 1.5 | −0.90 | −1.84-0.04 | 0.0610 |
| Range of motion | 15.5 | 16 | 2.6 | 13.6 | 14 | 2.2 | −1.90 | −3.44-−0.36 | 0.0038 |
| Strength | 7.9 | 8 | 2.8 | 7.2 | 8 | 2.3 | −0.70 | −2.33-0.93 | 0.1659 |
| Flexion deformity | 8.7 | 9 | 1.6 | 7.8 | 8 | 1.8 | −0.95 | −2.05-0.15 | 0.0786 |
| Instability | 8.8 | 10 | 1.6 | 8.0 | 8 | 2.0 | −0.85 | −1.99-0.29 | 0.1467 |
| Total score | 77.1 | 82.5 | 18.7 | 67.0 | 66 | 17.4 | −10.10 | −21.64-1.45 | 0.0618 |
| VRS pain score | 1.65 | 2.00 | 1.26 | 1.90 | 2.00 | 1.29 | 0.250 | −0.57-1.07 | 0.5408 |
VRS: Verbal Rating Scale, SD: Standard deviation, CI: Confidences interval
| Intravenous tramadol, n (%) | Epidural tramadol, n (%) | Chi-square test (P) | |
|---|---|---|---|
| Pain on walking | |||
| No pain on walking | 4 (20.0) | 3 (15.0) | 0.7483 |
| Mild pain | 7 (35.0) | 6 (30.0) | |
| Moderate pain | 8 (40.0) | 8 (40.0) | |
| Severe pain | 1 (5.0) | 3 (15.0) | |
| Pain at rest | |||
| No pain at rest | 6 (30.0) | 1 (5.0) | 0.139 |
| Mild pain | 9 (45.0) | 9 (45.0) | |
| Moderate pain | 4 (20.0) | 9 (45.0) | |
| Severe pain | 1 (5.0) | 1 (5.0) | |
| Function | |||
| Walking and standing unlimited | 10 (50.0) | 4 (20.0) | 0.1739 |
| Walking 5-10 blocks/standing<2 h | 7 (35.0) | 8 (40.0) | |
| Walking 1-5 blocks/standing 1/2 h | 2 (10.0) | 6 (30.0) | |
| Walking<1 block | 1 (5.0) | 2 (10.0) | |
| Climbing stairs | |||
| Without support | 13 (65.0) | 10 (50.0) | 0.3434 |
| With support | 7 (35.0) | 10 (50.0) | |
| Transfer activity | |||
| Without support | 13 (65.0) | 7 (35.0) | 0.061 |
| With support | 7 (35.0) | 13 (65.0) | |
| Range of motion (degrees) | |||
| 18 points (144) | 5 (25.0) | 2 (10.0) | 0.0082 |
| 17 points (136) | 1 (5.0) | 0 | |
| 16 points (128) | 7 (35.0) | 2 (10.0) | |
| 15 points (120) | 3 (15.0) | 0 | |
| 14 points (112) | 2 (10.0) | 8 (40.0) | |
| 12 points (96) | 0 | 6 (30.0) | |
| 10 points (80) | 1 (5.0) | 2 (10.0) | |
| 8 points (64) | 1 (5.0) | 0 | |
| Strength | |||
| Excellent | 9 (45.0) | 4 (20.0) | 0.2166 |
| Good | 7 (35.0) | 10 (50.0) | |
| Fair | 3 (15.0) | 6 (30.0) | |
| Poor | 1 (5.0) | 0 | |
| Flexion deformity | |||
| No deformity | 10 (50.0) | 5 (25.0) | 0.2045 |
| <5° deformity | 8 (40.0) | 10 (50.0) | |
| 5-10° deformity | 2 (10.0) | 5 (25.0) | |
| >10° deformity | 0 | 0 | |
| Instability (degrees) | |||
| No instability | 11 (55.0) | 7 (35.0) | 0.3261 |
| Mild instability (0-5) | 7 (35.0) | 8 (40.0) | |
| Moderate instability (5-10) | 2 (10.0) | 5 (25.0) |
Discussion
Literature has shown that epidural analgesia is more efficacious than the systemic analgesia for postoperative pain relief in the lower limb orthopedic surgery.[15] Choi et al. in their systemic review reported that patients receiving epidural analgesia in elective knee and hip surgeries had less pain at rest, especially in the first 4–6 h postoperative.[16] Addition of an opioid drug to the LA infusion has proven to decrease pain scores and improve patient satisfaction.[11,15,17] However, it has its some drawbacks or side effects such as hemodynamic instability, bladder and bowel dysfunction, unintended motor blockade, it makes patient confined to bed, pruritus, and risk of respiratory depression, because of these effects, its routine use is slowly declining and varieties of other regional analgesic techniques are being evaluated.[18,19]
However, some studies show that epidural anesthesia is associated with many adverse effects, such as urinary retention, hypotension, pruritus, and motor block.[20,21,22] A meta-analysis by Li et al. of seven Randamiszed control trial s, with 251 patients undergoing total knee arthroplasty, concluded that local infiltration anesthesia was as effective as epidural anesthesia for pain control.[23] However compared with parenteral opioids, epidural analgesia provides better postoperative analgesia with less nausea, vomiting, and pruritus.[24]
