
Translate this page into:
Intraoperative gamma probe application in patients prediagnosed with osteoid osteoma
Address for correspondence: Dr. Canan Can, Gazi Yasargil Egitim Ve Arastirma Hastanesi Nükleer Tip, Diyarbakir, Turkey. E-mail: canancankarahan@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Can C, Kapukaya A, Kaya H, Altindag S, Komek H. Intraoperative gamma probe application in patients prediagnosed with osteoid osteoma. J Orthop Allied Sci 2018;6:79-85.
Abstract
INTRODUCTION:
Osteoid osteoma is a benign but painful bone tumor that is treated with the excision of the nidus. Due to difficulties in reaching the tumor, intraoperative localization may be needed for complete excision without unnecessary resection of the surrounding bone.
AIM:
The aim of this study was to evaluate the effectiveness of intraoperative gamma probe application in the preoperative planning and for intraoperative localization of osteoid osteoma.
MATERIALS AND METHODS:
The study included a total of 26 patients, comprising 10 females and 16 males with a mean age of 19.6 years (range: 6–45 years), who were prediagnosed with osteoid osteoma based on clinical and radiological findings. All patients were admitted for surgery following bone scintigraphy. All operations were performed with the use of a gamma probe.
RESULTS:
Clinical results were obtained from the postoperative pain evaluation, and excised bone tissue fragments were evaluated histopathologically. Localization of the lesion area was made intraoperatively using a gamma probe in all patients. A statistically significant difference was determined between the radioactivity counts in the normal peripheral bones of the lesion and the lesion area itself (P < 0.001). The ratio of lesion to normal tissue was 4/1 on average. The radioactivity level dropped by 62% on average (30%–90%) in the cavity cleaned after postresectional excision of the pathological tissue. The radioactivity counts in the cavity after resection was found to be significantly lower than those of the lesion area before resection (P < 0.001).
CONCLUSION:
The use of a gamma probe in intraoperative localization following a preoperative injection of99mTc-methylene diphosphonate, is an easy and safe method that helps in the localization of osteoid osteoma nidus during surgery and guides a limited but complete resection of the tumor.
Keywords
Gamma probe
osteoid osteoma
scintigraphy

Introduction
Osteoid osteoma is the third most common benign bone tumor. Incidence has been reported to be 11% of all benign bone tumors and 3% of all primary bone tumors.[1] Osteoid osteoma is prevalent among children and young adults but may also be seen in older individuals and is more common in males. Osteoid osteoma has been described in almost all bones, with the exception of the sternum, and is more frequent in the long bones, especially in the proximal femur.
The diagnosis of osteoid osteoma is based on clinical, radiographic, and scintigraphic findings. Patients often suffer pain for months or years until the lesion is located. The classic radiographic presentation is a small regional lesion up to 2 cm in diameter in the cortical layer of a long bone, surrounded by intense-reactive sclerosis. Bone scintigraphy is the best method for the localization and diagnosis of the lesion. The classic scintigraphic appearance of double density is very specific to osteoid osteoma and is used as a guide for dedicated computed tomography (CT) examination.[2] Although there are reports in the literature of scintigraphically false-negative osteoid osteoma, these are rare situations with no definite explanation. This may occur when the nidus is <5 mm with minimal reactive sclerosis.[3]
With medical treatment of osteoid osteoma, pain may subside after 2–3 years of treatment with oral nonsteroidal anti-inflammatory drugs.[4] However, surgical treatment is a more attractive option as pain disappears immediately postoperatively, and the patients may resume their normal life. En bloc resection and nidus curettage with or without adjuvants are the most frequently performed surgical methods.[5]
Uptake of bone-seeking tracers such as technetium-labeled phosphonates is high in osteoid osteoma and the gamma radiation can be detected with handheld probes. The intraoperative use of a radiation probe to guide detection and resection of osteoid osteoma was first reported in 1980.[6]
The aim of intraoperative use of the gamma probe is to locate the tumor more precisely to reduce the unnecessary bone removal and to ensure complete resection of the nidus to reduce the recurrence rate.
The aim of the present study was to compare the use of an intraoperative handheld gamma probe for the precise localization of the osteoid osteoma nidus with a control group where nidus localization was made using radiographs or fluoroscopy.
Materials and Methods
The study included 26 patients who presented at the Orthopedics and Traumatology Clinic of Dicle University Faculty of Medicine between January 2007 and March 2009, were diagnosed with osteoid osteoma from clinical and radiological evaluations, and underwent surgery with the gamma probe method.
