
Translate this page into:
Noncontiguous two levels traumatic dislocation of the cervical spine managed with a posterior only approach
Address for correspondence: Dr. Amit Agrawal, Department of Neurosurgery, Narayana Medical College and Hospital, Chinthareddypalem, Nellore - 524 003, Andhra Pradesh, India. E-mail: dramiitagrawal@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Agrawal A, Kumar VA, Kiran NA, Venkatesh M, Kumar VA. Noncontiguous two levels traumatic dislocation of the cervical spine managed with a posterior only approach. J Orthop Spine 2019;7:80-2.
Abstract
Literature defines multiple noncontiguous vertebral injuries, as “injuries to the vertebral column involving ≥1 site, and these injuries are separated by an apparently normal area of the spine.” In the present article, we report an unusual case of two nonadjacent levels traumatic dislocation, involving the cervical spine managed through the posterior-only approach.
Keywords
Cervical spine fractures
noncontiguous spine fracture
posterior approach
spinal injuries

Introduction
Literature defines multiple noncontiguous vertebral injuries, as “injuries to the vertebral column involving ≥1 site, and these injuries are separated by an apparently normal area of the spine.”[1] Usually, these injuries involve different spinal region, that is, thoracic/thoracolumbar or cervical in combination [1-4] or thoracic + thoracic region;[5] however, the occurrence of multiple noncontiguous vertebral injuries in the same region, in the cervical region, is not reported. In the present article, we report an unusual case of two nonadjacent levels traumatic dislocation, involving the cervical spine managed through posterior only approach.
Case Report
A 65-year-old male patient was brought to the emergency room 12 h after the injury. He presented with the history of slip and fall while climbing down from a tree. He noticed weakness of all the four limbs and had urinary retention, for which an indwelling urinary catheter was placed. On examination, pulse rate was 46/min, blood pressure was 110/70 mm/hg, and respiratory rate was 18/min (predominantly abdominal breathing, with a single-breath counting of eight). The patient was conscious, alert, and oriented to time place and person (GCS: E4V5M6). Pupils were bilaterally equal and reacting to light. Motor examination showed normal bulk and hypotonia in all the limbs; the power was Grade 0 with absent deep tendon superficial reflexes. He had loss of sensation below T1 dermatome. He had priapism on examination. All the laboratory investigations including coagulation profile were normal. X-ray cervical spine was suggestive of C4/C5 and C6/C7 Grade III subluxation. Magnetic resonance imaging and computed tomography of the cervical spine showed anterior subluxation of C4 vertebra over C5 and bilateral locked facets of C4/C5 vertebra, anterior subluxation of C6 vertebra over C7, and bilateral locked facets of C6/C7 vertebra. Displaced fractures of left pedicles and superior facets of C5 and C7 vertebra and diffuse disc edema and pseudodisc bulges of C4/C5 and C6/C7 discs were seen compressing the thecal sac and compression of spinal cord. Long-segment diffuse hyperintense signals were seen spinal cord from C2/C3 disc space to C6/C7 disc space is seen in T2W images suggestive of cord edema [Figure 1]. Ultrasonography of the abdomen did not show any abnormality. The patient was treated with Gardner–Wells Skull Tongs traction preoperatively, and the weight was increased up to 8 kg. However, there was no reduction of the subluxation. In view of the unstable general condition and highly unstable spine, the patient was planned for a posterior approach first. Accordingly, the patient was taken for surgery. The patient was placed in prone position, and intraoperatively, traction was continued. The segments were still in nonreduced position [Figure 2a]. Cervical and dorsal spinous processes from C1 to T1 were exposed through a midline incision. Lamina and lateral masses were exposed from C3 to C7 levels, and screw entry points were identified. Lateral mass screws were placed from C3 to C7 levels bilaterally under radiographic guidance [Figure 2b]. Laminae were fractured and moving freely and to avoid inward impingement of the broken fragments and provide space for edematous cord to expand laminectomy was performed. Titanium rods were placed in screw heads, and nuts were tightened in sequential manner (to achieve Zip effect) which resulted in good reduced position of the subluxated vertebral bodies [Figure 2c and d]. Bone chips obtained from laminectomy were used to achieve fusion. The patient was kept on elective ventilation and could be gradually weaned off. The patient was stable at 6-month follow-up; however, there was no improvement in his neurological status.

