
Translate this page into:
Medial collateral ligament-ganglion cyst: A rare case report and review of its literature
Address for correspondence: Dr. Suneet Rajshekhar, Sunshine Hospital, Bhubaneswar, Odisha, India. E-mail: suneet.rajshekhar@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Rajshekhar S, Patnaik S. Medial collateral ligament-ganglion cyst: A rare case report and review of its literature. J Orthop Allied Sci 2018;6:89-92.
Abstract
Ganglion cysts are found in locations which are under constant stress. Although somewhat controversial, one common explanation for the formation of ganglion cysts is that they are the result of mucoid cystic degeneration in collagenous structures. Most commonly, they are found along the tendons or joints of wrist or hand. The common locations of ganglion cysts are the wrist, knee, and anterolateral aspect of the ankle. Intra-articular ganglion cysts of the knee are rare, and most originate from the cruciate ligaments. The symptoms and signs of intra-articular ganglion cysts of the knee are pain, effusion, limitation of motion, and a clicking sensation. Increased size may lead to increased symptoms. Their location can sometimes interfere with joint movement. We present a case of ganglion cyst arising over medial collateral ligament which was presented as a swelling and investigated using sonography, magnetic resonance imaging and arthroscopy, surgically resected and confirmed on histopathology. Thus awareness of the symptoms and locations is necessary.
Keywords
Arthroscopy
ganglion cyst
knee joint
medial collateral ligament

Introduction
A 58-year-old male presented with a painful swelling on the medial aspect of the right knee. The swelling was slowly progressive in nature for the last 5 years. On examination, a palpable soft mass measuring about 7.5 cm × 4.0 cm was found to be sitting over the medial joint line. Plain roentgenography showed bulging soft tissue over the medial aspect of the right knee with cortical erosion of medial aspect of the proximal tibia and distal femur. Sonography revealed a hypoechoic soft-tissue cystic swelling 47 mm × 37 mm size over the medial aspect of right knee showing thick wall and particulate contents. Coronal and axial T2-weighted magnetic resonance images revealed a large tibial collateral ligament bursa communicating to the joint surface. We performed a diagnostic arthroscopy before surgical excision of the mass to rule out a parameniscal cyst, and a degenerative meniscal tear was found. Histopathologic examination of the excised mass was found to be a ganglion cyst. On 18 months follow-up, patient has no recurrence of swelling and having only mild osteoartritic symptoms.
The first case of a ganglion cyst of either the anterior cruciate ligament (ACL) or posterior cruciate ligament (PCL) was reported by Caan, who found an asymptomatic ganglion of the ACL in an elderly man at autopsy in 1924.[1] Kang et al. reported eight cases of ganglion cysts without specific symptoms, including two cysts found in the infrapatellar fat pad.[2] Lin et al. reported a case intra-articular ganglion cyst with medial femoral condylar erosion that originated between the medial collateral ligament (MCL) and medial parameniscal area.[3] We report a case of symptomatic extra-articular ganglion cyst with medial femoral and tibial condylar erosion with degenerated posterior third medial meniscus tear that originated between the superficial MCL, patella tendon and the Pes anserinues bursa. As far as literature is concerned, this is a rare location for a ganglion cyst.
Case Report
A 58-year-old male patient presented with a painful swelling over the medial joint line of the right knee, slowly progressive in nature for approximately 5 years. He has a history of repeated aspiration of swelling followed by disappearance of swelling for few weeks. A swelling was easily noted on inspection and palpation over the affected knee. There was no history of major trauma or old fracture of that limb. On physical examination, a remarkably well-demarcated, soft mass was found on the medial joint line of the right knee. It measured about 5.5 cm × 4.0 cm × 2.0 cm [Figure 1]. Tenderness was noted on palpation. The overlying skin over the mass was shiny, no joint effusion was noted, and there was no locking sensation during motion. Pain was aggravated on knee movement and relieved on rest. The patient had full range of motion in the affected knee. The results of Lachman's test, anterior drawer test, posterior drawer test, and McMurray test were negative, but tenderness was there in the posterior third of the medial joint line. Plain roentgenography showed a bulging soft-tissue mass over the medial aspect of the right knee associated with adjacent bone erosion. Sonography revealed a hypo-echoic soft-tissue cystic swelling 47 mm × 37 mm size over the anterolateral aspect of the right knee showing thick wall and particulate contents. Coronal and axial T2-weighted magnetic resonance images revealed a large tibial collateral ligament bursa, measuring 42 mm × 35 mm × 34 mm (CL × ML × AP) with communication to the joint surface [Figure 2]. Focal erosion of the adjacent femoral condyle was also noted. The tentative diagnosis was intra-articular ganglion cyst or parameniscal cyst. Arthroscopy of the right knee showed degenerated complex tear of the medial meniscus with erosion of the medial tibial condyle cartilage, outerbridge classification score 4 [Figure 3].

