
Translate this page into:
Pseudo scapula alata in adolescent: Unwonted diagnosis
Address for correspondence: Dr. Pankaj Kumar Mishra, E-115/4, Shivaji Nagar, Bhopal, Madhya Pradesh, India. E-mail: drpankajv@yahoo.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Mishra PK, Oddam VK, Mishra S, Gohiya A. Pseudo scapula alata in adolescent: Unwonted diagnosis. J Orthop Allied Sci 2018;6:51-3.
Abstract
Winging of scapula is comprehensively known for the serratus anterior palsy and its dynamic presentation. However, on the contrary, pseudo winging may occur due to nonneuromuscular cause like osteochondroma. It is a rare case of pseudo winging of scapula due to osteochondroma in a pubescent girl. This article is for knowledge to share the experience of static scapula alata due to osteochondroma. It was managed by excision and confirmed by histopathological study. Patient relieved completely from her complaints.
Keywords
Osteochondroma
pseudo winging
scapula

Introduction
Osteochondroma comprises the 8.5% of all the bony tumors and 36% of the entire benign bone lesion. It rarely involves the scapula, and only 6% of it confined to scapula.[1] Scapula alata (winging of scapula) is comprehensively known for the serratus anterior palsy and its dynamic presentation. However, on the contrary, pseudo winging (static form of winged scapula) occurs due to nonneuromuscular cause and on the contrary exhibits the static deformities such as kyphoscoliotic deformity of the upper dorsal spine, malunited ribs, and osteochondroma from ventral scapular surface.[2]
If the osteochondroma is situated over the ventral surface of scapula, it remains unnoticed for a long time due to its position as well as due to slow growth unless it grows significantly. Hence, here, we are presenting the rare case of pseudo winging of scapula due to osteochondroma in pubescent girl.
Case Report
A 13-year-old girl presented to our hospital with an unsightly mass over her upper right side of the back. History revealed that she noticed the appearance of swelling about 2 years back. Initially, it was painless and convenient. Since then, it is growing insidiously and has attained the presenting size. Now, it is inconstantly painful (after movement of right upper limb) with unsightly appearance. The patient as well as accompanying was more concerned about cosmetic issue, whenever she used to don the skintight apparels.
On inspection, it appeared like winging of scapula of the right side with smooth skin surface. On palpation, there was prominence of medial border of scapula due to exophytic bony growth from inferomedial surface [Figure 1]. She had the complete painless range of motion of both shoulder. The right scapula was nontender and located at higher level than the left side. The omoplate could be mobilized freely. A gritty sensation was present on palpation during the abduction and adduction movement of the left shoulder. Winging did not exaggerated by any active shoulder maneuvers (protaction).
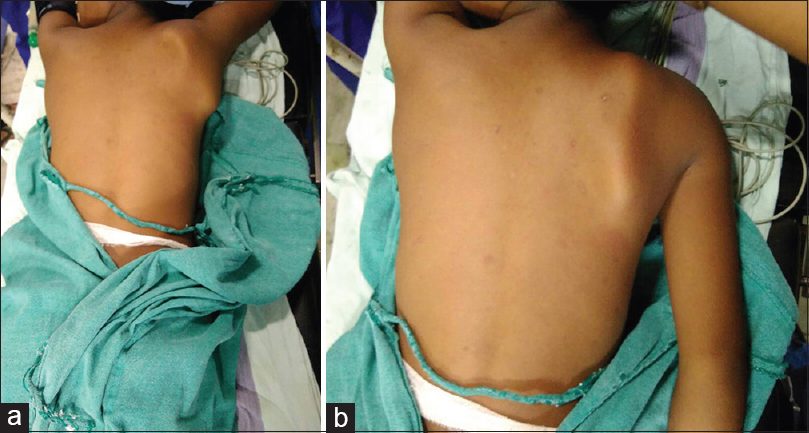
- Clinical photographs (a and b) of patient showing static nature of winging of scapula in different positions of movements
The anteroposterior (AP) and lateral radiograph were obtained, and it showed the pedunculated exophytic bony mass arising from the medial and ventral surface of omoplate [Figure 2] and the clinicoradiological diagnosis of osteochondroma was installed. Further, the computed tomography (CT) scan of the right shoulder sought which reconfirmed the diagnosis of large pedunculated osteochondroma [Figure 3].
