
Translate this page into:
Superior iliac hip dislocation: A rare injury and literature review
Address for correspondence: Dr. Ganesh Singh Dharmshaktu, Department of Orthopaedics, Government Medical College, Haldwani - 263 139, Uttarakhand, India. E-mail: drganeshortho@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Dharmshaktu GS, Adhikari N, Mourya P. Superior iliac hip dislocation: A rare injury and literature review. J Orthop Spine 2020;8:123-5.
Abstract
The anterior hip dislocations are uncommon and are further categorized into pubic or iliac type. Iliac type of dislocation is less common than pubic type. These injuries are limited to a few case reports or small series in the literature. There is no consensus on the mechanism of injury and treatment strategy for this injury. We present a case of isolated left side superior iliac type of hip dislocation in a 30-year-old male patient. The case was managed by uneventful concentric reduction under anesthesia. There was no recurrence and radiological features of osteonecrosis was not noted in the follow-up of 8 months.
Keywords
Closed reduction
dislocation
hip
iliac dislocation
superior hip dislocation

Introduction
The hip dislocation is an uncommon injury with a reported incidence of 5% of all dislocations.[1] The most common, posterior dislocation usually results from axial force toward flexed hip joint through the lower limb and knee in a typical dashboard injury pattern. The similar injury in extended hip and abduction results in anterior dislocation.[2] The anterior dislocation is classified in superior-anterior (pubic) or inferior-anterior (obturator). Pubic type results from abduction, extension, and external rotation, whereas obturator type result from abduction, flexion, and external rotation.[3] The reported incidence of anterior dislocation is 2%–17% of all hip dislocations.[4]
Superior dislocations variant of anterior dislocations are much less common than inferior ones.[5] These injuries usually present with hip extended and external rotation; however, these positions may alter in the presence of other associated injuries or fractures. Femoral neurovascular structures may be injured. Various reduction maneuvers are described such as Allis's maneuver, “Captain Morgan” maneuver, reverse Bigelow, and Stimson maneuver for successful closed reduction, whereas the open methods are reserved for very few difficult cases.[6] Careful observation of clinical and radiological presentation is important to appropriately diagnose or manage these rare injuries.
Case Report
A 30-year-old male patient presented with a history of fall from the height of about 10 feet into a gorge 1 hour back following a road traffic accident and could not bear weight on the left lower extremity. He was carried to a nearby hospital for first aid before referral. He had a history of no other associated injury and all he could recall was an entanglement of his left leg between seats of his car and had no exact recall of position of the limb. There were pain and limitation of movement at the hip region and the patient demanded urgent radiograph and treatment. Distal neurovascular status was found intact and the patient was rushed for radiography. The radiographs of the patient revealed no fracture in the upper femur and acetabulum region. The head of the femur was present outside the acetabulum and adjacent to the iliac bone just below the anterior superior iliac spine (ASIS) level [Figure 1]. It could also be palpated as hard globular mass beneath the ASIS and anteriorly. The diagnosis of superior hip dislocation of the iliac variant was established and the case was planned for a reduction under anesthesia following informed consent of the technique, future prognosis, and publication of data. The advice of computerized tomography (CT) scan and magnetic resonance imaging (MRI) was refused by the patient due to financial constraints. The affected limb was shortened and slight external rotation of the limb was noted during quick preprocedure evaluation [Figure 2, first image]. Under sedation, the limb was slightly flexed at hip almost 30° and longitudinal traction was applied, resulting in snapping sound of clinical reduction. The length of the the affected extremity and rotation was also regained [Figure 2, second image]. The postreduction radiographs confirmed concentric reduction [Figure 3a] and the lower limb was given rest and precautionary skin traction with only 50 g weight was provided. The postprocedure period was uneventful, and the patient was discharged after explaining instruction of bed rest for 3 weeks and quadriceps and gluteal muscle strengthening exercises. Gentle physiotherapy and nonweight bearing ambulation under supervision were started after 3 weeks for 4 more weeks. The patient then began initially toe-touch and then full weight-bearing ambulation while the pain and discomfort were recovered. There was no clinical and radiological recurrence noted in the follow-up [Figure 3b]. The radiological signs of osteonecrosis were also not noted in the follow-up of 8 months with the Harris Hip Score 85 out of 100 signifying a good result. The patient had painless ambulation and performed activities of daily living without discomfort or disability.

- The radiograph showing superior dislocation of the left femoral head out of the acetabulum. The femoral head is seen resting adjacent to the ipsilateral iliac bone. There is no associated bony injury