- Sagittal T1 (a) and T2 (b) of the cervical spine showing multilevel anterior subluxations at C4 over C5 and C6 over C7 vertebrae with lax anterior and posterior longitudinal ligaments, severe cervical cord compression noted at C4–5 level and cord edema from C3–C7 levels. Sagittal computed tomography reformatted images (c and d) show locked facet joints at C4–5 and C6–7 levels
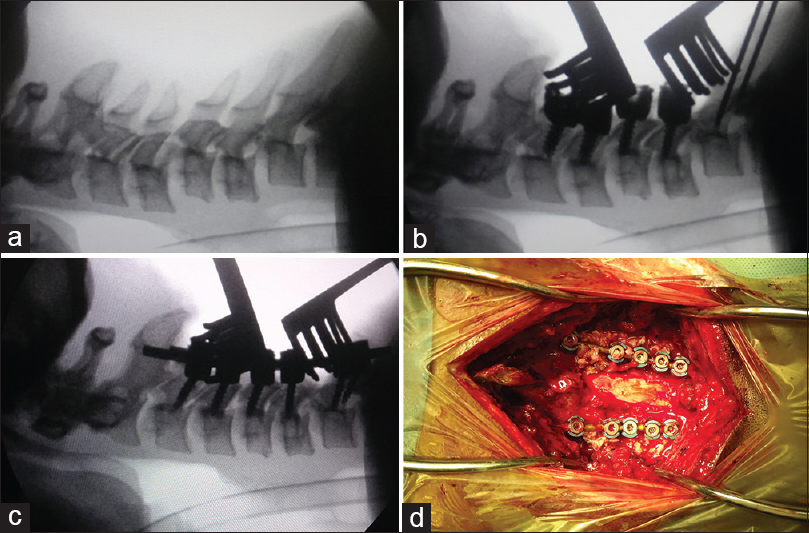
- (a) Intraoperative radiographic image showing C4 and C6–7 subluxation, (b) placement of lateral mass screws, (c) good alignment of vertebras after tightening the screws, and (d) intraoperative image showing the position of the screw heads
Discussion
The reported incidence of spinal injuries involving the cervical region is up to 3%, and up to 6.7% of the patients can have dislocation of the facets joints (usually C5–C6 and C6–C7 levels).[6] Involvement of the multiple spinal regions is reported in as many as 4.8% of patients with spinal injuries;[7] however, cervical dislocation involving two levels is uncommon with only two reported cases of adjacent levels of dislocation.[8,9] Usually, these uncommon injuries are caused by fall from high heights (in presented case tree),[5] the abnormal axial loading, flexion, and rotation can lead forces that cause compression, shear, and rotation forces at multiple levels.[8,9]
Surgical management of these unstable cases is not only controversial but also is a challenge for the treating personnel.[10] Initial traction can help to reduce the dislocation in selected cases; however, if this not reduce the dislocation neurosurgical intervention (i.e., anterior or posterior or a combined approach) to achieve open reduction is suggested.[8,11] Of the two reported cases of adjacent level dislocation involving cervical region, one case was managed by anterior only approach,[9] and the other case was managed through posterior only approach.[8] In the reported cases, the authors approached from posteriorly (one level above and one level below) and could achieve good reduction and stability using wire and iliac crest graft.[9] It can be argued that posterior approach alone may not provide anterior support; hence, anterior approach may also be needed to achieve stability.[8,12,13] However, with the advancements in surgical techniques, the posterior approach can provide adequate reduction under direct vision and stable fixation with lateral mass screws and rods.[14]
Conclusion
It has been reported that spinal injuries involving multiple-level noncontiguous level have an increased risk of deformity [9] and have poorer neurological outcome.[15] Posterior only approach can be used in unstable patients who sustain nonadjacent levels traumatic dislocation of the cervical spine.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Multiple non-contiguous injuries to the spine. Acta Orthop Scand. 1976;47:52-8.
- [CrossRef] [PubMed] [Google Scholar]
- Changing patterns of fracture in the dorsal and lumbar spine. Br Med J. 1966;1:891-4.
- [CrossRef] [PubMed] [Google Scholar]
- Stability of the thoracic and lumbar spine in traumatic paraplegia following fracture or fracture-dislocation. J Bone Joint Surg Am. 1970;52:1115-30.
- [CrossRef] [Google Scholar]
- Epidemiology of extraspinal fractures associated with acute spinal cord injury. Spinal Cord. 2001;39:589-94.
- [CrossRef] [PubMed] [Google Scholar]
- Delayed surgical management of a traumatic bilateral cervical facet dislocation by an anterior-posterior-anterior approach. J Clin Neurosci. 2007;14:782-6.
- [CrossRef] [PubMed] [Google Scholar]
- Reduction technique for uni-and biarticular dislocations of the lower cervical spine. Spine (Phila Pa 1976). 1998;23:949-54.
- [CrossRef] [PubMed] [Google Scholar]
- Two adjacent levels dislocation of the cervical spine managed viaan anterior only approach. A case report. J Med Liban. 2016;64:181-5.
- [CrossRef] [PubMed] [Google Scholar]
- Complete dislocations at two adjacent levels of the cervical spine. A case report. Spine (Phila Pa 1976). 1984;9:319-22.
- [CrossRef] [PubMed] [Google Scholar]
- Controversies in the treatment of cervical spine dislocations. Spine J. 2009;9:418-23.
- [CrossRef] [PubMed] [Google Scholar]
- A new anterior-posterior surgical approach for the treatment of cervical facet dislocations. J Spinal Disord Tech. 2014;27:E104-9.
- [CrossRef] [PubMed] [Google Scholar]
- The management of traumatic cervical bilateral facet fracture-dislocations with unicortical anterior plates. J Spinal Disord. 2000;13:374-81.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior reduction for cervical spine dislocation. Spine (Phila Pa 1976). 2006;31:648-52.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior stabilization of cervical spine injuries using the roy-camille plates: A long-term follow-up. Eur J Orthop Surg Traumatol (24 Suppl 1):S125-30.
- [CrossRef] [PubMed] [Google Scholar]
- Multilevel spinal injuries. Incidence, distribution and neurological patterns. J Bone Joint Surg Br. 1989;71:692-5.
- [CrossRef] [PubMed] [Google Scholar]




