
Translate this page into:
Atypical necrotizing fasciitis following surgical treatment for closed ankle fracture dislocation
Address for correspondence: Dr. André Grenho, Orthopaedics and Traumatology Department, Curry Cabral Hospital – Central Lisbon Hospital Centre, 8 Beneficência Street, 1050-099 Lisbon, Portugal. E-mail: andregrenho@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Grenho A, Vieira L, Arcângelo J, Pereira AV. Atypical necrotizing fasciitis following surgical treatment for closed ankle fracture dislocation. J Orthop Allied Sci 2018;6:38-42.
Abstract
We report the case of a 66-year-old female who sustained a closed ankle fracture dislocation of her right ankle (Weber B; AO 44-B3.2). She underwent an open reduction with internal fixation, complicated with a small, superficial wound dehiscence during the initial follow-up. One month after surgery, she developed inflammatory signs on her right ankle, but disregarded them. One week later, she was admitted into the emergency department with infection of her ankle's osteosynthesis, and a necrotizing fasciitis of her left upper limb, neck, and thorax. The patient underwent multiple surgical interventions for the removal of osteosynthesis hardware, fasciotomies, consecutive debridements, and finally a below-the-knee amputation. Streptococcus pyogenes was identified in several cultures as the responsible agent, and directed antibiotic treatment was performed. However, despite all treatments, the patient's clinical status progressively worsened until she eventually deceased, 1 month after admission.
Keywords
Amputation
ankle fracture dislocation
necrotizing fasciitis

Introduction
Necrotizing fasciitis (NF) is a rare and severe soft-tissue infection, leading to necrosis of fascia, subcutaneous fat, and skin. Despite its low incidence of 0.4-3 cases per 100,000 people,[1,2] NF is a life-threatening infection, with reported mortality rates ranging from 30% to 73%.[3-6] Well-known predisposing conditions are trauma, surgery, or injections, but idiopathic cases have also been described in literature.[4,7] There are several risk factors for this condition, the most recognizable being immunodeficiency, diabetes, obesity, liver cirrhosis, or even some medications.[2,8-13]
Causative agents are normally Gram-positive organisms, although some Gram-negative and even Candida spp. have also been identified.[14]
Although identifying such a disease in an early stage may be a challenge, it will definitively improve the patient's outcome and survival.[3,15,16]
A rare presentation of this condition may sometimes occur, with symptoms of NF being identified at a location distant from the original injury site. This has been credited to hematogenous spread of the infective agent, particularly if that agent is a Streptococcus.[17] This may increase difficulty in identifying the underlying condition, especially to the untrained physician.
Case Report
We present the case of a 66-year-old female with prior medical history of obesity, high blood pressure, high blood cholesterol, and hypothyroidism, all medicated and under control. She was admitted through the emergency department (ED) due to a closed fracture dislocation of her right ankle (Weber classification: B; AO classification: 44-B3.2/IC2-MT1-NV1) [Figure 1]. The following day, she underwent open reduction with internal fixation. Prophylactic antibiotic (cefazolin 1 g, TDS) was administered for 24 h. The patient stayed in the hospital for an additional 2 days after surgery, being discharged to outpatient clinic for follow-up, with no significant occurrences during surgery. She did, however, have a small, superficial wound dehiscence, in the initial postoperative period, that was cleaned and dressed with sterile gauze at her local pharmacy.

- Anteroposterior and lateral radiographs of right ankle after reduction and temporary splint of fracture dislocation; Weber classification: B, AO classification: 44-B3.2
One month after the surgery, the patient had developed inflammatory signs on her right ankle, but disregarded them, not seeking medical advice, contrary to what she had been told. One week later, she was admitted again to the ED for fever (39.4°C), polypnea (28 cycles/min), hypotension (88/47 mmHg), and severe inflammatory signs on the left upper extremity, with bullous formation [Figure 2]. Her right ankle surgical wound also presented with inflammatory signs and fluctuation.

