
Translate this page into:
Endoscopic transiliac approach to L5-S1 disc and foramen, technique and results
Address for correspondence: Dr. K. Mahesha, Maithri Speciality Clinics, Near Hotel Maya International, Bendoorwell, Mangalore, Karnataka, India. E-mail: maheshakb@yahoo.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Mahesha K. Endoscopic transiliac approach to L5-S1 disc and foramen, technique and results. J Orthop Allied Sci 2018;6:22-8.
Abstract
BACKGROUND:
Transforaminal endoscopic discectomy has become popular due to its advantages over open discectomy. However, transforaminal endoscopic surgery may be difficult to perform at L5-S1 level in some cases due to anatomic variations such as high iliac crest. Endoscopic transiliac approach is an option for patients with high iliac crest or narrow foramen. The aim of this retrospective study was to describe the technique, analyse the results and complications.
MATERIALS AND METHODS:
10 patients with variety of L5-S1 disc pathology who were treated with endoscopic transiliac surgery under local anaesthesia from June 2015 to December 2016 were included in the study. Clinical follow up was done at one month, three months, six months, one year. Outcome was assessed using modified Macnab's criteria.
RESULTS:
All patients had immediate relief from symptoms. Excellent outcome was noted in eight patients, Good outcome in one patient, and fair result in one patient. No patient had any complications. No patient required conversion to open or alternative procedure. Mean hospital stay was 1 day.
CONCLUSIONS:
Endoscopic transiliac approach is safe and effective in lumbosacral disc pathologies. Transiliac approach removes the limitations of transforaminal approach for L5-S1 disc space. Transiliac approach is the only versatile minimally invasive approach to lumbosacral junction which can tackle variety of clinical conditions.
Keywords
Endoscopic discectomy
transiliac approach
transforaminal discectomy

Introduction
Percutaneous endoscopic lumbar discectomy was first introduced in 1983 by Kambin and Gellman.[1] A study by Kambin and Schaffer used arthroscope for visualization and excision of the disc.[2] Yeung AT developed rigid working channel endoscope for transforaminal endoscopic discectomy.[3] Transforaminal endoscopic disc surgery has several advantages over open surgery such as less damage to paraspinal muscle, rapid recovery, and less complications. However, transforaminal endoscopic surgery may be difficult to perform at L5–S1 level in some cases due to anatomic variations such as high iliac crest.[4,5] The minimally invasive options for L5–S1 level include supra-iliac transforaminal decompression, foraminoplasty ventral epidural approach, transiliac transforaminal approach, and interlaminar approach.[6] Osman and Marsolais reported a cadaver study on the feasibility of the transiliac approach for L5–S1 in 1997 and concluded that transiliac approach to the lumbosacral junction is safe.[7] Osman et al. in their study reported the results of transiliac approach in 15 patients for L5–S1 disc pathology. He concluded that endoscopic transiliac approach to the L5–S1 disc and foramen is feasible and safe.[8] There are very few studies in the literature regarding transiliac approach for the lumbosacral junction. The purpose of this study is to analyze the results of endoscopic discectomy with transiliac approach using a simple technique.
Materials and Methods
Ten patients with lumbar disc prolapse L5–S1 treated with endoscopic transiliac discectomy and decompression between June 2015 and December 2016 were included in the study. This was a retrospective study with a minimum follow-up period of 1 year. The indications for surgery were patients with L5–S1 disc prolapse with the failed conservative treatment of 6 weeks duration, patients with recurrent disc prolapse and patients with foraminal stenosis. The duration of symptoms ranged from 6 weeks to 1 year. All patients had preoperative X-rays, and magnetic resonance imaging (MRI) scans of the lumbosacral spine, and clinical findings were correlated with MRI pictures. Patients with instability were excluded from the study.