- The clinical image before reduction (first image) showing left lower limb shortening with mild external rotation of the limb suggestive of proximal migration of femur. Regain of length is noted after clinical reduction (second image)
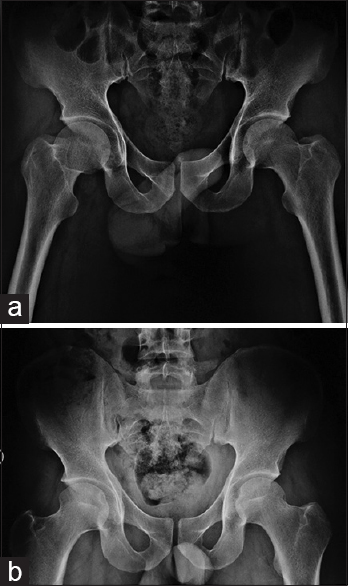
- The postreduction radiograph (a) showing a well reduced, concentric hip joint. Radiograph in the follow-up showing stable joint with no recurrence or signs of osteonecrosis (b)
Discussion
These injuries have limited reports and there are chances of these injuries to be misdiagnosed as more common posterior dislocation. One easy trick to distinguish between the two may require a careful appreciation of the lesser trochanter. The lesser trochanter when obscured and less prominent due to internal rotation of the hip is usually fund in posterior dislocation while in the anterior dislocation as the limb is externally rotated the whole profile of lesser trochanter is seen.[7] The clinical picture of our patient was of shortening without internal rotation, thus ruling out posterior dislocation and lack of external rotation also favored the diagnosis of pure, superior dislocation. There were, fortunately, no associated adjacent or remote injuries. Usually, the closed reduction under anesthesia reduces the joint, but failed reduction may require open reduction as done in two out of three reported cases by Admani et al.[8] The above author used Allis maneuver in all cases, including one successful attempt, but we used slight flexion as under anesthesia milder forces were aimed at the already traumatized hip with probable notorious vascular insult. The anterior approach was used by authors in the supine position in two cases. The concomitant fractures like that of the acetabulum may be present and require management of that fracture following the reduction. A report of anterior column acetabular fracture was managed by surgical internal fixation.[9] Another recent report of three cases of the superolateral (iliac) type of hip dislocation with associated acetabular fractures were reported by Vijayan et al.[10] Posterior acetabular rim and wall fracture are also reported in one report, thus highlighting the exclusion of associated injuries.[11] The shortcoming of our report was that no CT was done as the advice was refused by the patient, so we may have missed small avulsions or labral damages. One rare incidence of bilateral iliac hip dislocation has been reported by Sen et al. and has one side femoral head fracture.[12]
The role of traction after simple hip dislocations have not been found overtly beneficial and earlier mobilization is equally good. The skin traction given by us just ensured enforced bed rest for an initial hospital stay, which was discontinued after 5 days followed by nonweight bearing for the next 10 days.[13] The hip dislocations can be classified as simple dislocation and complex dislocations (fracturedislocations). The pathoanatomy of the hip joint dislocations has been better understood by newer technologies such as multi-detector CT, hip arthroscopy, and high field MRI.[14] Associated injury to structures such as ligamentum teres, joint capsule, and iliofemoral ligament has been observed with superior dislocation. These injuries may have future complications such as instability and arthritis.[15,16] Avulsion injury of anterior inferior iliac spine and impaction injuries of the head of the femur may also occur and may only be appreciated in advance imaging.[17,18] The dislocations should thus undergo CT or MRI evaluation to better document and manage additional injuries. Osteonecrosis and secondary arthritis are major complications of hip dislocation and require long monitoring and our case had no history of radiological features of it before he lost to follow-up after 8 months. These rare injuries require a large series of cases or multicentric collaboration to gather large case pool for better insights into mechanism and treatment consensus.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Understanding a rare injury: An observational study of anterior-superior hip dislocations. AJR Am J Roentgenol. 2020;214:624-9.
- [CrossRef] [PubMed] [Google Scholar]
- Dislocation of the hip: A review of types, causes, and treatment. Ochsner J. 2018;18:242-52.
- [CrossRef] [PubMed] [Google Scholar]
- Obturator dislocation of the hip. J Bone Joint Surg Br. 2001;83:113-5.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior hip dislocation: Atypical superolateral displacement of the femoral head. AJR Am J Roentgenol. 1983;141:385-6.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior Hip (femur) Dislocation. In: In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
- [Google Scholar]
- Traumatic hip dislocation: What the orthopedic surgeon wants to know. Radiographics. 2017;37:2181-201.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior superior dislocation of the hip joint: A report of 3 cases and review of the literature. East Afr Orthop J.. 2014;8:71-5.
- [Google Scholar]
- Superior dislocation hip with anterior column acetabular fracture Open reduction and internal fixation using a twin incision technique. Pan Afr Med J. 2012;12:41.
- [Google Scholar]
- Superolateral anterior hip dislocation with acetabular fracture: Report of three cases and review of literature. J Kar Orth Assoc. 2019;7:39-43.
- [Google Scholar]
- Traumatic anterior dislocation of the hip jpin t with posterior acetabular wall fracture. Acta Orthop Belg. 2005;71:111-4.
- [Google Scholar]
- Bilateral simultaneous iliac dislocation of the hip. Hip Int. 2004;14:196-8.
- [CrossRef] [PubMed] [Google Scholar]
- Hip dislocation without fracture: Traction or mobilization after reduction? Injury. 1993;24:27-31.
- [CrossRef] [PubMed] [Google Scholar]
- Hip dislocations-epidemiology, treatment, and outcomes. Injury. 2010;41:329-34.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging evaluation of the hip after arthroscopic surgery for femoroacetabular impingement. Skeletal Radiol. 2017;46:1315-26.
- [CrossRef] [PubMed] [Google Scholar]
- Should the capsule be repaired or plicated after hip arthroscopy for labral tears associated with femoroacetabular impingement or instability? A systematic review. Arthroscopy. 2018;34:303-18.
- [CrossRef] [PubMed] [Google Scholar]
- Traumatic anterior dislocation of the hip: Spectrum of plain film and CT findings. AJR Am J Roentgenol. 1995;165:1215-9.
- [CrossRef] [PubMed] [Google Scholar]
- Traumatic anterior hip dislocation associated with anterior and inferior iliac spines avulsions and a capsular-labral lesion. Strategies Trauma Limb Reconstr. 2008;3:39-43.
- [CrossRef] [PubMed] [Google Scholar]