- Left forearm showing inflammatory signs and bullous formation
A computed tomography was performed, showing severe soft-tissue edema and changes to normal soft-tissue architecture, in the left shoulder girth and entire left upper limb, as well as in the neck and thorax, with presence of air in subcutaneous soft tissue [Figure 3]. Blood tests showed an elevated C-reactive protein (310.9 mg/L) and creatinine kinase (3709 U/L), acute kidney failure (creatinine/urea – 1.28/62 mg/dL), hyponatremia (129 mmol/L), and high lactate levels (3.73 mmol/L). Laboratory Risk Indicators for Necrotizing Fasciitis (LRINEC) score was 7.

- Computed tomography scan sections showing severe soft-tissue edema and changes to normal soft-tissue architecture, in the left shoulder girth, neck, and thorax, with presence of air in subcutaneous soft tissue
Differential diagnosis was performed between necrotizing and nonnecrotizing skin and soft-tissue infections. In this case, with the aggressive progression, history of surgical wound dehiscence, and a LRINEC score over 6, the NF is the most probable condition.
Due to rapid progression of this condition, with increased intracompartmental pressure of the left upper extremity and extending cellulitis to the neck and thorax, a decision was made to perform decompressive fasciotomies, with extensive soft-tissue debridement of the patient's left upper extremity, neck, thorax, and thoracolumbar areas [Figures 4 and 5]. Since her right ankle also presented signs of NF, hardware was also removed, followed by debridement, lavage, and articulation stabilization with an external fixator. All debrided areas presented with characteristic “dishwater pus” and there was no significant bleeding or resistance to blunt dissection (finger test), all of these were suggestive of NF. Several tissue samples were collected, during surgery, for cultures.

- Decompressive fasciotomies and debridement: left upper limb and shoulder
- Decompressive fasciotomies and debridement: left upper extremity and thoracolumbar area
The patient was admitted to the Intensive Care Unit due to NF with associated sepsis, starting on broad-spectrum antibiotics until the causative agent, Streptococcus pyogenes, was identified on tissue cultures collected from both the ankle and upper limb, as well as blood cultures. The NF was classified as type II, in accordance to the system proposed by Giuliano et al.[18] Antibiotic regimen was adjusted accordingly to the agent's antibiotic susceptibility, starting on piperacillin/tazobactam on day 5 postoperative, in addition to clindamycin that was already being administered.
A Plastic and Orthopedic Surgery joint team performed multiple debridements due to progressive worsening of soft-tissues necrosis. Distal tibial and fibular osteomyelitis, associated with articulation exposure and ankle instability developed, with no potential for joint reconstruction. A multidisciplinary decision was made to perform a below-the-knee amputation. This possibility had already been presented to both the patient and her family, since the beginning of NF treatment, making it simpler to obtain informed consent for this procedure. Upper-limb amputation was also considered, but due to extension of NF to the shoulder girth, neck, and thorax, no safe surgical margins were found for closure after either an amputation or disarticulation.
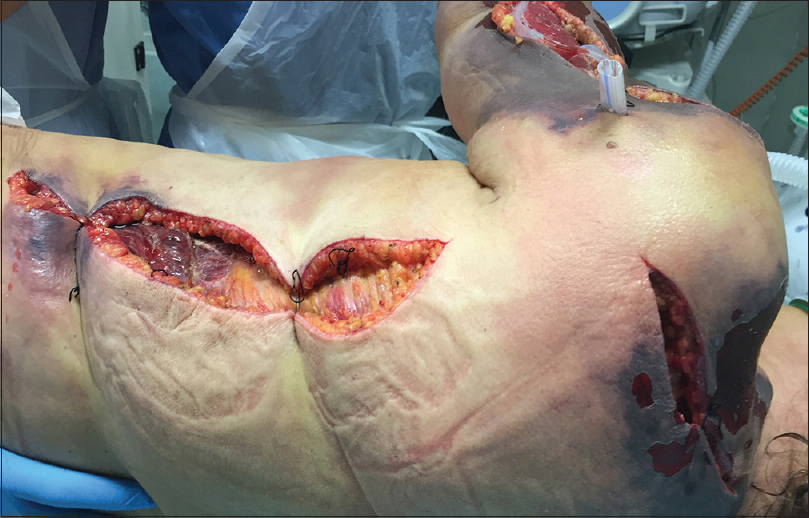
Despite all medical treatments and multiple surgical interventions, the patient's condition progressively worsened, with increased soft-tissue destruction and organ failure [Figures 6 and 7], needing dialysis, as well as respiratory, transfusional, and adrenergic support. The patient eventually deceased, 34 days after being admitted to the Intensive Care Unit, due to multiple organ failure.