Procedure
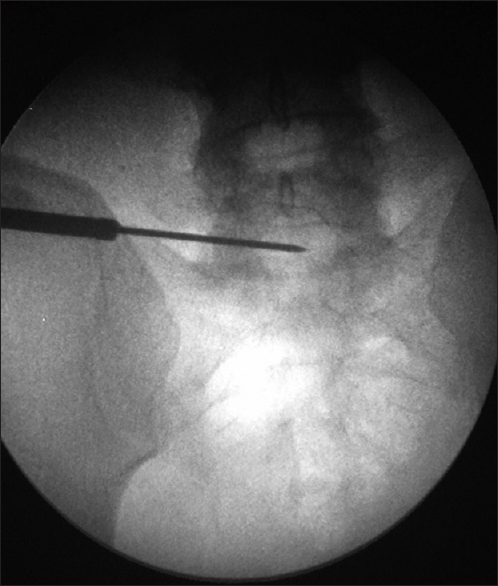
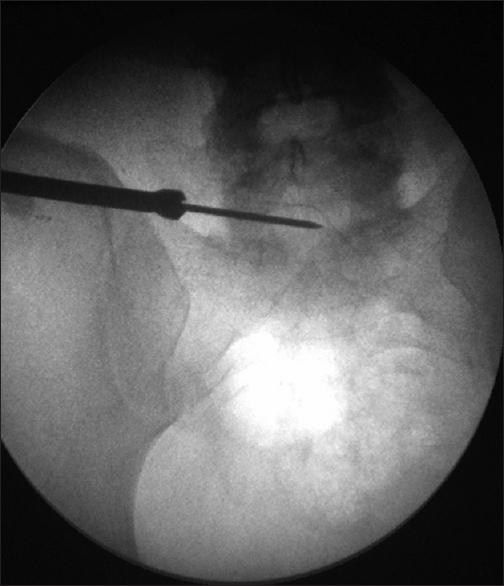
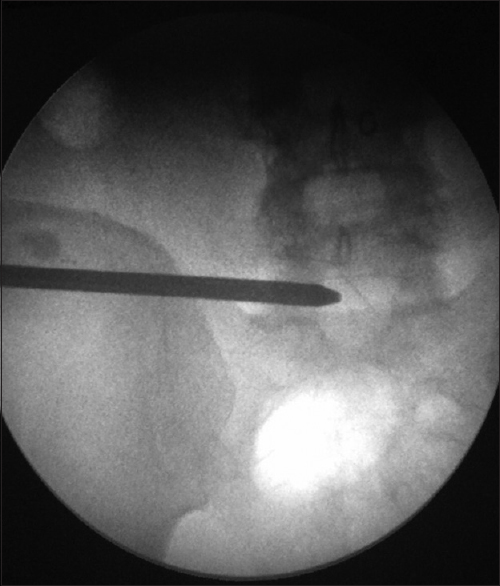
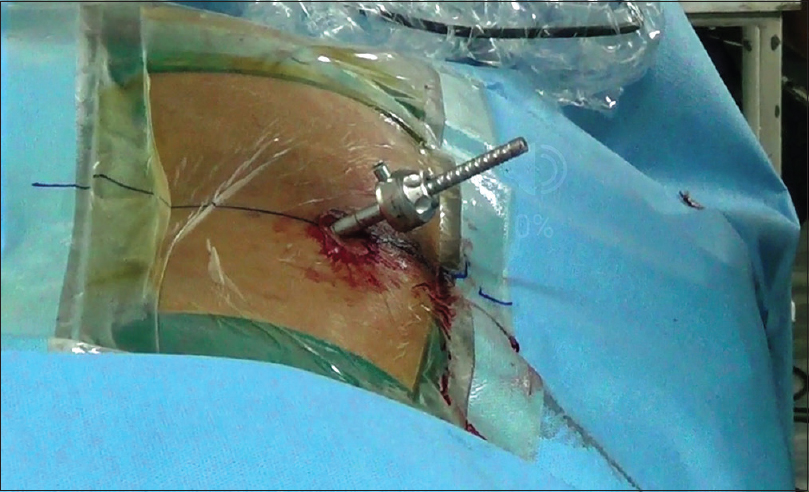
Preoperatively, all patients were administered third-generation cephalosporin and amikacin intravenously as prophylactic antibiotics. All patients were given injection diclofenac 75 mg intramuscularly 15 min before starting the procedure for pain relief. Tranexamic acid injection 1 g was given intravenously to reduce bone bleeding. All procedures were performed under local anesthesia and sedation. The patient is positioned prone over a radiolucent table so that anteroposterior (AP) and lateral images are obtained. Parts were prepared, painted, and draped. Marking was done using a needle and sterile marker pen. A transverse line was drawn at the level of L5–S1 disc space under AP (Ferguson) image. Another oblique line was drawn along the disc space in the lateral view. Point of intersection of the two lines was the starting point which is generally 12 cm–13 cm lateral to midline [Figure 1]. These lines and images correspond to the final position of K-wire [Figures 2 and 3]. The marking depends on the site of pathology. Local anesthetic was injected into the skin, subcutaneous tissue, muscle, and to the periosteum of the posterior ileum. A 7 mm long stab incision was made using 11 blade knife. A 2 mm × 300 mm long K-wire was drilled across the ileum into the L5–S1 disc space using a battery drill. Target point for the tip of the K-wire was medial pedicle line in AP view and posterior border of the disc in lateral view. Alternatively, 2.3 mm beath pin can be used instead of K wire. Beath pin is longer, thicker, and stronger than K wire. Once the wire is in the proper place, it is advanced to the center of the disc space in AP view [Figure 2]. In the lateral view, the tip of the wire should be in the posterior third of disc space [Figure 3]. A 6 mm flower tip cannulated reamer was used to enlarge the transiliac window using the battery drill [Figure 4]. Reaming was done at a low rpm to avoid pain. In general, slow reaming is painless. If required, a local anesthetic can be injected into the track. Reaming was monitored under image intensifier [Figure 5]. Once the posterior ileum is reamed, there is a loss of resistance, and this was confirmed under image intensifier. Reamer was withdrawn retaining the K-wire. Eight mm cannulated reamer was taken and reaming is done over the K-wire [Figure 6]. Most of the cannula have