Imaging methods of conventional radiography, CT, and whole-body scintigraphy were used in addition to clinical findings for the diagnosis of osteoid osteoma. No preoperative biopsy was performed on any patient. In addition, bone scintigraphy was performed on all patients before the surgical procedure.
Bone scintigraphy
The patients underwent three-phase bone scintigraphy with an injection of99m Tc-methylene diphosphonate (MDP) at a dosage of 15–20 mCi in adults and at a lower dosage in children on the day of operation. Scintigraphic imaging was applied using a single-detector GE Millennium MPS (GE, Milwaukee, Wisconsin, USA) gamma camera and a low-energy, high-resolution collimator.
A radioactive marker was used to identify and highlight the area on the skin where the activity was increased under the gamma camera. Figure 1 shows the radiological and scintigraphic images of the sample patient.

- (a) X-ray findings: Cortical thickening and periosteal reaction in the left middle femur diaphysis, (b) Computed tomography findings: The left femur diaphysis showing cortical thickening in the posterolateral part and in the middle, compatible with nidus of millimetric diameter, (c) Scintigraphic findings: Increased activity in the left middle femur diaphysis
Osteoid osteoma surgery with intraoperative gamma probe
The patients were admitted for surgery following the completion of the bone scintigraphy with99m Tc-MDP. The patients were administered general or spinal anesthesia. In eight patients with a lesion in the pelvic bones or proximal femur, catheterization was applied to avoid confusion of urinary activity with the lesion.
Following the necessary surgical preparations, the gamma probe (C-Trak system, CareWise Morgan Hill, California, USA) counts were taken on the skin and the region where the surgical incision would be made was determined according to these counts. The incision was started from the point where the highest count was taken.
After revealing the lesion through the incision, the counts of the peripheral normal bone tissue were taken and recorded. Then, the lesion region with the highest count was determined. The surgeon marked the borders of the bone block that was to be excised. The minimal width-block resection of the bone was applied in the region with the highest count. The lesion area was extracted with a curette depending on the anatomic structure of the bone. The bone excision continued until the radioactivity counts of the cavity converged with the counts from the peripheral-sclerotic bone tissue.
All tissues extracted during the surgical procedure were sent to the pathology department for histopathological examination. Intraoperative radiographic control was applied to two patients with proximal femur and acetabulum lesion localization. Preincision skin, preexcision, and postexcision cavity gamma probe counts of the lesion area with possible osteoid osteoma were recorded. The Wilcoxon matched-pairs test was used for statistical analysis of the data.
Follow-up
The clinical results were evaluated with a postoperative pain scale, while the excised bone tissue fragments were evaluated histopathologically. The patients were followed up for complications and recurrence.
Results
A total of 26 patients included in the study comprised 10 females and 16 males with a mean age of 19.6 years (range: 6–45 years).
The primary reason for presentation of the patients at hospital was pain in the limbs caused by osteoid osteoma. The pain was in the form of localized ache that was continuous throughout the day and worsened at night. The pain was significantly reduced with the use of aspirin or nonsteroidal anti-inflammatory drugs. The mean duration of symptoms before admission to hospital was 16 months (range: 2–48 months).
In all 26 patients, no pathological result was determined in any of the routine biochemistry, hemogram, sedimentation, C-reactive protein, and antistreptolysin tests.
A lesion area was observed on the radiographs of all the patients. There was distinct cortical thickening in 21 patients and 8 patients had periosteal reaction. The lesion localization was determined as in the femur in 14 patients, in the tibia in 9, in the acetabulum in 2, and in the fibula in 1.
The lesions observed on radiography were confirmed on CT for all patients. In 17 patients, the nidus was detected on CT. One of the tubular bone lesions was metaphysoepiphyseal, while three were diaphysometaphyseal, and the others were diaphyseal. There was cortical thickening in 22 patients, when evaluated for intraosseous localization, 19 lesions were intracortical, and 7 lesions were intramedullary.
Scintigraphic findings
All patients underwent three-phase bone scintigraphy on the day of operation. The preoperative three-phase bone scintigraphy revealed an increased osteoblastic activity in the lesion areas, observed on the radiographic and CT examinations. The time between the injection and the onset of surgery was mean 4.6 h (range: 4–6 h).
