
Translate this page into:
Is there a need for orthogeriatric unit in the Indian hospital setup for managing hip fractures?
Address for correspondence: Dr. Devashis Barick, Department of Orthopedics, NKP Salve Institute of Medical Sciences, Digdoh Hills, Nagpur, Maharashtra, India. E-mail: devashisb@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kedar A, Dwidmuthe S, Barick D. Is there a need for orthogeriatric unit in the Indian hospital setup for managing hip fractures?. J Orthop Allied Sci 2018;6:29-32.
Abstract
AIMS:
The current orthopedic treatment of geriatric hip fracture is inadequate as per the British Orthopaedic Association guidelines and hence to know whether there is a need of orthogeriatric unit in the tertiary hospital setups in India for the management of hip fracture.
METHODOLOGY:
This is a retrospective cross-sectional study, held in tertiary care teaching hospital. The data of patients with age >60 years admitted with hip fracture of 2016–2017 were recorded from medical record section. Age, sex, type of fracture, total duration of admission, delay in surgery, and associated comorbidities were recorded. Patients who had undergone hip surgery electively for other hip or acetabular fracture were excluded from the study.
OBSERVATION:
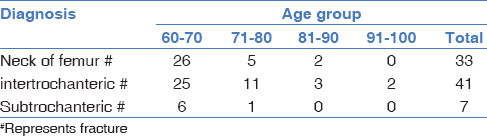
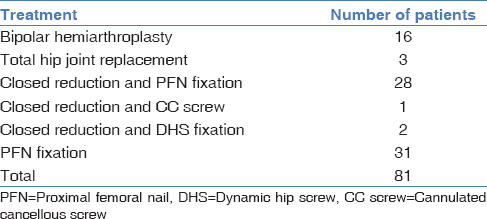
There were a total of 81 cases of hip fracture, of which there were 39 males and 42 females. Seventy-one percent of patients were from the age group of 60–70 years. Maximum number of (54.3%), 44 Patients were having intertrochanteric fracture, followed by fracture of the neck of the femur (35 patients) and subtrochanteric fracture (7 patients). These patients were treated with bipolar hemiarthroplasty, total hip replacement, or with proximal femoral nail fixation or with dynamic hip screw fixation. Hypertension, diabetes mellitus, asthma, and hemiparesis were associated diseases. The maximum stay was 65 days, the minimum stay was 8 days, and the average stay was 13 days. The average delay between admission to surgery was 7 days, maximum of 24 days. We could not analyze the exact cause for delay due to lack of proper data in most of the cases.
CONCLUSION (IMPACT OF STUDY):
Hip fractures in the elderly in India are increasing and not getting the quality of care required. There is an urgent need to the implementation of orthogeriatric unit, and team approach is required to curtail the delay in treatment. This may lead to decrease in the cost of treatment, reduced postfracture morbidity, and mortality. Formation of hip fracture registry would also help us to analyze the present status of care for hip fractures in the elderly.
Keywords
Delay
elderly
fracture neck femur

Introduction
As is evident worldwide, there is a constant increase in the number of persons above the age group of 60 years (geriatric age group) and older. According to the population census 2011 there are 104 million elderly persons in India. From 5.6% in 1961 to 8.6% in 2011, with this growth in the numbers of elderly citizens, the demand for health care has been increasing which is a matter of great concern.[1] This age group, in particular, has been found to be succumbing to medical illness, and a significant number of them also suffer from traumatic conditions such as fragility fractures. They have a slow rate of healing (due to poor bone quality) and also different patterns of injury. It is prudent to prevent morbidity and mortality in the elderly, particularly in cases of fractures. Hip fractures are among the most common fragility fractures and its incidence is increasing due increase in life expectancy across the world.[2,3] Delay in operative intervention is associated with increased morbidity and mortality.[4] One-year mortality is very high after hip fractures in elderly patients.[5]
In this retrospective study, review of common fractures seen in elderly patients and the other associated injuries with it was done, to emphasize on the need for a special and dedicated geriatric unit, in hospital setup. This need is due to the age group that evidently has different physiologies when compared to other age groups, i.e., Low bone mass (osteoporotic) (most fractures are due to porosity of bone) Low immunity (more prone to infection) Other conditions that ail the elderly are hypertension, diabetes mellitus (DM), Alzheimer's disease, urinary incontinence, stroke, dementia, etc.[6] Furthermore, there is a paucity of studies concerning about fractures-related injuries in this age group. In India, particularly, funds allocated to health are very less and have been found to be providing health care to only 25% of total population and the rest are catered to by small-to-medium hospitals in the private setup. Health-care cost is also one of the common causes for poverty in many parts of India.[7] This study was conducted to evaluate the prevalence of hip fractures in elderly patients admitted at his tertiary care hospital. Associated comorbidities were also assessed average delay in surgery and length of hospital stay to understand the gravity of the problem.
