
Translate this page into:
“A Journey from Doom to Bloom” – A Rare Case of Low-Energy Pediatric Open Supracondylar Fracture of Humerus with Brachial Artery Laceration Managed with “Orthoplastic Approach”
Address for correspondence: Dr. Sharat Agarwal, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India. E-mail: drsharat88@yahoo.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Agarwal S, Sarkar S, Agarwal M. “A journey from doom to bloom” - A rare case of low-energy pediatric open supracondylar fracture of humerus with brachial artery laceration managed with “Orthoplastic Approach”. J Orthop Spine 2020;8:113-7.
Abstract
Supracondylar fracture of the humerus (SFH) is the most common fracture of the elbow in the pediatric population (60%). The brachial artery is the most frequently injured artery in the upper extremity due to its vulnerability, and commonly, it is associated with road traffic accidents (RTAs) and occupational injuries. However, brachial artery injury in the pediatric age group is not very frequent as in adults and commonly associated with SFH. Long-term sequelae of ischemia in the forearm such as Volkmann's ischemic contracture may prove disastrous. Early aggressive management in terms of exploration of the brachial artery is recommended by Blakey et al., to prevent such serious complications. Arterial injury ranges anywhere from vascular contusion and intimal damage, to complete arterial transaction. Low-velocity injuries such as falls or sports injuries can cause isolated Type 1 open fractures (Gustilo and Anderson classification of open fractures). Open supracondylar fracture complicated by brachial artery laceration is usually seen in high-velocity injuries such as RTA and is usually a part of multiple injuries sustained in such patients. However, in search of literature, we have not found an isolated Type 3 open supracondylar fracture with brachial artery laceration following a fall from a speeding bicycle, which is considered as a low-energy trauma. This patient was managed with reduction and fixation of the fracture with crossed K-wires and repair of the brachial artery with interpositional reversed saphenous vein graft to save the limb.
Keywords
Brachial artery laceration
low-velocity open fracture
open supracondylar fracture
orthoplastic approach
pediatric fractures

Introduction
Supracondylar fractures of the humerus (SFH) are a common pediatric elbow injury, accounting for 16% of all pediatric fractures with a peak incidence at the ages of 5–8 years.[1,2,3] In the Indian setting, Tandon et al. have reported an incidence of 2.8% of open injuries in 500 pediatric fractures.[4] The main artery involved in SFH is the brachial artery, and the pattern of injury to the artery varies from simple contusion to laceration, thrombosis, perforation, and even transaction with the ends exposed or entrapped in the fractured segments.[5] Most cases of pediatric open fractures are a result of high-velocity trauma including motor vehicle accidents and fall from heights. Low-velocity injuries such as falls or sports injuries also lead to open fractures, usually Type I injuries.[6] However, here, we report a rare case of open SFH with brachial artery laceration due to an injury following a fall from speeding bicycle, which was successfully managed with brachial artery repair using reversed interpositional saphenous vein graft, wound management, and simultaneous fracture fixation, eventually resulting in limb survival with good functional outcome exemplifying the concept of “Orthoplastic Approach.”
Case Report
A 10-year-old boy was brought to the emergency department of our hospital with swelling, bleeding lacerated wound, severe pain, and deformity at the right elbow region following fall from a bicycle about 6 h before admission. There was associated pain, swelling, and deformity in the distal forearm also. On examination, there was a 5 cm × 6 cm lacerated wound present on the front of elbow, and the distal arm with a large segment of fractured bone (distal humerus) was jutting out of the wound indicating contamination of the fractured site [Figure 1]. Distal radial and ulnar artery pulsations were absent. Due to the cold and pale nature of the hand and apparently evident torn vessel at the elbow, it has prompted us to consider laceration of the brachial artery. There was an associated restriction of hand-and-finger movements; however, the sensations in the distal forearm and hand were intact. Radiographs taken in the emergency room showed Gartland Type III SHF [Figure 2] with displaced fracture of the distal one-third shaft of radius and ulna. Considering the high possibility of brachial artery laceration with an urgent indication for the vascular repair, a decision to do emergency angiography was taken. Simultaneously, preparations were made for undertaking urgent microvascular surgical intervention with the help of a vascular surgeon to prevent limb loss and debilitating long-term sequelae. Angiography confirmed the brachial artery laceration [Figures 3 and 4], and accordingly, the injury was classified as Grade 3C (Gustilo–Anderson classification of open fractures).