Following the anesthesia induction for all patients, the radioactivity counts were performed on the skin in the lesion and normal regions through the intraoperative gamma probe. The ratio of lesion area skin radioactivity counts to normal tissue radioactivity counts ranged from 2/1 to 17/1 with an average of 6/1.
The surgical incision was started from the point with the highest skin radioactivity count. When the incision was made and the lesion site was revealed, the radioactivity counts of the peripheral bone region were taken. The ratio of gamma probe radioactivity counts from the bone tissue surface in the lesion area to the radioactivity counts from the peripheral bone ranged from 2/1 to 13/1 and was 4/1 on average.
The gamma probe was used to help complete excision after the initial localization of the lesion was determined for resection. The excision was continued until the counts from the lesion area approached the level of counts from the peripheral normal bone.
The signal reduction in the radioactivity counts of the cavity cleared after excision of the pathological tissue was mean 59% (range: 11%–91%). The radioactivity counts on the cavity after excision decreased to twofold lower than the count obtained from the normal peripheral bone tissue in 21 of 26 patients (80%) [Table 1].
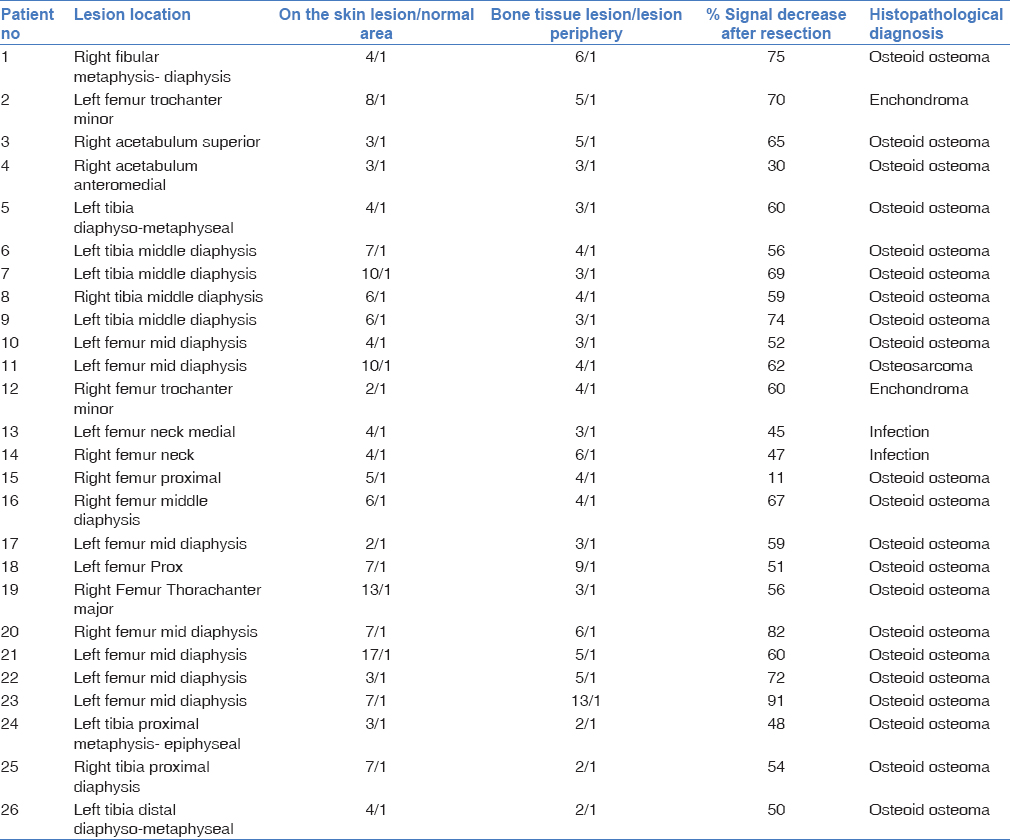
Urinary catheterization was applied to patient #4 as a lesion on the anteromedial acetabulum was in close proximity to the bladder. The lesions were localized using the gamma probe. Intraoperative radiography was performed to check the area of lesion. Intraoperative radiography confirmed excision of the lesion when the signal decreased by 30% in the cavity after resection.
In patient #15, the bone scintigraphy image taken during the examination did not support the diagnosis of osteoid osteoma. Despite numerous small bone excisions during the operation, the signal decrease in the radioactivity counts was 11%, which raised suspicion of the preoperative diagnosis. Following histopathological analysis, osteosarcoma was diagnosed.