Recently, Mikami J et al. reported that the combination of tramadol and acetaminophen has been shown to be feasible for subacute postoperative pain management after TKA.[25] In the above study conducted by Mikami J et al., it was concluded that group Tramadol/Acetaminophen was shown to be superior to that of NSAID for postoperative pain reduction and the number of days required for walking after total knee arthroplasty. Thus, tramadol seems to be effective for relieving postoperative pain.
Successful postoperative rehabilitation program most importantly revolves around early mobilization, achieving full ROM and patient satisfaction; all three of these factors heavily rely on a good postoperative pain management protocol. With the advent of multiple pain management, options include
Preoperative analgesia (1 h before surgery with the help of opioid, NSAIDs, cox-2 inhibitor, and gabapentanoid [gabapentin and pregabalin])
Intraoperative local infiltration with the help of bupivacaine, ropivacaine, morphine, steroids, and epinephrine
Epidural analgesia with the help of drugs such as bupivacaine, tramadol, and fentanyl
Systemic analgesics (opioid/nonopioid), for example, tramadol
Regional blocks such as femoral nerve block, adductor canal block, and sciatic and selective tibial nerve block.
Selecting a good postoperative pain management protocol which shows minimum number of complications, good patient compliance, ease of administration, and least number of risk factors associated with it is important for a successful rehabilitation. Decreased proprioception and weakness are the main drawbacks associated with postoperative blocks as early mobilization cannot be started and there is an increased risk of postoperative fall due to lack of proprioception at the knee joint.
Within our limited study group, the following advantages of intravenous tramadol over epidural tramadol were noted:
Ease of administration
No need for postdrug administration monitoring of vitals
Good analgesia
No major risk factors
Good patient compliance for intravenous line.
Complications/drawbacks associated with epidural tramadol based on available literature:
Bowel and bladder dysfunction
Infection
Misplacement of the catheter
Respiratory depression
Postdural puncture headache
Epidural hematoma
Epidural abscess
Catheter can get kinked
Breakage and migration can also occur.
However, it is worth noting that within our study group managed with epidural tramadol, respiratory depression was not noted. The drop in blood pressure in one patient may be caused due to a reduction in vascular tone following adequate analgesia. The burning sensation in bilateral lower limbs noted could not be explained, however, it has been documented in a study conducted by Chrubasik et al.[26] on epidural tramadol in postoperative case of abdominal surgery.
A newer concept in pain management in total knee replacement is multimodal pain management. This concept was introduced in an attempt to the control pain with less reliance on opioids. A multidisciplinary approach to pain management with a goal to maximize the analgesic effect and minimize the side effects of the medications is the goal of multimodality management.
Conclusion
Based on the advantages noted within out limited study group, among the patients managed with intravenous tramadol and the literature available on the complications that may occur due to an epidural catheter, we determined that intravenous tramadol can provide an effective postoperative analgesia and has the added advantage of no need for monitoring after drug administration.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Pain intensity on the first day after surgery: A prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118:934-44.
- [CrossRef] [PubMed] [Google Scholar]
- Perioperative pain management in hip and knee replacement surgery. Am J Orthop (Belle Mead NJ). 2014;43:S1-16.
- [Google Scholar]
- Postoperative analgesia after total knee arthroplasty. Rev Bras Anestesiol. 2016;66:437-8.