- Lacerated wound in front of elbow with exposed distal humerus and lacerated brachial artery (arrow)

- Radiograph showing displaced supracondylar fracture of humerus

- Angiogram showing interrupted circulation in the brachial artery

- Computed tomography angiogram with interrupted circulation in brachial artery
An emergency distal humeral and brachial artery exploration was done with simultaneous debridement using a lazy S-shaped incision incorporating wound. The soft tissues and bone ends were irrigated with low-pressure systems using normal saline to remove all foreign matters. The fracture was reduced and held with three 1.25 mm K-wires (two lateral and one medial), which crossed each other transfixing the fracture site, and it was decided to manage the distal forearm bone fracture conservatively [Figure 5].[7,8] Being an unstable bone fracture, we performed bone fixation before vascular repair. This ensured dependable biomechanical stability at the fracture site to provide protection to overlying vascular repair. During exploration, the median nerve was found intact but was mildly contused. The brachial artery was found to be completely transacted with the proximal end retracted deep under the muscle, while the distal end could be easily found. The proximal stump was lacerated and thrombosed with visible pulsation 2 cm above the stump. The two ends were resected, and a Fogarty embolectomy catheter was introduced through both ends to ensure the patency of the vessel. A segment (~5 cm) of the long saphenous vein from the right groin was harvested. An interpositional reversed vein graft was performed using 9-0 nylon sutures [Figure 6]. A proximal forearm fasciotomy was performed to prevent compartment syndrome due to reperfusion injury. Per-operatively, distal radial pulsations were restored back after the brachial artery reconstruction. The injured arm was maintained in a long-arm plaster splint in about 100° of flexion. Postoperatively, distal limb circulation was monitored by pink and warm hand and good finger movements on examination, digital oxygen saturation using SpO2, capillary refilling of <3 s, and radial pulsations indicating good circulation in the hand and forearm.[7] He was started on systemic anticoagulant therapy with intravenous infusion of heparin in the dosage of 3500 units/day (100 U/kg) for 2 weeks with constant monitoring of coagulation profile and international normalized ratio. He was advised antiplatelet therapy with tablet Aspirin 100 mg/d to be taken orally for 6 weeks at discharge from the hospital. The patient was given injection cefuroxime 1 g and injection gentamicin 60 mg twice a day to cover against both Gram-positive and Gram-negative organisms for 2 weeks. Injection metronidazole 500 mg thrice a day for 5 days intravenously was given for coverage against anaerobic organisms due to ischemic nature of injury. The patient showed good recovery of limb circulation and survival following intervention. Removal of K-wires was undertaken on an outpatient basis after 6 weeks. The patient was followed on a regular outpatient basis and given physiotherapy with elbow mobilization. There was complete recovery of elbow function with no residual upper limb deformity and good fracture union and remodeling of the fractures at the end of 3 months [Figures 7-10].

- Radiograph showing fracture fixation using crossed K-wires and fracture distal one-third both bone forearms managed conservatively
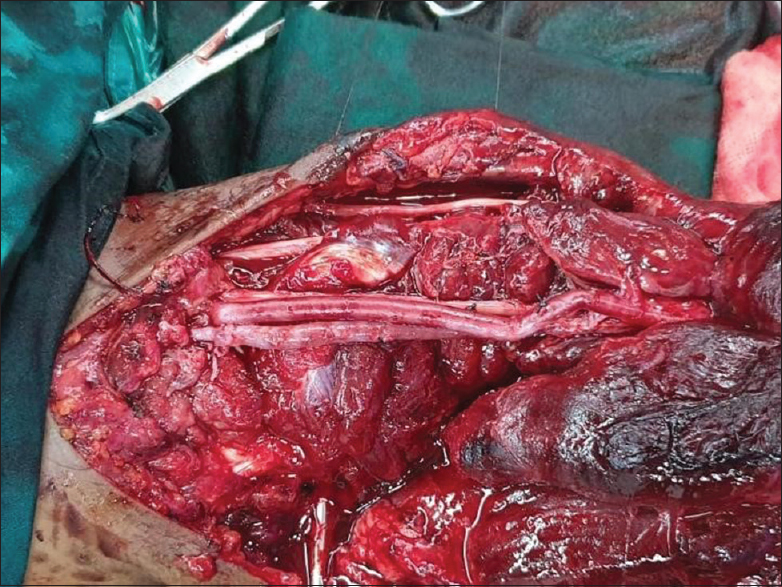
- Per-operative picture showing repaired brachial artery using reverse-interpositional saphenous vein graft (arrow)

- Clinical picture of the healed wound on anterior aspect of elbow region (arrow)
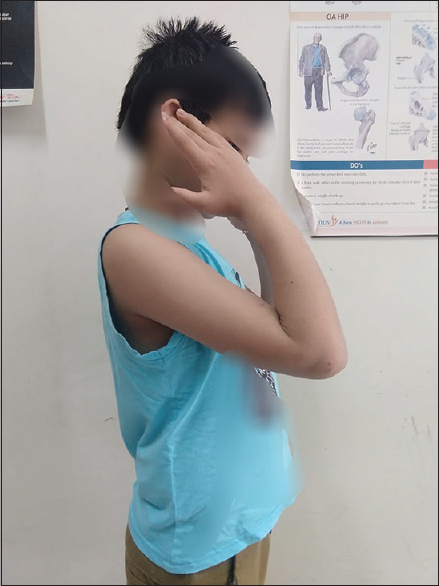
- Clinical picture showing full flexion after 3 months of injury
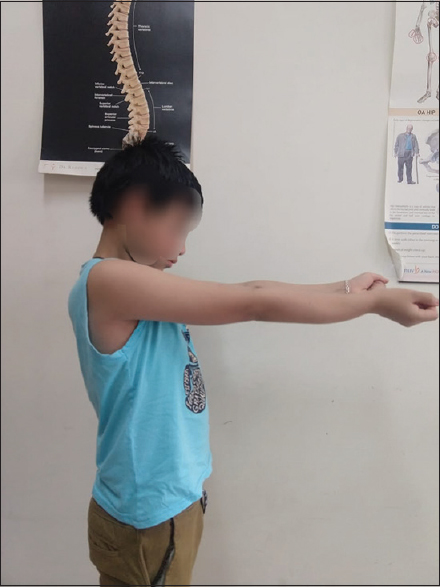
- Clinical picture with normal full extension with no upper limb deformity after 3 months of injury