Methodology
This is a retrospective cross-sectional study at a tertiary care teaching hospital. Data were obtained from the hospital medical records department for 2016–2017 (June 2016 to June 2017). List of patients with hip fracture who were treated at this hospital was recovered from inpatient ward registers, and subsequently, their hospital records were studied at the hospital record section. Patients with age more than 60 years who have undergone the treatment for hip fractures were included in the study. Patients who had undergone any surgery for acetabular fractures, revision surgery of either hips were excluded from the study. Age, sex, type of fracture, total duration of admission, time from admission to surgery, and associated comorbidities were recorded. The data collected were compiled in Microsoft Excel. Average and mean were calculated wherever required using Microsoft Excel 2010 (Microsoft Windows).
Results
Eighty-one patients with age >60 years underwent surgeries for hip fractures. There were 39 males and 42 females. Seventy-one percent of patients were in the age group of 60–70 years [Table 1]. There were maximum cases of intertrochanteric fractures (44), followed by fractures of the neck of the femur (35) and subtrochanteric fractures (7) [Table 2]. These patients were treated with bipolar hemiarthroplasty, total hip joint replacement, closed reduction with cannulated cancellous screw (although this is not the preferred modality of treatment in this age group, only one patient was the subject of this modality of treatment and this was done as his physiological age appeared to be far <60 years with apparently good bone stock on radiology), or with proximal femoral nail fixation or with dynamic hip screw fixation [Table 3]. Hypertension (22), DM (6), asthma (2), and hemiparesis (2) were the diseases associated in this age group, of which hypertension is most commonly associated. The average stay in hospital was 13 days with range from 8 to 65 days. Average delay between admission and surgery was 7 days. The maximum delay was 24 days. We could not analyze the exact cause for delay due to lack of proper data in most of the cases.

Discussion
According to the WHO global health survey for 2015, the average life expectancy in India has increased to 68.43 years.[8] Hip fractures in the elderly is one of the common causes for seeking hospital treatment in this age group apart from cardiovascular diseases. Extensive data are available regarding the incidence of hip fractures in elderly patients. The geriatric group of patients almost always suffers from osteoporosis and fragility fractures along with other comorbid conditions and associated illnesses that affect their general health and fitness to undergo any surgery. We have conducted this retrospective cross-sectional study to understand the need or requirement of a specialized geriatric unit in our hospital.
The prevalence of hip fractures in geriatric age group due to trauma is very common. Males and females are almost equally affected. In our study, we observed the entire spectrum of hip fractures in these geriatric patients. Patients with intertrochanteric and subtrochanteric fractures usually had their fractures fixed, and only one patient with a transcervical fracture neck of the femur was fixed with cannulated cancellous screws. Irrespective of the modality of fixation or treatment, the average stay in the hospital was about 13 days. It is well documented and known that this stay should be minimized because it affects the mental, physical, and financial condition of patients. (Most of the patients are from low socioeconomic status.)[9] The important finding was that there was an average delay in surgery of 7 days to a maximum of 24 days, which is contrary to the recommendations of the British Orthopaedic Society as given below.