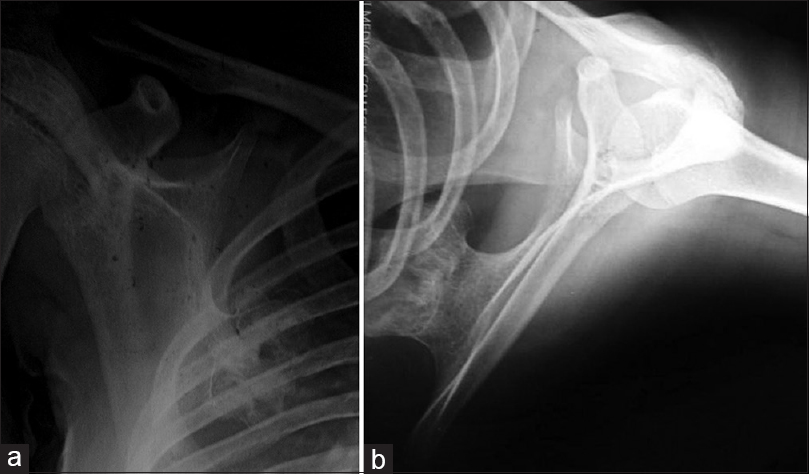
- Anteroposterior (a) and lateral (b) X-rays showing osteochondroma originating from ventral and medial border of right scapula

- Computed tomography (three-dimensional reconstruction) of right scapula showing exophytic pedunculated osteochondroma arising from the inferomedial surface
While it was a painless swelling, but consequently, it had fetched the important deformity. Hence, the informed consent taken and the excision planned. Under general anesthesia and prone position, the longitudinal incision (about 7 cm) given over medial border of the right scapula [Figure 4]. The extraperiosteal resection of osteochondroma achieved along with healthy scapular base [Figure 5]. Biopsy confirmed the clinical diagnosis. As soon as, the pain subsided the ROM exercise started, and she got discharged at third postoperative day. After 6 months of follow-up, she is happy and showed the full range of motion (ROM) at right shoulder with sheer absence of deformity [Figure 6].
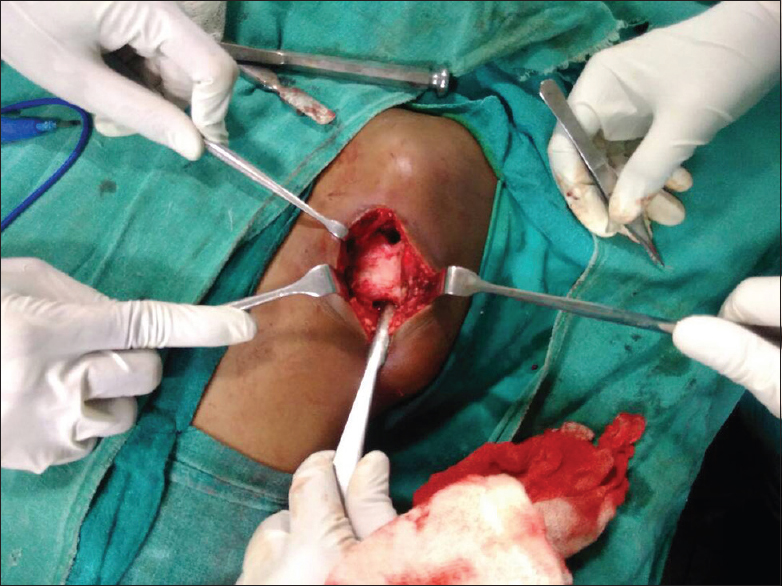
- Medial border incision and base of osteochondroma approached
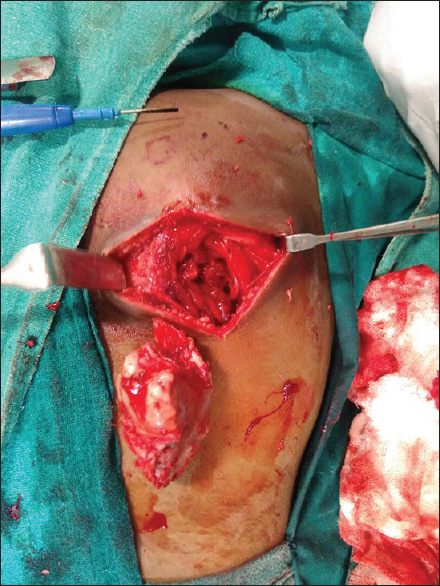
- Excised osteochondroma from the base of scapula

- Follow-up image showing normal contour and positioning of both scapula on active movement of shoulder
Discussion
Scapula alata (winging of scapula) was first mentioned by the Velpeau.[3] Winging of the scapula is characterized by prominence of the vertebral border of scapula and can be classified as dynamic and static type. Long thoracic nerve palsy (nerve of serratus anterior) is the authoritative etiology for prototype of dynamic winging. Due to palsy, the serratus anterior becomes incapable to hold the omoplate to thorax and on active movement (90° forward flexion) it shifts to medial and upward and becomes more prominent.[4] Although there is another variant of dynamic winging due to trapezius palsy (spinal accessory nerve injury) in which scapula moves to lateral and downward on active movement (90° abduction).