- Clinical picture
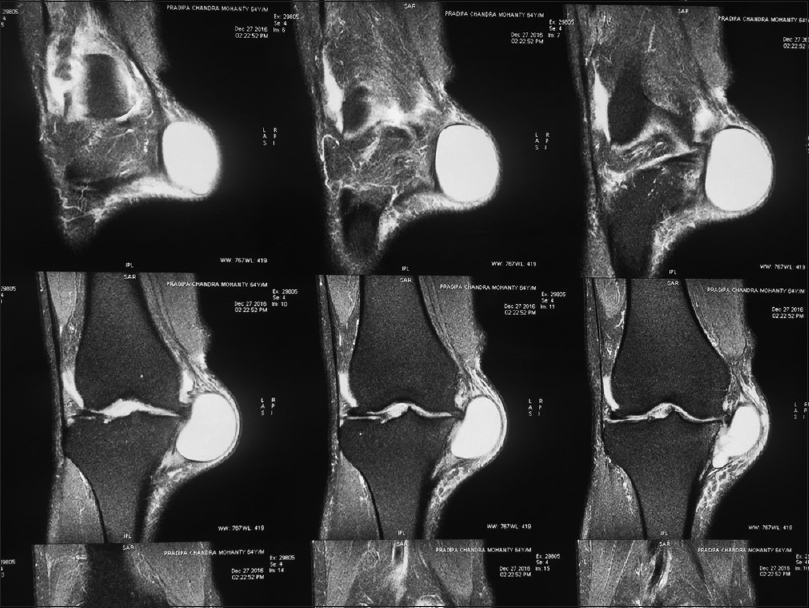
- Magnetic resonance imaging image
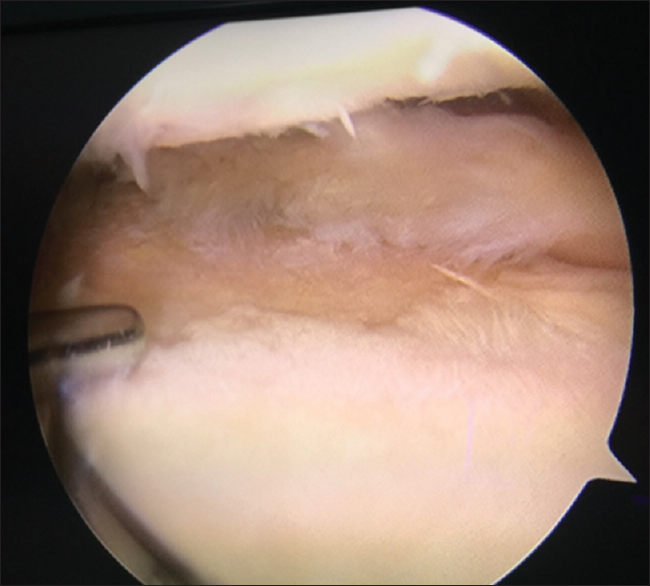
- Arthroscopic image
The lobulated, cystic mass was identified and dissected. Its stalk was found just adjacent to the insertion of the MCL [Figure 4]. The mass was excised completely and separated from the MCL, medial aspect of the patella tendon and the bursa surface of the Pes anserinues [Figure 5]. The specimen measured about 6.0 cm × 3.2 cm × 0.8 cm and had a multilobulated wall with lining cells and mucoid material in the cyst. Microscopic examination proved that the mass was an intra-articular ganglion cyst. There was no recurrence of swelling or major symptoms on 18-months follow-up.

- Intraoperative picture

- Resected cyst
Discussion
In general, most ganglion cysts are found in locations which are under constant stress. Although somewhat controversial, one common explanation for the formation of ganglion cysts is that they are the result of mucoid cystic degeneration in collagenous structures.[4] Most authors believe that they result from the degeneration of the menisci or from synovial tissue herniated through a defect in the joint capsule.[5] This degeneration produces a cyst with a well-defined fibrous capsule and highly viscous fluid internally, which will typically be demonstrated by intermediate or intermediate low T1 and high T2 signal.[6] Although trauma may play an important role in the formation of ganglion cysts,[4] Liu et al. reported that ganglion cysts of the ACL might be a congenital abnormality because of a negative trauma history and symptom relief after cyst removal.[7] Pressure from high-viscosity fluid in the ganglion cyst against the adjacent bone surface over a long period may produce an indentation through gradual erosion of the bone,[6] as stated by Lin et al. Such cysts are frequently interpreted as intraosseous ganglia. A ganglion cyst may originate from bone, tendon, bursae, parameniscal tissue, and intercompartment septi.[8] These lesions occur most frequently on the dorsum of the wrist, the palm, and the dorsolateral aspect of the foot. Ganglion cysts within knee joints are rare. The common locations of intra-articular ganglion cysts are the ACL and PCL and rarely, the infrapatellar fat pad. Ganglion cyst from the MCL is very rare, though stated earlier by Lin et al. as an intraarticular cyst.