Considering similar findings to this study, the British Orthopaedic Association (BOA) in 2007 has published a blue book on the care of patients with fragility fractures in consultation with geriatric society.[9,10]
The report identifies eight aspects of good care that should be aimed for in every patient:
Prompt admission under the care of an orthopedic consultant
Rapid comprehensive assessment with surgical, medical, and an esthetic input
Minimal delay to surgery
Accurate and well-performed surgery
Prompt mobilization after surgery
Early multidisciplinary team rehabilitation
Early supported discharge and community rehabilitation
Secondary prevention of fractures.
Dhanwal et al.[11] in their study conducted at Rohtak concluded that hip fractures rates in India are intermediate between those in the industrialized world and Africa and similar to some countries like China. The incidence rate of hip fractures in persons above 50 years was found to be 105/100,000 and 159/100,000 in women. The incidence increased with advancing age. There are very few centers which are following the recommendations given by the BOA in India. Jain et al.[12] conducted a study following the BOA recommendations and have concluded that specialized care and early surgery and mobilization gave good clinical outcome in patients with hip fractures.
Elderly patients have their own problems associated with fragility fractures. Hip fractures are one the most difficult fractures to manage in this age group. Many have associated cardiac, renal, or metabolic diseases, diabetic, osteoporosis, and other coexisting medical conditions. The incidence of hip fractures being high in the elderly, carries significant morbidity and mortality. According to Wilkinson et al., 10% will die within 1 month and almost 30% within a year.[13] Only half of the patients go back to their prefracture level after a hip fracture. The presence of associated diseases often delays the orthopedic procedure and also prolongs hospital stay there by increasing the cost of treatment of these fractures.[14] Long duration of hospitalization and complications during the hospital stay are common causes for increased cost as well as poor physiological and psychological outcomes. It has been studied and documented that a team approach reduces the cost of treatment.[14] After institution of geriatric fracture care (GFC) in some centers, they have shown reduction in hospital stay, and time to operation with significant improvement in care and fracture outcome has been seen as early as within 1 year of the institution of GFC.[15] In the late 1990s, a concept of early optimization before surgery evolved and this was termed as the enhanced recovery after surgery (ERAS) protocol or pathway.
The concept of ERAS or the ERAS pathway had come up in 1992 and was initially applied to colorectal surgery by Dr. Henrik Kehlet and over time the benefits of this protocol have been modified and also extended to other surgical disciplines with positive outcomes, more so in the elderly group of patients.[16] It is now being practiced in many western setups and centers where patients with geriatric fractures and those undergoing joint replacement surgery are being rapidly optimized and appropriate surgery is being performed within 48 h of hospital admissions. They have found that this significantly reduces the mortality and morbidity from hip fractures irrespective of the comorbid conditions prevailing either before or after surgery. The crux of the ERAS pathway is the presence of a dedicated team of doctors, anesthetist, orthopedic surgeon, and geriatric specialist who are attending to the patients preoperatively and in the postoperative period. The emphasis has been to optimize these patients early for surgery. The implementation of the multimodal ERAS pathway reduces operative stress, supports organ function, reduces morbidity, and accelerates convalescence. Thereby significantly improving the functional capacity of the patients during the convalescence phase, it fast-tracks the patients on the road to recovery.
The ERAS has demonstrated continued reductions in length of stay, without any evidence of increased complications. The improved gains in rehabilitative efficiency also bestow a considerable economic incentive to orthopedic units. Multimodal optimization is an important part of this process and is often achieved through preoperative patient seminars or clinics, run by nursing staff and therapy services. These have been shown to be beneficial and can help to reduce length of stay, achieve earlier ambulation, and allow for discharge back to a usual place of residence.[17] The improvements to quality of care and postoperative efficiency which are gained by implementing ERAS programs are thought to be largely due to the underlying organizational structure. If the patient pathway is well structured and highly standardized, with developmental input from all members of the multidisciplinary team, then improvements to patient care are likely to manifest.[18] These benefits are universal and confer an advantage regardless of the patients' preoperative condition.[19]
Our study, of course, has certain limitations such as it is a retrospective cross-sectional study with less number of patients in the study. Multicenter studies are required to substantiate the findings in this study. We also do not have data regarding readmission in these patients. We could not investigate the cause for delay in surgery in these patients. However, it seemed evident that most patients went in for delayed surgery as time was consumed in the course of optimizing them for surgery.