an outer diameter of 8 mm and hence, reaming up to 8 mm was sufficient. If required, reaming can be done with bigger diameter (9, 10 mm) reamers. These reamers and K-wires are from the anterior cruciate reconstruction set. In general, ala of the sacrum does not come in the way of the approach. Rarely if the ala of the sacrum comes in the way of transiliac approach, it can be reamed. This is author's technique of sequential reaming which is very well tolerated by the patient. Once the reaming is complete, K-wire was removed. An 18G needle was inserted into the disc space under image control [Figures 7 and 8]. A guidewire was passed into the disc space, and the needle was removed. A dilator was inserted over the guidewire into the disc space [Figure 9]. The annulus was infiltrated with local anesthetic using the side channel of the dilator. Once the dilator is in the center of disc space in AP view and in the posterior third of the disc space in lateral view, guidewire was removed, and operation sheath is advanced over the dilator [Figures 10 and 11]. The dilator was removed and endoscope (GORE System from KARL STORZ GmbH and Co, KG Tuttlingen, Germany) was inserted. The disc was directly visualized and removed using inside-out technique [Figure 12]. The annular tear was visualized. Annuloplasty was done using a radiofrequency probe. Traversing root was completely decompressed [Figure 13]. If there was foraminal disc herniation, it was visualized and removed. If there was foraminal stenosis, it was decompressed using various tools such as burr, angled punch, angled forceps, flavum knife, and articulating curette. Bleeding was controlled with the radiofrequency probe. In case of stenosis, the exiting root, dural sac, traversing root, and dorsal root ganglion were decompressed. Patient confirmed relief of pain at the end of the procedure. The steroid was injected into the foramen at the end of the procedure in case of foraminoplasty. Endoscope and cannula were removed. Wound was closed with a subcutaneous 2-0 vicryl suture. Sterile dressing was applied. Postoperatively, the patient was monitored in the intensive care unit for 1 h. The patient was permitted to sit, stand, and walk 1 h after the procedure. The patient was kept overnight and discharged next day. Postoperative MRI scan was done on disc extrusions to confirm complete decompression [Figures 14 and 15]. Postoperative computed tomography (CT) scan was done in the first case to document the safety of transiliac window [Figure 16].