The most common symptom of intra-articular ganglion cysts of the knee is pain. Other usual symptoms and signs include effusion, limitation of motion, and a clicking sensation.[9,10] Deutsch et al. hypothesized that the symptoms may be correlated with the variable size of the cyst.[4] In our case, symptoms of pain were mainly stretch pain of overlying skin and were aggravated by activity.
Differential diagnoses of a cyst-like lesion in the knee include synovial cyst, ganglion cyst, and parameniscal cyst. The diagnostic methods for ganglion cysts include plain roentgenography, soft-tissue sonography, computed tomography (CT), magnetic resonance imaging (MRI), and arthrography [Figure 4]. MRI has been advocated as the modality of choice in diagnosing cystic lesions of the knee.[11,12] Delayed roentgenography and CT after arthrography may sometimes help the diagnosis by showing articular communication of ganglion cysts of the knee which was not done in our case. The advantages of multiplanar capabilities and superior soft-tissue contrast make MRI better at identifying the anatomic and morphologic relationships of synovial tissue to surrounding structures, such as bone, vessels, and other soft-tissue structures. In this case, the differential diagnoses from MRI findings should include parameniscal cyst or intraarticular ganglion cyst. Before excision of the mass, arthroscopic evaluation was carried out to rule out the possibility of a medial meniscus tear [Figure 3]. Since there was remarkable degenerated tear in the medial meniscus, intraarticular ganglion cyst was the more likely diagnosis.
The treatment of ganglion cysts in the knee includes arthroscopic excision, aspiration, and open excision. Brown and Dandy found that 95% of patients had good or excellent results after arthroscopic excision.[13] No recurrence after arthroscopic excision was reported, although it seems that ganglion cysts may recur after excision. CT-guided aspiration is another choice. Nokes et al. aspirated two ganglion cysts of the PCL of the knee with an 18G needle and syringe holder, using CT guidance to avoid the popliteal vessels.[14] Both patients had relief from pain and had no recurrence of the cysts at 2 years. To reduce the possibility of recurrence, surgical excision is better than aspiration. We performed a parapatellar incision to excise the ganglion cyst because it was located out of reach of arthroscopy. There was no pain after surgical treatment and no recurrence at 1-year follow-up.
Conclusion
Ganglion cyst may develop over the collaterals of knee and may pose difficulty in diagnosis. Our report illustrates the importance of maintaining an index of suspension for the diagnosis ganglion cyst in case of soft-tissue swelling around the knee. A ganglion cyst should be kept in mind in differential diagnoses of soft-tissue swelling around the knee.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Cyst formation (ganglion) in the anterior cruciate ligament of the knee. Dtsch Z Chir. 1924;186:403-8.
- [Google Scholar]
- Intra-articular ganglion cysts of the knee. Arthroscopy. 1999;15:373-8.
- [CrossRef] [PubMed] [Google Scholar]
- Intra-articular ganglion cyst from medial collateral ligament of the knee joint: A case report and review of the literature. The Kaohsiung J Med Sci. 2004;20:357-61.
- [CrossRef] [Google Scholar]
- Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy. 1994;10:219-23.
- [CrossRef] [PubMed] [Google Scholar]
- The dorsal ganglion of the wrist: Its pathogenesis, gross and microscopic anatomy, and surgical treatment. J Hand Surg Am. 1976;1:228-35.
- [CrossRef] [PubMed] [Google Scholar]
- An unusual intra-articular ganglion of the knee with interosseous extension. A case report. J Bone Joint Surg Am. 1989;71:773-5.
- [CrossRef] [Google Scholar]
- Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy. 1994;10:110-2.
- [CrossRef] [PubMed] [Google Scholar]
- Intra-articular ganglion blocking extension of the knee: Brief report. J Bone Joint Surg Br. 1988;70:837..
- [CrossRef] [PubMed] [Google Scholar]
- The prevalence and significance of cyst-like changes at the cruciate ligament attachments in the knee. Skeletal Radiol. 1992;21:365-9.
- [CrossRef] [PubMed] [Google Scholar]
- Intraarticular ganglia of the knee: Prevalence, presentation, etiology, and management. AJR Am J Roentgenol. 1997;168:123-7.
- [CrossRef] [PubMed] [Google Scholar]
- Meniscal and ganglion cysts of the knee: MR evaluation. AJR Am J Roentgenol. 1988;150:331-6.
- [CrossRef] [PubMed] [Google Scholar]
- Intra-articular ganglia in the knee. Arthroscopy. 1990;6:322-3.
- [CrossRef] [PubMed] [Google Scholar]
- Ganglion cysts of the cruciate ligaments of the knee: Recognition on MR images and CT-guided aspiration. AJR Am J Roentgenol. 1994;162:1503..
- [CrossRef] [PubMed] [Google Scholar]