- [CrossRef] [PubMed] [Google Scholar]
- Impact on postoperative pain of long-lasting pre-emptive epidural analgesia before total hip replacement: A prospective, randomised, double-blind study. Anaesthesia. 2005;60:118-23.
- [CrossRef] [PubMed] [Google Scholar]
- The efficacy of preemptive analgesia for acute postoperative pain management: A meta-analysis. Anesth Analg. 2005;100:757-73.
- [CrossRef] [PubMed] [Google Scholar]
- The John Insall award: No benefit of minimally invasive TKA on gait and strength outcomes: A randomized controlled trial. Clin Orthopaedics Related Res. 2013;471:46-55.
- [CrossRef] [PubMed] [Google Scholar]
- The analgesic efficacy of celecoxib, pregabalin, and their combination for spinal fusion surgery. Anesth Analg. 2006;103:1271-7.
- [CrossRef] [PubMed] [Google Scholar]
- Guidelines for the management of postoperative pain after total knee arthroplasty. Knee Surg Related Res. 2012;24:201.
- [CrossRef] [PubMed] [Google Scholar]
- Pain management for joint arthroplasty: Preemptive analgesia. J Arthroplasty. 2002;17:129-33.
- [CrossRef] [PubMed] [Google Scholar]
- Epidural analgesia compared with peripheral nerve blockade after major knee surgery. Crit Care. 2009;13:1.
- [CrossRef] [Google Scholar]
- The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg. 1993;77:1048-56.
- [CrossRef] [PubMed] [Google Scholar]
- A pre-emptive multimodal pathway featuring peripheral nerve block improves perioperative outcomes after major orthopedic surgery. Reg Anesth Pain Med. 2008;33:510-7.
- [CrossRef] [Google Scholar]
- A comprehensive anesthesia protocol that emphasizes peripheral nerve blockade for total knee and total hip arthroplasty. J Bone Joint Surg Am (87 Suppl 2):63-70.
- [CrossRef] [Google Scholar]
- Practice guidelines for acute pain management in the perioperative setting: An updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116:248-73.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of continuous epidural infusion of ropivacaine and sufentanil with intravenous patient-controlled analgesia after total hip replacement. Anaesthesia. 2001;56:1181-201.
- [CrossRef] [PubMed] [Google Scholar]
- Epidural analgesia for pain relief following hip or knee replacement. Cochrane Database Syst Rev (3):CD003071. doi: 10.1002/14651858.CD003071
- [CrossRef] [PubMed] [Google Scholar]
- Advantage of ropivacaine for postoperative epidural analgesia following leg orthopedic surgery. Masui. 2005;54:8-13.
- [Google Scholar]
- An economic evaluation of bupivacaine plus fentanyl versus ropivacaine alone for patient-controlled epidural analgesia after total-knee replacement procedure: A double-blinded randomized study. Reg Anesth Pain Med. 2005;30:446-51.
- [CrossRef] [Google Scholar]
- Epidural analgesia compared with peripheral nerve blockade after major knee surgery: A systematic review and meta-analysis of randomized trials. Br J Anaesth. 2008;100:154-64.
- [CrossRef] [PubMed] [Google Scholar]
- Postoperative pain and patient-controlled epidural analgesia-related adverse effects in young and elderly patients: A retrospective analysis of 2,435 patients. J Pain Res. 2017;10:897-904.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness and safety of continuous ultrasound-guided femoral nerve block versus epidural analgesia after total knee arthroplasty. Rev Esp Anestesiol Reanim. 2017;64:79-85.
- [CrossRef] [Google Scholar]
- Epidural versus intra-articular infusion analgesia following total knee replacement. J Orthop Surg (Hong Kong). 2015;23:287-9.
- [CrossRef] [PubMed] [Google Scholar]
- Local infiltration anesthesia versus epidural analgesia for postoperative pain control in total knee arthroplasty: A systematic review and meta-analysis. J Orthop Surg Res. 2018;13:112.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of postoperative epidural analgesia: A meta-analysis. JAMA. 2003;290:2455-63.
- [CrossRef] [PubMed] [Google Scholar]
- Novel management of postoperative pain using only oral analgesics after LADG. Surg Today. 2016;46:117-22.
- [CrossRef] [PubMed] [Google Scholar]
- Analgesic potency of epidural tramadol after abdominal surgery. Pain. 1987;30:S154.
- [CrossRef] [Google Scholar]