On the other hand, the static form of scapula alata is characterized by the scapular prominence at rest, and there is no noticeable metamorphose with active movements. Hence, the static scapula alata has also been entitled as pseudo winging.[5] Usually, the scapula alata follows the somnolent course, and ventral scapular osteochondroma often precipitate the pain and gritty sensation due to scapulothoracic movements. Even the audible crepitus may be due to the abduction and internal rotation of the shoulder.[6]
The AP view of subscapular osteochondroma is not sufficient to delineate it. A true lateral view is needed to clinch the diagnosis to the certain extent. CT scan is more specific for the pathognomonic features of osteochondroma as well as for preoperative planning. Even by CT, the malignant transformation can be suspected due to the presence of poorly or nonmineralized area within the large osteochondroma.[7] Sometimes, the acute development of bursa can be misinterpreted as malignant changes in osteochondroma. In such a condition magnetic resonance imaging (MRI) is useful, which differentiate to bursa and measure the width of cartilaginous cap and significantly predicts the malignant transformation.[8] Electrodiagnostic studies may be helpful in diagnosis as well for prognosis in positional scapular deformity to rule out nerve or muscle pathology and has been routinely favored by some authors.[9]
Operative indication of osteochondroma includes pain, decreased ROM, cosmetic deformity, and local pressure effect. Our case was diagnosed by X-ray and confirmed by CT scan. She was neurologically intact and had indolent course, so we did not go for MRI and electrodiagnostic studies. This article is on the horizon of knowledge for sharing the experience of static scapula alata due to osteochondroma. It was managed by excision and confirmed by histopathological study. Patient relieved completely from her complaints.
Conclusion
Irregardless of its exceptional position the osteochondroma can be conceded for the differential diagnosis for any pubescent presenting with the winging of scapula. Slow growing and benign nature creates problem in diagnosis. Hence, we bring it to core of literature so that the acquaintance of literature and clinical proficiency can overcome the pathology.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Bone and Soft Tissue Tumors: Clinical Features, Imaging, Pathology and Treatment. Wien: Springer; 1999. p. :2.
- [Google Scholar]
- Acquired winged scapula due to solitary bursal exostosis of the scapula. Arch Putti Chir Organi Mov. 1966;21:127-33.
- [Google Scholar]
- Surgical anatomy of trafficking and anatomy of the regions considered in relation to the convertible surgery Traite d'anatomie chirurgicale ou anatomie des regions consideree dans ses rapports avec la chirurgie. Vol 1. Paris: Crevot; 1825. p. :303.
- [Google Scholar]
- Paralysis of the serratus magnus muscle caused by lesions of the long thoracic nerve. JAMA. 1940;114:1994-6.
- [CrossRef] [Google Scholar]
- Pseudowinging of the scapula due to osteochondromata. J Pediatr Orthop. 1985;5:722-4.
- [CrossRef] [PubMed] [Google Scholar]
- Delayed presentation of osteochondroma on the ventral surface of the scapula. Int J Shoulder Surg. 2012;6:61-3.
- [CrossRef] [PubMed] [Google Scholar]
- Chondrosarcoma arising in osteochondroma. Cancer. 1982;49:1890-7.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics. 2000;20:1407-34.
- [CrossRef] [PubMed] [Google Scholar]
- “Pseudowinging” of the scapula secondary to subscapular osteochondroma. Clin Orthop Relat Res. 1982;162:119-24.
- [CrossRef] [Google Scholar]