Of the 26 patients included in the study, 21 were diagnosed with osteoid osteoma, 2 with enchondroma, 2 with infection, and 1 with osteosarcoma following histopathological analysis.
A statistically significant difference was determined between the counts from the lesion area, and the normal skin before the incision was made (P < 0.001). The difference between the counts from the lesion area and the peripheral bone tissue was found to be statistically significant when the incision was made and the lesion area was revealed (P < 0.001). The difference between the radioactivity counts taken from the cavity after the resection, and the lesion area before the resection was found to be statistically significant at a low level (P < 0.001).
Operating time was mean 54 min (range: 35–80 min). The radionuclide method did not cause the surgery to be prolonged and decreased the amount of the excised bone tissue. Postoperative length of hospital stay was mean 2 days (range: 1–4 days). Mean follow-up duration was 22 months (range: 12–36 months).
Since the bone resections in patients with osteoid osteoma were minimal, no grafting, internal fixation, or external fixation was applied to any patients. No intraoperative or postoperative pathological fracture was encountered. All patients were mobilized in the early postoperative period.
Discussion
The surgical treatment of osteoid osteoma includes a precise localization followed by complete excision of the nidus.[7] It is not necessary to remove the reactive bone tissue surrounding the nidus, as it has been determined that this reactive bone tissue will spontaneously regress in the years, following complete excision of the nidus.[8] Osteoid osteomas are often in inaccessible locations, so to ensure complete excision and to avoid unnecessary excision of peripheral bone tissue, there has to be accurate intraoperative localization. Various methods, such as intraoperative radiological monitoring, CT exploration, marking with intraoperative tetracycline, intraoperative scintigraphy with mobile gamma cameras,[9] and intraoperative gamma probe application,[10] have been used for the intraoperative localization of the nidus.
Intraoperative application of gamma probe for the determination and resection of osteoid osteoma was first used in 1980.[6]
In a study of 58 patients with osteoid osteoma, Perkins and Hardy reported that the detection of increased activity in preoperative bone scintigraphy facilitates the localization of the lesion during surgery.[11] In the present study, the increased uptake area determined on preoperative bone scintigraphy helped to determine the course of operation and facilitated the localization of the lesion during the surgery. There was a statistically significant difference between the normal tissue and the lesion area in the gamma probe radioactivity counts (P < 0.001). The gamma probe was observed to be successful in terms of determining the point of incision and guiding the course of the operation.
In a study performed on 175 patients with osteoid osteoma with the application of intraoperative gamma probe, Wioland andSergent-Alaoui stated that the radioactivity count in the surgical area depended on the amount of injected radioactive substance, the time between the injection and surgery, the thickness of the bone to be excised, and the ability of the nidus to concentrate the diphosphonates. Since osteoid osteoma always shows increased activity on scintigraphy, it was emphasized that the radioguided method is highly successful in localization of the nidus. The primary principle of radioguided surgery for osteoid osteoma was stated to be to determine the uptake of the normal bone adjacent to the suspected bone lesion and to identify the lesion area with the highest count.[12]
Perkins and Hardy stated that a ratio of lesion/normal tissue count at ≥2/1 is positive in terms of pathological radiotracer concentration during intraoperative gamma probe use, with uptake rates depending on tumor type, localization, and the type of radiopharmaceuticals used. In a study performed on 58 patients with osteoid osteoma, the lesion/normal tissue uptake ratio was reported to be mean 3/1 and the highest measured ratio was 30/1 with the use of99m Tc-Hydroxy MDP.[11]
In the present study, the ratio of lesion/normal bone tissue ranged from 2/1 to 13/1 with the use of Tc99m-MDP. In addition, the difference between the gamma probe radioactivity counts of the lesion area, and the normal bone tissue was statistically significant in respect of determining the resection point (P < 0.001). This shows that the gamma probe successfully determined the location of nidus on the bone surface and the lesion area where the resection was to be implemented.