- Left upper limb before final debridement

- Left upper limb and neck before final debridement
Discussion
Intense pain associated with inflammatory signs, especially in the presence of a possible entry wound, should make health-care professionals suspicious to the possibility of NF. This diagnosis must be considered even if the suspected entry wound is distant to the affected area.
No single-image study or laboratory finding can correctly and unequivocally differentiate NF from other conditions. Therefore, scoring systems have been developed to help diagnose this clinical entity, the most well known being the LRINEC score, developed by Wong et al., that presents a 92% positive predictive value for NF whenever score is equal or higher than 6.[19-21] Nevertheless, this score is still undergoing validation, with some authors agreeing that other admission markers may have either diagnostic or predictive value, such as high blood lactate and creatinine levels, low blood pressure, or respiratory distress.[11,22,23]
Furthermore, mortality rates rise with the patient's age, female sex, postoperative mechanical respiratory dependence, or organ failure, namely kidney or liver.[15,24]
After suspicion of this diagnosis, early and aggressive surgical procedures are mandatory, with serial debridement of the affected area, foreign material removal, or even amputation, in severe cases, allowing for the best clinical outcome and an improvement in survival rates.[3,8,15] An Intensive Care Unit, with constant patient surveillance, is also mandatory when addressing this situation, further increasing survival chances.[25]
Whenever NF of the extremities is not controllable through serial debridement, an amputation may be required to reduce the amount of devascularized tissue where microbial agents may nest.[23] In their study, Angoules et al. found an amputation rate of 22.3% in a group of 451 patients with limb NF.[26] There is still no score that identifies the need for an amputation, although some authors have tried to use LRINEC to predict the risk for an amputation in a given patient.[27]
Nevertheless, and even when all correct measures are performed, mortality rates can go as high as 35% when NF affects the extremities.[15,26] Furthermore, thoracic involvement will additionally decrease the chances of survival, since aggressive debridement may not be feasible.[25]
Broad-spectrum antibiotics are also deemed necessary, until the infectious agent is isolated in tissue cultures.[11,25] Epidemiology of microorganisms responsible for this condition varies in different studies, with some of these infections being polymicrobial.[3] Nonetheless, group A beta-hemolytic Streptococci, Staphylococcus aureus, and Haemophilus are the most commonly isolated agents in cultures.[11,28]
Finally, as this demanding condition leads to several medical and surgical complications, it is our conviction that only a multidisciplinary approach may offer the best solution for the patient. In addition, both patients and their families must be made aware, early from the beginning of treatment, that an amputation may be necessary in order to increase the chance for survival. It is our opinion that this will facilitate getting consent if this procedure is then deemed necessary.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Acknowledgement
We would like to acknowledge the help of the intensive care unit staff.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Population-based surveillance for group A streptococcal necrotizing fasciitis: Clinical features, prognostic indicators, and microbiologic analysis of seventy-seven cases. Ontario Group A Streptococcal Study. Am J Med. 1997;103:18-24.
- [CrossRef] [PubMed] [Google Scholar]