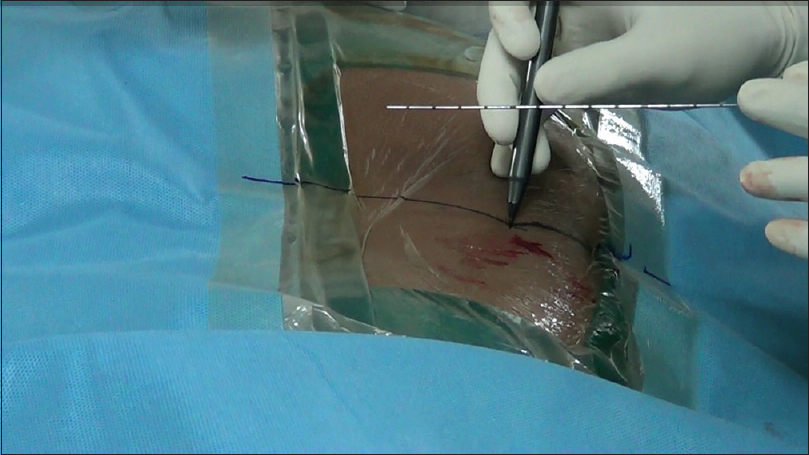
- Marking with needle and sterile pen
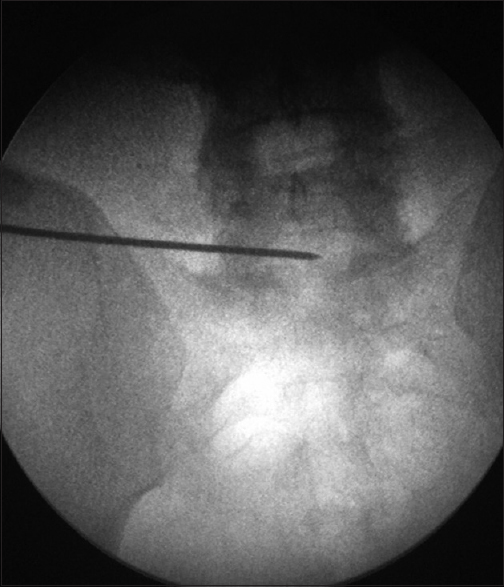
- Position of transiliac K wire in AP view
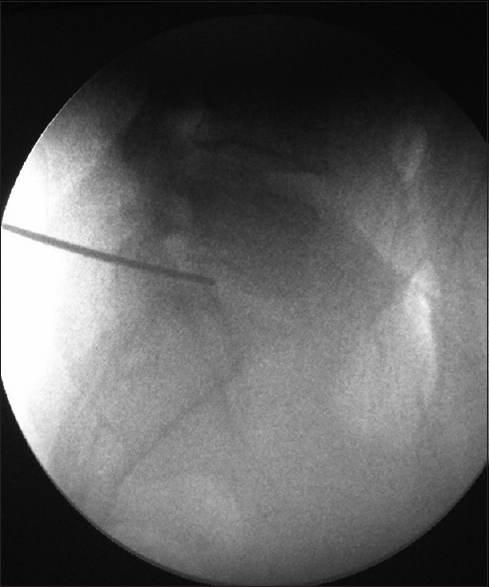
- Position of transiliac K wire in lateral view
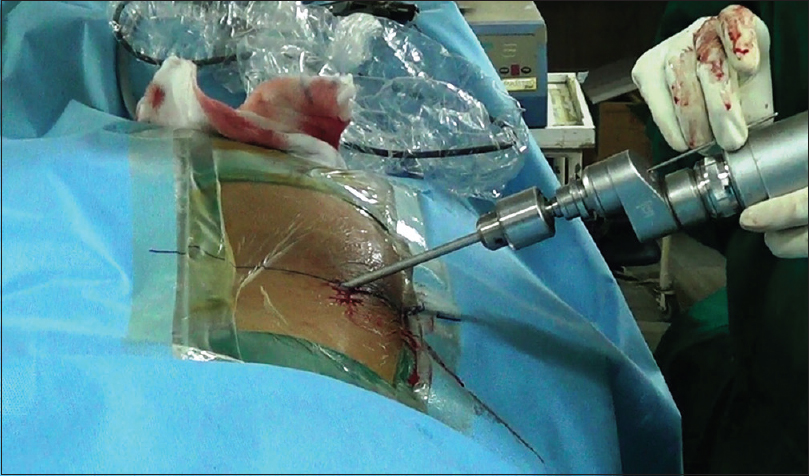
- Reaming with reamer and power drill
- Transiliac reaming with 6 mm reamer
- Transiliac reaming with 8 mm reamer
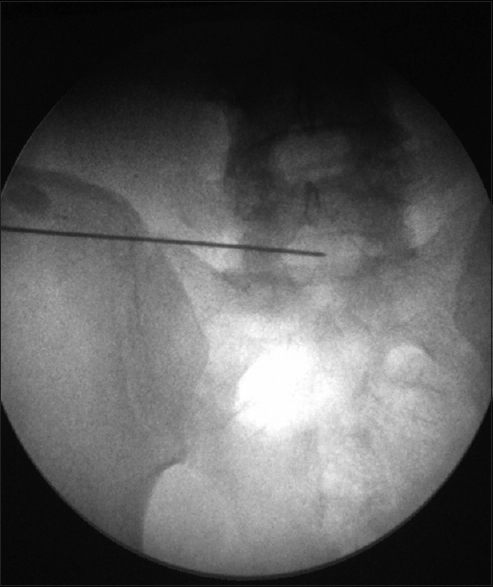
- Insertion of 18 G needle through transiliac window AP view
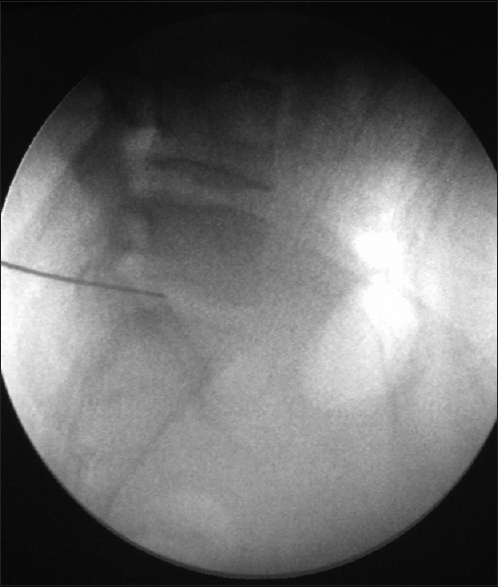
- Insertion of 18 G needle through transiliac window lateral view
- Insertion of dilator

- Insertion of dilator over the cannula
- Dilator and cannula in situ