Although it is generally possible to determine lesion localization at the beginning of the operation, it is difficult to show that the pathological tissue has been removed at the end of the operation. As the anatomy of the operated area changes and there is a high-radioactivity concentration in the relevant area in patients with high-perilesional sclerosis, the surgeon cannot be sure about the complete removal of a lesion.[12] Confirmation that the nidus has been completely excised at the end of the operation is the most important step in the surgical treatment of osteoid osteoma. Tumor resection is verified by the decrease in the previously increased activity in the remaining bone tissue.[13]
In a study of seven patients with osteoid osteoma who were operated on with application of intraoperative gamma probe; Hempfing et al. reported that the nidus was localized in all patients and the signal in the cavity after resection decreased by mean 63%.[14]
Wioland andSergent-Alaoui operated on 175 patients with osteoid osteoma and reported decrease in the radioactivity counts rate ranging from 20% to 40% following the excision.[12]
The radioactivity counts of the patients in the present study decreased at a rate of mean 62% (range: 30%–90%) in the cavity cleared after the resection of the pathological tissue. The difference between the radioactivity counts from the lesion area before and after resection was found to be statistically significant (P < 0.001). This demonstrated the relationship between the removal of the lesion and the decrease in the counts. The success of excision is correlated with the decrease in the radioactivity counts.
Perkins and Hardy reported that the radioactivity counts in and around the cavity after resection were higher than the counts in the normal bone area and argued that this was due to peripheral periosteal thickening.[11]
In the current study, the measured radioactivity in the cavity after resection was higher than the radioactivity measured in the normal bone area in all except one of the patients. This condition was thought to be due to the change in anatomical structure caused by perilesional sclerosis and surgical trauma in the cavity.
In the patient with a lesion located in the medial acetabulum, a 30% reduction was seen in the count rate, although the excision of the pathological tissue was shown by the intraoperative radiographic control. This demonstrated that residual urine in the bladder caused increased radioactivity counts in lesions close to this region, despite urinary catheterization.
In a study by Perkins and Hardy, it was stated that high physiological activity in the epiphyseal region may lead to increased gamma probe counts in lesions in this region, especially in children.[11]
In the present study, a lesion was localized in a 6-year-old patient with a metaphysoepiphyseal lesion with a ratio of 2/1 and a reduction of 48% occurred after resection. Due to the physiological radiopharmaceutical involvement in this region, the normal tissue background activity count was high. In three patients with metaphyseal and diaphysometaphyseal lesions, the background activity was measured to be high due to the proximity of the epiphyseal region, and it was observed that the excision was successfully performed with an average signal reduction of 54%. A positive correlation was reported between the good therapy and histopathology.[15] Positive histopathology is the definitive proof that the nidus has been reached, but negative histopathology does not indicate that nidus has not been removed. Difficulties were identified during the selection and processing of samples.[16]
Etchebehere et al. separated 37 patients into two groups in a study, in which they performed surgery with nidus localization through the gamma probe. Surgery was applied under gamma probe guidance in the first group and using the conventional method in the second control group. The results of the nidus resection were compared with the histology or postoperative imaging and the success of the procedure was determined. The histopathology was positive in 81% of the gamma probe group and 67% in the control group.[10] In the present study, 21 of the 26 patients were diagnosed with osteoid osteoma as a result of histopathological analysis and 15 of these 21 patients were determined with nidus in the samples (71%).
Various methods have been developed to demonstrate the presence of nidus in the resected bones. These include examination of the sample under bidirectional conventional radiography and ultraviolet light for tetracycline fluorescence.[17] Multiplanar fluoroscopy may sometimes be helpful if the nidus is in cancellous bone with minimal sclerotic reaction.[18] However, if the tumor is localized in the cortical bone, the reactive sclerosis may hide the nidus on radiography or fluoroscopy. Both methods have disadvantages in respect of obtaining information from the excised bone part. If the sample does not contain the nidus, further resection of the bone is required, resulting in further removal of bone tissue.[19]
With radiofrequency ablation (RFA), successful results have been achieved at rates between 70% and 100%.[18] This procedure does not require patient hospitalization and the loss of bone tissue is minimal. However, RFA has major disadvantages such as being an expensive intervention that requires technical equipment, and being contraindicated in lesions close to major neurological structures (<1.5 cm), and thus not being preferred in the spinal region, insufficient histological material, especially in suspicious lesions, and high radiation exposure. Although it is a percutaneous intervention, general and local complications such as cardiac arrest, aspiration, skin burn, cellulitis, reflex sympathetic dystrophy, and nail loss have been reported in the RFA method.[18]
The advantage of using an intraoperative gamma probe is that the osteoid osteoma surgery can be applied to lesions close to vital structures, and it has a lower radiation dosimetry compared to the CT-scan-guided procedure.[10] This is a more economical treatment option that does not require technical equipment and special operating room equipment, has low rates of recurrence and complications, and a high success rate. With this method, complete excision of the nidus is ensured, while sufficient material is obtained for the histological examination and the peripheral reactive bone tissue is left in its place. Thus, since there is no significant weakening of the bone, early functional use of the extremity is possible.