- Correlates of length of stay, cost of care, and mortality among patients hospitalized for necrotizing fasciitis. Epidemiol Infect. 2007;135:868-76.
- [CrossRef] [PubMed] [Google Scholar]
- Determinants of mortality for necrotizing soft-tissue infections. Ann Surg. 1995;221:558-63.
- [CrossRef] [PubMed] [Google Scholar]
- Necrotizing soft tissue infections after injection therapy: Higher mortality and worse outcome compared to other entry mechanisms. J Infect. 2015;71:312-6.
- [CrossRef] [PubMed] [Google Scholar]
- Review of 58 patients with necrotizing fasciitis in the Netherlands. World J Emerg Surg. 2016;11:21..
- [CrossRef] [PubMed] [Google Scholar]
- Idiopathic necrotizing fasciitis: Risk factors and strategies for management. Am Surg. 2005;71:315-20.
- [CrossRef] [PubMed] [Google Scholar]
- Necrotizing fasciitis: Early recognition and aggressive treatment remain important. J Wound Ostomy Continence Nurs. 1995;22:219-22.
- [CrossRef] [PubMed] [Google Scholar]
- Nonsteroidal anti-inflammatory drugs and necrotising fasciitis. An update. Drug Saf. 1997;17:369-73.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatological complications of obesity. Am J Clin Dermatol. 2002;3:497-506.
- [CrossRef] [PubMed] [Google Scholar]
- Necrotizing fasciitis: Risk factors of mortality. Risk Manag Healthc Policy. 2015;8:1-7.
- [CrossRef] [PubMed] [Google Scholar]
- Necrotizing fasciitis in patients with diabetes mellitus: Clinical characteristics and risk factors for mortality. BMC Infect Dis. 2015;15:417..
- [CrossRef] [PubMed] [Google Scholar]
- Necrotizing fasciitis in three university hospitals in Korea: A change in causative microorganisms and risk factors of mortality during the last decade. Infect Chemother. 2013;45:387-93.
- [CrossRef] [PubMed] [Google Scholar]
- Factors affecting the mortality of necrotizing fasciitis involving the upper extremities. Surg Today. 2008;38:1108-13.
- [CrossRef] [PubMed] [Google Scholar]
- Streptococcal toxic-shock syndrome: Spectrum of disease, pathogenesis, and new concepts in treatment. Emerg Infect Dis. 1995;1:69-78.
- [CrossRef] [PubMed] [Google Scholar]
- Bacteriology of necrotizing fasciitis. Am J Surg. 1977;134:52-7.
- [CrossRef] [PubMed] [Google Scholar]
- The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004;32:1535-41.
- [CrossRef] [PubMed] [Google Scholar]
- A simple model to help distinguish necrotizing fasciitis from nonnecrotizing soft tissue infection. J Am Coll Surg. 2000;191:227-31.
- [CrossRef] [PubMed] [Google Scholar]
- Objective criteria may assist in distinguishing necrotizing fasciitis from nonnecrotizing soft tissue infection. Am J Surg. 2000;179:17-21.
- [CrossRef] [Google Scholar]
- Raised serum lactate: A marker of necrotizing fasciitis? J Plast Reconstr Aesthet Surg. 2013;66:1712-6.
- [CrossRef] [PubMed] [Google Scholar]
- Necrotizing fasciitis of the lower limb: An outcome study of surgical treatment. Med J Malaysia. 2006;61(Suppl A):17-20.
- [Google Scholar]
- Prognostic factors and monomicrobial necrotizing fasciitis: Gram-positive versus gram-negative pathogens. BMC Infect Dis. 2011;11:5..
- [CrossRef] [PubMed] [Google Scholar]
- Craniocervical necrotizing fasciitis with and without thoracic extension: Management strategies and outcome. Am J Otolaryngol. 2009;30:17-23.
- [CrossRef] [PubMed] [Google Scholar]
- Necrotising fasciitis of upper and lower limb: A systematic review. Injury. 2007;38(Suppl 5):S19-26.
- [CrossRef] [PubMed] [Google Scholar]
- Necrotizing fasciitis attended in the emergency department in a tertiary hospital: Evaluation of the LRINEC scale. Rev Esp Cir Ortop Traumatol. 2017;61:265-72.
- [CrossRef] [Google Scholar]
- Report of 2 fatal cases of adult necrotizing fasciitis and toxic shock syndrome caused by Streptococcus agalactiae. Clin Infect Dis. 2000;31:E15-7.
- [CrossRef] [PubMed] [Google Scholar]