- Transiliac endoscopic discectomy
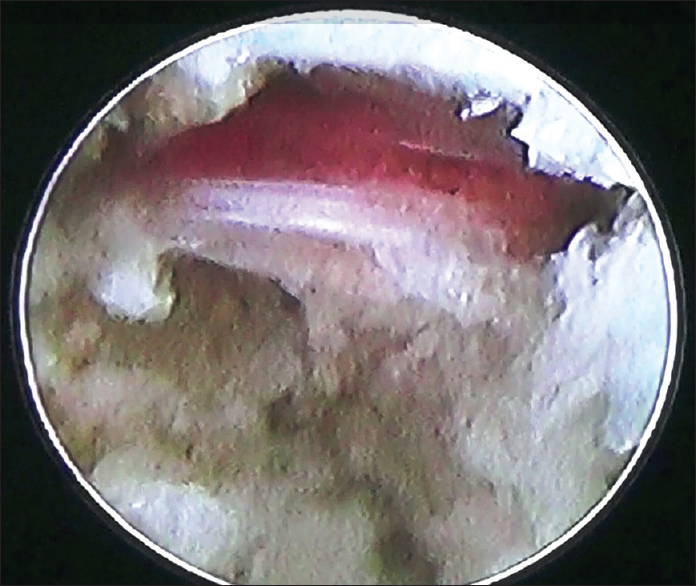
- Endoscopic view of decompressed nerve root
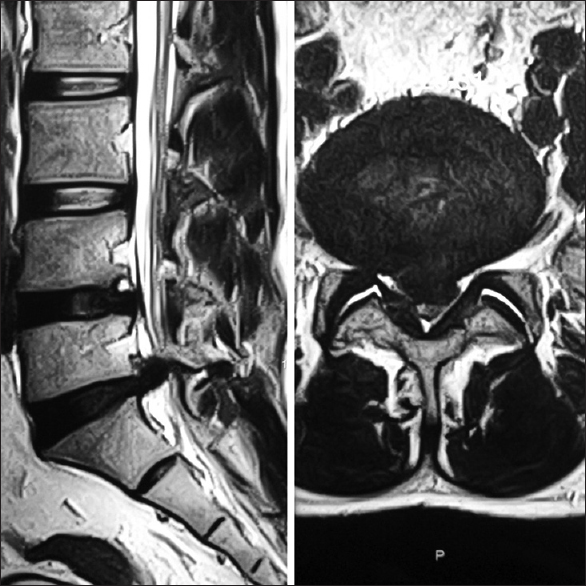
- Pre operative MRI scan

- Post operative MRI scan
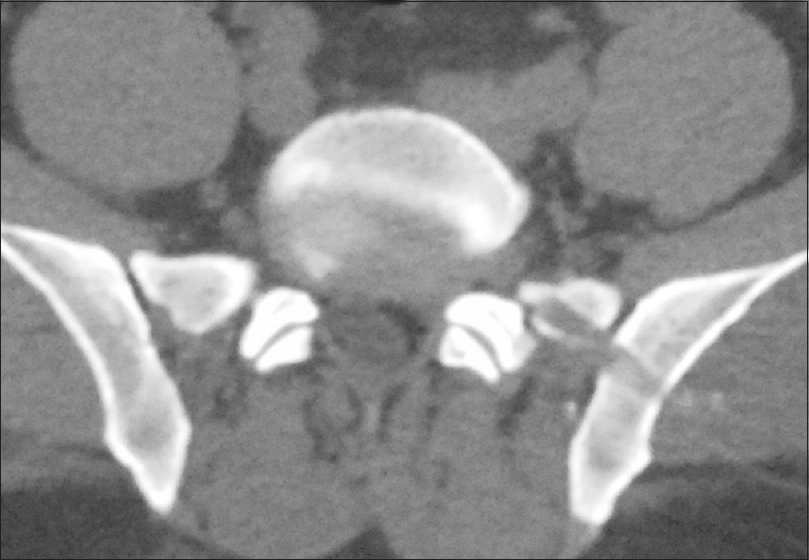
- Post operative CT scan showing transiliac window
Patients were advised to take rest at home for 1 month. Patients are advised to resume light activity as early as possible depending on pain tolerance. Follow-up was done at 1 month, 3 months, 6 months, 1 year, and then yearly after the surgery. At follow-up, the patient was assessed regarding his symptoms, neurologic status, visual analog scale (VAS), and Oswestry disability index (ODI). A modified Macnab criteria were used for grading the results.
Results
The mean age of patients was 40.29 years (range 26–84 years). There were seven males and three females. There were three disc protrusions, two extrusions, one foramianal disc, two cases of foraminal stenosis and two cases of recurrent disc protrusions. Five patients had right-sided radiculopathy, 5 patients had left-sided radiculopathy. The mean operative time for making the transiliac window was 20 min (Range 10–45 min). The mean operative time for the entire transiliac endoscopic decompression was 70 min (Range 50–120 min). The mean blood loss was 20 ml. The mean hospital stay was 1 day. No patient required conversion to alternative approach or open procedure.