- Radiograph of united supracondylar and distal one-third both bone fracture after 3 months of injury
Discussion
The concept of “Orthoplastic Approach” is an integrated approach to address both fracture fixation and soft-tissue management including vascular repairs.[6] Fixation in open fractures should be aimed at providing stable fixation of fractures and facilitating wound care, apart from decreasing pain; preventing further soft-tissue damage from fracture fragments; restoring length, alignment, and rotation; and supporting a robust host response against microbes despite the presence of metallic implants. In children, rigid fixation is not always mandatory as in the case of adults. The use of percutaneous Kirschner wires has been shown to provide adequate fixation in supracondylar fractures.[7,8,9] Brachial artery injury represents a relatively rare yet serious complication of pediatric supracondylar humeral fractures, and traumatic pediatric vascular injuries are very rare, with an incidence of vascular injury being higher in open injuries than closed injuries.[10] The most common situations of vascular lesions in childhood were penetrating injuries and fractures of the extremities, either as isolated injuries or in multiply injured patients.[11] Traditionally, brachial artery traumatic lesions have been managed surgically, with primary anastomosis, vein or prosthetic grafts, or simple ligation. Initial careful wound exploration and debridement with careful removal of any foreign bodies is imperative to check the possibility of infection in an ischemic limb at the time of primary surgery for a successful outcome. Complete functional recovery with restoration of limb circulation distal to the injury can be achieved by early exploration, bypass vein or interpositional grafting (Great saphenous vein has proven to be the most common and the best conduit for brachial arterial reconstruction with the added advantage of comparability of its caliber with that of brachial artery), and fasciotomy following fracture reduction and fixation.
Conclusion
The management of brachial artery injury requires an urgent repair or venous grafting based on the extent of the defect to salvage an ischemic limb. Repair of the artery within 6 h is the gold standard treatment to avoid ischemic damage to neural tissues and distal muscle mass and should be preceded with reduction and fixation of supracondylar fracture to protect the vascular repair. However, it is not unusual in our practice to have patients presenting beyond 6 h since injury, wherein still consideration for the arterial repair can be given, which may be done before fixing the fracture to avoid prolonging the ischemia time further. Furthermore, clinicians should remember that the delayed presentation risk survival of the limb due to the likelihood of compartment syndrome, myoglobinuria, acute renal failure, and the possibility of postrepair reperfusion injury.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Ischaemia and the pink, pulseless hand complicating supracondylar fractures of the humerus in childhood: Long-term follow-up. J Bone Joint Surg Br. 2009;91:1487-92.
- [CrossRef] [PubMed] [Google Scholar]
- The epidemiology of low- and high-energy distal radius fracture in middle-aged and elderly men and women in Southern Norway. PLoS One. 2012;7:e43367.
- [CrossRef] [PubMed] [Google Scholar]
- Limb fracture pattern in different paediatric age groups: A study of 3,350 children. J Orthop Trauma. 1993;7:15-22.
- [CrossRef] [PubMed] [Google Scholar]
- Paediatric trauma epidemiology in an urban scenario in India. J Orthop Surg (Hong Kong). 2007;15:41-5.
- [CrossRef] [PubMed] [Google Scholar]
- Open fractures in children. Principles of evaluation and management. J Bone Joint Surg Am. 2005;87:2784-98.
- [CrossRef] [Google Scholar]
- Treatment of pink pulseless hand following supracondylar fractures of the humerus in children. Int Orthop. 2009;33:237-41.
- [CrossRef] [PubMed] [Google Scholar]
- Management of supracondylar fractures of the humerus in children. EFORT Open Rev. 2018;3:526-40.
- [CrossRef] [PubMed] [Google Scholar]
- Multicentre collaborative cohort study of the use of Kirschner wires for the management of supracondylar fractures in children. Chin J Traumatol. 2019;22:249-54.
- [CrossRef] [PubMed] [Google Scholar]
- The ortho-plastic approach to soft tissue management in trauma. Open Orthop J. 2014;8:399-408.
- [CrossRef] [PubMed] [Google Scholar]
- Operative treatment of supracondylar fractures of the humerus in children. The consequences of pin placement. J Bone Joint Surg Am. 2001;83:735-40.
- [CrossRef] [PubMed] [Google Scholar]
- Rupture of the brachial artery accompanying dislocation of the elbow or supracondylar fracture. J Bone Joint Surg Am. 1951;33-A:889-94.
- [CrossRef] [Google Scholar]




