
Translate this page into:
Calcifying posterior longitudinal ligamentum and posterior osteophytes in case of anterior cervical corpectomy with titanium cage reconstruction
Address for correspondence: Dr. Amit Agrawal, Department of Neurosurgery, Narayana Medical College Hospital, Chinthareddypalem, Nellore - 524 003, Andhra Pradesh, India. E-mail: dramitagrawal@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Agrawal A, Gopalkrishnaiah T. Calcifying posterior longitudinal ligamentum and posterior osteophytes in case of anterior cervical corpectomy with titanium cage reconstruction. J Orthop Allied Sci 2016;4:101-2.
Dear Sir,
Anterior cervical corpectomy with titanium cage reconstruction is one of the effective methods of cervical spine reconstruction.[1,2,3] A 58-year-old male patient who was operated 2 years back for cervical disc disease was apparently doing well. Now, he presented with burning sensation and persistence of paresthesias. There was no history of weakness. There was no history of bowel and bladder disturbances. On examination, the motor and sensory systems were normal. Deep tendon reflexes were normal. Planters were bilateral flexors. His cervical spine X-ray showed titanium cage in-situ with good fusion [Figure 1a]However, there was ossification of the posterior longitudinal ligament with osteophytes. Magnetic resonance imaging of the cervical spine confirmed the ossified longitudinal ligament with mild thecal compression [Figure 1b]. In the absence of features of myelopathy, the patient was planned for conservative management and regular follow-up.
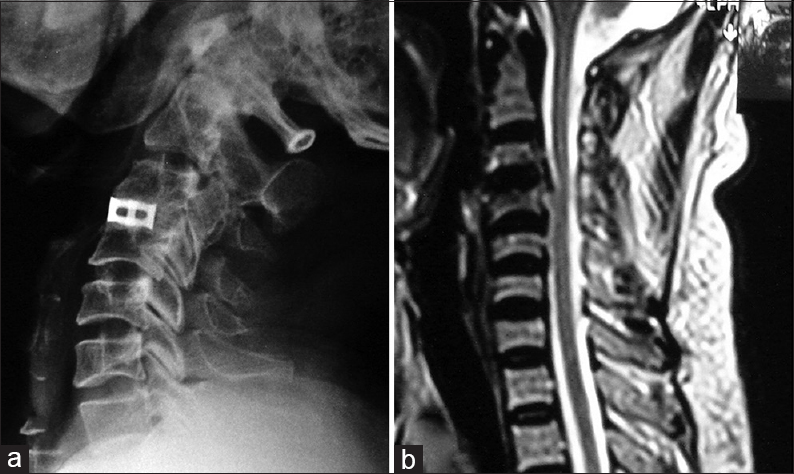
- (a) X-ray of the cervical spine lateral view showing titanium cage in situ with good and solid bony fusion at C3-C4 level, note the posterior osteophytes and ossified ligamentum, (b) Magnetic resonance imaging T2-weighted image showing mild cord compression and calcified ligamentum
The major advantages of titanium cages are immediate stability, restoration of foraminal height and alignment, restoration of anatomic cervical lordosis at the intervertebral segment, and less operative time.[4,5,6] At present, the patient had good fusion as per the criteria described on plain radiograph (segmental movement in the lateral flexion-extension view should stand within 2°, formation of trabecular bone between allograft or cage and adjacent vertebral body and disappearance of the adjacent vertebral body endplate, effacement of bony spur, and remodeling of graft bone).[6,7,8,9,10] Although titanium cage has good outcome, there are few limitations: (1) their high modulus of elasticity contributes to subsidence and kyphotic deformity of the involved segment,[6,10,11,12,13,14,15] (2) cage malplacement,[3] and (3) cage extrusion.[6] Although clinical outcomes of the stand-alone cage have been shown to be encouraging, cage subsidence is a major concern as its complications [Figure 2].[15] If a patient with titanium cage in situ and radiological evidence of good fusion requires a revision surgery, it can be extremely difficult.[16] The cage extraction from a corpectomy site also requires a significant amount of drilling of above and below vertebral bodies.[16] In contrary to the problem of cage subsidence, the present patient had ossified posterior longitudinal ligament and posterior osteophytes (although may not be responsible for his symptomatology). As he did not have deficits related to the involved segments, he was counseled accordingly and managed conservatively.

- X-ray of the cervical spine lateral view of another patient showing titanium cage subsidence
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Anterior cervical reconstruction using titanium mesh cages. J Ayub Med Coll Abbottabad. 2007;19:23-5.
- [Google Scholar]
- Long-term follow-up results in patients with cervical disk disease treated by cervical anterior fusion using titanium cage implants. Neurol Med Chir (Tokyo). 2008;48:440-6.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy and safety of the use of titanium mesh cages and anterior cervical plates for interbody fusion after anterior cervical corpectomy. Surg Neurol. 2006;65:464-71.
- [CrossRef] [PubMed] [Google Scholar]
- Comparing anterior cervical fusion using titanium cage with hydroxyapatite and with autograft. Asian Biomed. 2010;4:147-52.
- [CrossRef] [Google Scholar]
- Subsidence resulting from simulated postoperative neck movements: An in vitro investigation with a new cervical fusion cage. Spine (Phila Pa 1976). 2000;25:2762-70.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior cervical reconstruction using titanium cages with anterior plating. Spine (Phila Pa 1976). 1999;24:1604-10.
- [CrossRef] [PubMed] [Google Scholar]
- The advantages of rectangular titanium cage (RABEA) fusion after anterior cervical discectomy: Comparative study of fibula allograft. J Korean Neurosurg Soc. 2004;36:448-53.
- [Google Scholar]
- A randomized prospective study of an anterior cervical interbody fusion device with a minimum of 2 years of follow-up results. J Neurosurg. 2000;93(2 Suppl):222-6.
- [CrossRef] [PubMed] [Google Scholar]
- A prospective randomized multicenter clinical evaluation of an anterior cervical fusion cage. Spine (Phila Pa 1976). 2000;25:2646-54.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of anterior cervical fusion: Comparison of titanium cages, polyetheretherketone (PEEK) cages and autogenous bone grafts. J Clin Neurosci. 2008;15:1240-5.
- [CrossRef] [PubMed] [Google Scholar]
- The process of subsidence after cervical stabilizations by cage alone, cage with plate and plate-cage. A biomechanical comparative study. Neurol Neurochir Pol. 2007;41:411-6.
- [Google Scholar]
- Anterior cervical discectomy and fusion with implantable titanium cage: Initial impressions, patient outcomes and comparison to fusion with allograft. Spine J. 2004;4:184-91.
- [CrossRef] [PubMed] [Google Scholar]
- Subsidence of the wing titanium cage after anterior cervical interbody fusion: 2-year follow-up study. J Neurosurg Spine. 2006;4:447-53.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior cervical interbody fusion with a titanium box cage: Early radiological assessment of fusion and subsidence. Spine J. 2005;5:645-9.
- [CrossRef] [PubMed] [Google Scholar]
- Cage subsidence does not, but cervical lordosis improvement does affect the long-term results of anterior cervical fusion with stand-alone cage for degenerative cervical disc disease: A retrospective study. Eur Spine J. 2012;21:1374-82.
- [CrossRef] [PubMed] [Google Scholar]
- Application of anterior decompression and reconstruction using titanium mesh with locking plates in the management of cervical spondylotic myelopathy. J Nanjing Med Univ. 2008;22:260-4.
- [CrossRef] [Google Scholar]