Of the ten patients, the excellent outcome was noted in eight patients, good outcome in one patient, and fair result in one patient. The fair result was seen in a patient who had two previous open surgeries. No patient had a poor outcome. The mean VAS reduced from 8 preoperatively to 1.6 postoperatively (P < 0.001). ODI also showed marked improvement from a preoperative 48% to a postoperative 6% (P < 0.001). For statistical analysis of both VAS and ODI, Student's paired t-test was used and found to be highly significant. No patient had any complication. It is important to note that two patients were above 75 years of age with multiple medical problems. These patients had a high risk for general anesthesia. However, transforaminal surgery under local anesthesia has a minimum anesthetic risk.
Discussion
The lumbosacral junction is a difficult area for spine surgery due to the complex anatomy.[8] The minimally invasive options include supra-iliac transforaminal decompression, foraminoplastic ventral epidural approach, transiliac transforaminal approach and interlaminar approach.[6-8] The difficulty in using transforaminal approach to L5–S1 space is due to various anatomic factors such as high iliac crest, narrow intertransverse space, wide facet joint of L5–S1, thick transverse process, and ala of the sacrum.[6,9] Even in situ ations where the pelvic anatomy is normal, the normal trajectory of suprailiac approach is downward, and this is not suitable for central disc herniation or up migrated disc fragment. Elderly patients with foraminal stenosis of L5–S1 require decompression of upper part of foramen which is difficult with the regular supra-iliac approach. In situ ations where the L5–S1 is deeply seated in the pelvis, the supra-iliac approach may be impossible, or risks injury to the exiting L5 nerve root or the S1 endplate.
Lee et al. in their study reported foraminoplastic ventral epidural approach for L5–S1 disc herniation[4] in 25 patients. This approach has limitations of any supra-iliac approach because the trajectory is always limited by the iliac crest. Lee et al. reported that 8% of their patients required conversion to open procedure due to incomplete decompression or recurrence.[6]
Choi et al. reported a percutaneous interlaminar approach for selected L5–S1 disc herniation in 67 patients. Favorable result was obtained in 90% of cases. However, they reported complications such as dural tear in two cases, dysesthesia in nine cases, recurrence in one case, conversion to open surgery in two cases. It is important to note that percutaneous interlaminar approach is not suitable for cases with stenosis, previous open surgery, far lateral and foraminal disc herniations, narrow interlaminar space, and significant motor deficits.[9] Percutaneous interlaminar has limited access to the inside of the disc space. This is the same drawback of traditional surgery without the inside view of the disc where the problem started as an annular tear.[10] Hence, percutaneous interlaminar approach has limited indications and more complications.
Because alternative approaches have significant limitations, the only direct approach for L5–S1 space is the endoscopic transiliac approach. The cadaver study by Osman and Marsolais clearly revealed there were no neural or vascular structures in the neighborhood of the transiliac access channel. Significantly, there was minimal risk of penetration into the pelvic cavity or retroperitoneal space.[7] Embryologically, the ilium derives from the same mesenchymal tissue as the paraspinal muscles which are traversed by the more cephalad transforaminal endoscopic procedures, hence, it is not surprising that the track is posterior to the posterior wall of the pelvic cavity.
Transiliac window is 4.16 cm anterolateral to the posterosuperior iliac spine.