De Boeck et al. operated on 13 patients considered to have benign bone tumor after the preoperative injection of99m Tc-MDP and used an intraoperative gamma probe. In the histopathological analysis, eight of the 13 patients were diagnosed with osteoid osteoma, two with infection, and three with osteoblastoma. It was claimed that this method allowed the complete resection of the osteoid osteoma nidus and resection of the lesion without causing as much excision of the peripheral bone as in other lesions, and it can be used successfully to relieve pain in patients.[13]
In the present series of 26 patients, 21 were diagnosed with osteoid osteoma, 1 with osteosarcoma, 2 with infection, and 2 with enchondroma as a result of the histopathological analysis. Excision of the lesion was successfully performed with the intraoperative application of the gamma probe in the other four patients in addition to the patients with osteosarcoma and osteoid osteoma. It was also observed that the gamma probe method could be used successfully in the excision of the lesion without unnecessary resection of bone in other benign bone lesions.
Conclusion
In conclusion, the results of this study showed that radioguided surgery implemented with the use of gamma probe after the preoperative injection of99m Tc-MDP is a simple, safe, and economical method that helps the intraoperative localization of the osteoid osteoma nidus and guides the complete resection of a tumor.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am. 1996;27:559-74.
- [CrossRef] [PubMed] [Google Scholar]
- Osteoid osteoma: Radionuclide diagnosis. Radiology. 1984;151:779-84.
- [CrossRef] [PubMed] [Google Scholar]
- Negative radionuclide scan in osteoid osteoma. A case report. Clin Orthop Relat Res. 1984;185:245-9.
- [CrossRef] [Google Scholar]
- Osteoid osteoma. Direct visual identification and intralesional excision of the nidus with minimal removal of bone. J Bone Joint Surg Br. 1999;81:814-20.
- [CrossRef] [Google Scholar]
- Evaluation of a sterilizable radiation probe as an aid to the surgical treatment of osteoid-osteoma. Technical note. J Bone Joint Surg Am. 1983;65:1019-22.
- [CrossRef] [Google Scholar]
- Recurrent osteoid osteoma. Report of a case with a review of the literature. J Bone Joint Surg Br. 1970;52:128-33.
- [CrossRef] [Google Scholar]
- Bone Tumors. (4th). Saint Louis: The C.V. Mosby Company; 1972. p. :89-102.
- [CrossRef] [Google Scholar]
- Intraoperative skeletal scintigraphy for localization of osteoid-osteoma in the spine. Case report. J Bone Joint Surg Am. 1980;62:143-4.
- [CrossRef] [Google Scholar]
- Intraoperative localization of an osteoid-osteoma using a gamma probe. Int Orthop. 2004;28:379-83.
- [CrossRef] [PubMed] [Google Scholar]
- Intra-operative nuclear medicine in surgical practice. Nucl Med Commun. 1996;17:1006-15.
- [CrossRef] [PubMed] [Google Scholar]
- Didactic review of 175 radionuclide-guided excisions of osteoid osteomas. Eur J Nucl Med. 1996;23:1003-11.
- [CrossRef] [PubMed] [Google Scholar]
- Intraoperative radioactive localization of small bone tumours. Int Orthop. 1992;16:172-5.
- [CrossRef] [PubMed] [Google Scholar]
- The indication for gamma probe-guided surgery of spinal osteoid osteomas. Eur Spine J. 2007;16:1668-72.
- [CrossRef] [PubMed] [Google Scholar]
- Osteoid-osteoma: Diagnostic problems. J Bone Joint Surg Am. 1975;57:154-9.
- [CrossRef] [Google Scholar]
- Osteoid-osteoma: Intraoperative tetracycline-fluorescence demonstration of the nidus. J Bone Joint Surg Am. 1986;68:747-51.
- [CrossRef] [Google Scholar]
- An improved technique of intra-operative bone scanning. J Bone Joint Surg Br. 1986;68:643-6.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am. 1998;80:815-21.
- [CrossRef] [PubMed] [Google Scholar]
- Osteoid osteoma of the proximal femur: New techniques in diagnosis and treatment. J Pediatr Orthop. 1984;4:669-72.
- [CrossRef] [PubMed] [Google Scholar]