Conclusion
Hip fractures in the elderly in India are increasing, and unfortunately, these patients are not getting the quality of care required. There is an urgent need for implementation of orthogeriatric unit, and team approach is required to curtail the delay in treatment. The interdepartmental coordination and teamwork as emphasized in the ERAS protocols if implemented can also significantly alter the course of recovery of patients. It was strongly felt that even in the absence of dedicated orthogeriatric units, the introduction and implementation of ERAS protocols should be attempted and individualized as per needs and limitations of respective institutions. This would lead to decrease the cost of treatment, reduced postfracture morbidity, and mortality. Formation of a hip fracture registry would also help us to analyze the present status of care for hip fractures in the elderly.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Available from: http://mospi.nic.in/sites/default/files/publication_reports/ElderlyinIndia_2016.pdf (accessed )
- Hip fractures in the elderly: A world-wide projection. Osteoporos Int. 1992;2:285-9.
- [Google Scholar]
- Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int. 2011;22:1277-88.
- [CrossRef] [PubMed] [Google Scholar]
- Mortality associated with delay in operation after hip fracture: Observational study. BMJ. 2006;332:947-51.
- [CrossRef] [PubMed] [Google Scholar]
- The 1-year mortality of patients treated in a hip fracture program for elders. Geriatr Orthop Surg Rehabil. 2010;1:6-14.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of comorbidities on hospitalization costs following hip fracture. J Bone Joint Surg Am. 2012;94:9-17.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: http://www.who.int/countries/ind/en (accessed )
- Identifying a standard set of outcome parameters for the evaluation of orthogeriatric co-management for hip fractures. Osteoporosis Int. 2014;12:63..
- [Google Scholar]
- Managing osteoporosis in patients with fragility fractures: Did the British Orthopaedic Association guidelines have any impact? Ann R Coll Surg Engl. 2007;89:504-9.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence of hip fracture in Rohtak district, North India. Arch Osteoporos. 2013;8:135..
- [CrossRef] [PubMed] [Google Scholar]
- Early results of a geriatric hip fracture program in India for femoral neck fracture. Geriatr Orthop Surg Rehabil. 2015;6:42-6.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: http://eprints.nottingham.ac.uk/38469/1/ThesisFinal.pdf (accessed )
- The cost of osteoporotic fractures in the UK: Projections for 2000–2020. J Med Econ. 2001;4:51-62.
- [CrossRef] [Google Scholar]
- Implementation of a co-managed geriatric fracture center reduces hospital stay and time-to-operation in elderly femoral neck fracture patients. Arch Orthop Trauma Surg. 2013;133:1527-31.
- [CrossRef] [PubMed] [Google Scholar]
- Enhanced recovery after surgery (ERAS): An orthopaedic perspective. J Perioper Pract. 2013;23:228-32.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical pathways in hip and knee arthroplasty: A prospective randomised controlled study. Med J Aust. 1999;170:59-62.
- [CrossRef] [PubMed] [Google Scholar]
- Multidisciplinary rehabilitation programmes following joint replacement at the hip and knee in chronic arthropathy. Cochrane Database Syst Rev (2):CD004957.
- [CrossRef] [PubMed] [Google Scholar]
- Enhanced recovery program in total hip arthroplasty. Indian J Orthop. 2012;46:407-12.
- [CrossRef] [PubMed] [Google Scholar]