Transiliac track is posterior to the sacral ala, and cephalad to the S1 pedicle. Transiliac track does not violate the retroperitoneal space and is a safe distance from the lumbosacral trunk. The superior gluteal neurovascular bundle is 4.8 cm caudal to the transiliac window.[7] By taking a lateral entry and remaining posterior, one can avoid major complications.[8]
Osman et al. reported transiliac endoscopic surgery in 15 patients with favorable results. He reported postoperative dysesthesia in two cases which resolved after 3 weeks. He used preoperative MRI scan for marking the entry point.[8] Bai et al. reported transiliac endoscopic discectomy in 19 patients. They used preoperative CT scan for marking the entry point. They also used preoperative ultrasound to rule out vascular anomalies of the superior gluteal artery. According to MacNab's criteria, excellent results were seen in 14 patients, good results in 4 patients and fair result in one patient.[11]
In the present study, preoperative marking with CT or MRI was not used. Author has used the traditional marking in fluoroscopy under AP and lateral images to get the entry point. The entry point is dependent on the site of the herniation or compression. Location of perfect entry point and the target is vital to the success of the transiliac endoscopic surgery. Authors have used simple orthopedic K-wire, cannulated reamers and battery drill for making the transiliac approach. The technique is simple, safe, and well tolerated under local anesthesia. None of the patients required additional sedation or analgesia for making the transiliac window. As the cannula remains inside a bony tunnel, it permits limited mobility of the cannula. It is safe to drill a transiliac tunnel of 10 mm diameter. 10 mm tunnel permits some mobility to the cannula, but not free mobility. In the present series, 8 mm tunnel was sufficient in all patients. Complete decompression was achieved in all cases, and no patient required open surgery. No complication was encountered in this series. This series includes a variety of conditions such as migrated disc, recurrent disc, and foraminal disc and foraminal stenosis with the satisfactory result and no complications. This proves that transiliac endoscopic decompression is a versatile and safe approach for lumbosacral junction.
The advantages of transiliac approach include easy removal of central, foraminal or up migrated disc fragment, no damage to the endplate of S1, reduced risk of exiting nerve injury, ease of foraminoplasty, and epidural access. The disadvantages include slightly increased blood loss and operating time, limited mobility of the cannula.
Limitations of this study
The sample size of this study is small, and it is a retrospective study with a short follow-up. The present study includes spectrum of pathologies such as simple disc protrusion, up migrated extrusion, foraminal disc, recurrent disc, and foraminal stenosis. A study with large sample size and long-term follow-up are needed.
Conclusions
Transiliac endoscopic discectomy is a safe and effective in lumbosacral disc pathologies. The procedure can be performed with marking under fluoroscopy with simple orthopedic instruments and endoscope under local anesthesia. Transiliac approach removes the limitations of transforaminal approach for L5–S1 disc space. Transiliac approach is the only versatile minimally invasive approach to lumbosacral junction which can tackle a variety of clinical conditions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Percuraneous lateral discectomy of the lumbar spine: A preliminary report. Clin Orthop Relat Res. 1983;174:127-32.
- [CrossRef] [Google Scholar]
- Percutaneous lumbar discectomy. Review of 100 patients and current practice. Clin Orthop Relat Res. 1989;238:24-34.
- [CrossRef] [Google Scholar]
- Minimally invasive disc surgery with the yeung endoscopic spine system (YESS) Surg Technol Int. 1999;8:267-77.
- [Google Scholar]
- Percutaneous endoscopic lumbar discectomy: Results of first 100 cases. Indian J Orthop. 2017;51:36-42.
- [CrossRef] [PubMed] [Google Scholar]
- The “inside out” transforaminal technique to treat lumbar spinal pain in an awake and aware patient under local anesthesia: Results and a review of the literature. Int J Spine Surg. 2014;8:28..
- [CrossRef] [PubMed] [Google Scholar]
- Foraminoplastic ventral epidural approach for removal of extruded herniated fragment at the L5-S1 level. Neurol Med Chir (Tokyo). 2010;50:1074-8.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic transiliac approach to L5-S1 disc and foramen. A cadaver study. Spine (Phila Pa 1976). 1997;22:1259-63.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopic trans-iliac approach to L5-S1 disc and foramen - a report on clinical experience. Int J Spine Surg. 2014;8:20..
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous endoscopic interlaminar discectomy for intracanalicular disc herniations at L5-S1 using a rigid working channel endoscope. Neurosurgery. 2006;58:ONS59-68.
- [CrossRef] [PubMed] [Google Scholar]
- New emerging gore matrix: Basis of stitchless spine surgery under local anesthesia. J Orthop Allied Sci. 2017;5:1-5.
- [Google Scholar]
- Application of transiliac approach to intervertebral endoscopic discectomy in L5/S1 intervertebral disc herniation. Eur J Med Res. 2017;22:14..
- [CrossRef] [PubMed] [Google Scholar]




