
Translate this page into:
Peringuinal luxation of the femoral head and neck
Address for correspondence: Dr. Andreas Schicho M.D., Department of Orthopaedic Trauma, Ulm University, Albert Einstein Allee 23, D-89081 Ulm, Germany. E-mail: andreas.schicho@uniklinik-ulm.de
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Schicho A, Riepl C. Peringuinal luxation of the femoral head and neck. J Orthop Allied Sci 2016;4:98-100.
Abstract
In high-energy accidents, even exceptional multifragmentary fractures can be found in young and healthy individuals. We hereby report a case of a traumatic proximal femur fracture with dislocation of the femoral head and neck fragment to the scrotum. Although the blood supply to the fragment must have been destroyed during the displacement to the scrotum, there were no radiologic signs of femoral head necrosis. Initial open reduction and internal fixation failed within 7 weeks. The revision with a proximal femur nail was stable. A fast progressing osteoarthritis due to accompanying acetabular fracture urges for a total hip replacement.
Keywords
Femoral fracture
femoral head necrosis
femoral nailing
luxation
open reduction and internal fixation
polytrauma
revision

Introduction
Motorcycle accidents often cause severe injuries including fractures of the pelvis, acetabulum, and femur. Due to the combination of high-energy trauma and typically low protection, even exceptional multifragmentary fractures can be found in young and healthy individuals.[1]
We hereby report a case of a traumatic proximal femur fracture with dislocation of the femoral head and neck fragment to the scrotum, surgical approach and postoperative course with its complications. We hereby report on both the initial findings and the therapeutic pathway with its complications. Informed patient consent for publication was obtained.
Case Report
A 33-year-old man was involved in a motorcycle crash when he lost control at speed 80 kph and struck head-on into an oncoming car. He did not wear protective gear but a helmet. On arrival of the emergency medical service, he was responsive and alert (Glasgow Coma Scale 15). He was intubated for transport and admitted to our level I emergency room. Examination revealed open fractures of the right forearm and hand. The left leg was shortened and rotated outward, the left femur was unstable, and his left scrotum was swollen and hard. His blood pressure was 100/40 mmHg with a heart rate of 105 beats/min.
The polytrauma computed tomography (CT) workup showed an acromioclavicular dislocation Rockwood III (left), fracture of the scapula (right), multifragmentary fracture of the anterior pelvic ring and ventral acetabulum, multifragmentary fracture of the proximal left femur with dislocation of the femoral head and neck to the left scrotum, and a separate greater trochanter fragment [Figure 1a and b]. In addition, radiographs of the right forearm and hand showed fractures of the ulna, metacarpalia III and IV, and fingers 4 and 5.
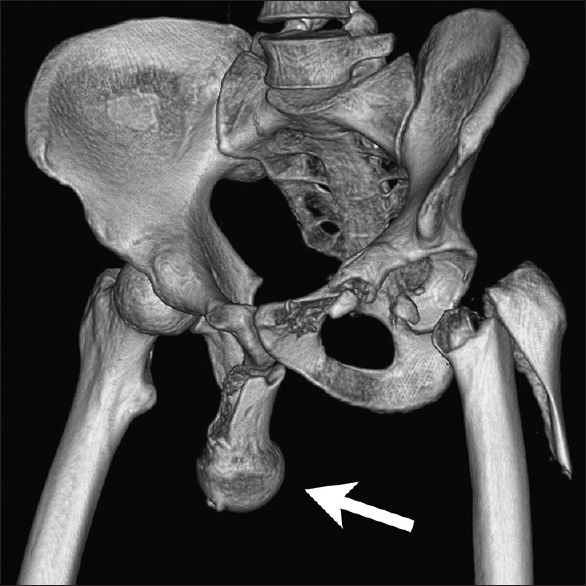
- Dislocation of the femoral head and neck three dimensional-reconstruction of the polytrauma computed tomography scan showed a per inguinal dislocation of the femoral head and neck fragment to the left scrotum (arrow)
The patient was transferred to the operating room. In the supine position, the femoral head was retrieved from the left scrotum by direct incision. The proximal femur was approached from a lateral incision to set fragments by open reduction and internal fixation (ORIF). The trochanter fragment was secured to the femoral stem by tension wires. The femoral head and neck were set back in position, and the fragments were fixed by two 7.3 mm screws. A trochanter stabilizing plate (TSP) was contoured to fit the greater trochanter fragment and mounted over the tension wires and 7.3 mm-screws.
A postoperative X-ray showed anatomic reconstruction with a caput-collum-diaphysis-angle (CCD angle) of 139° on the right and 137° on the left [Figure 2]. The following unweighted mobilization and a femoral torsion angle CT showed a 1 cm loss of leg length on the left. In the 1-month follow-up scan, the CCD angle was decreased to 133°. The patient was dismissed from our hospital after 5 weeks for rehabilitation. With demanded unweighted mobilization for 8 weeks, he returned to our outpatient department for X-ray control on a regular basis. The femoral head and neck were collapsed to a CCD angle of 124° after 7 weeks. Another X-ray and CT control 12 weeks after trauma showed a further depression (CCD angle 122°), signs of bony healing, and no necrosis of the femoral head. With a remaining CCD angle of 112° after 16 weeks [Figure 3], plates and screws had to be removed, and a long proximal femur nail-antirotation (PFN-A, Synthes; 135° angle) was implanted for recovery of the CCD angle [Figure 4]. After 2 weeks of unweighted mobilization, the femoral head and neck fragment was still in place. Sixteen months after trauma, the patient was able to walk freely without any help. A control CT scan showed no signs of femoral head necrosis but fast progress of arthritis and limited bony healing.
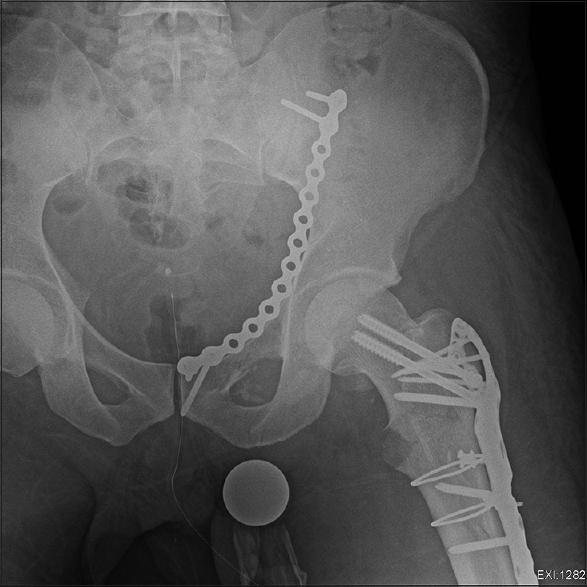
- Control computed tomography showing anatomical reduction caput-collum-diaphysis angle 139° on the right side (not shown), 137° on the reconstructed left side
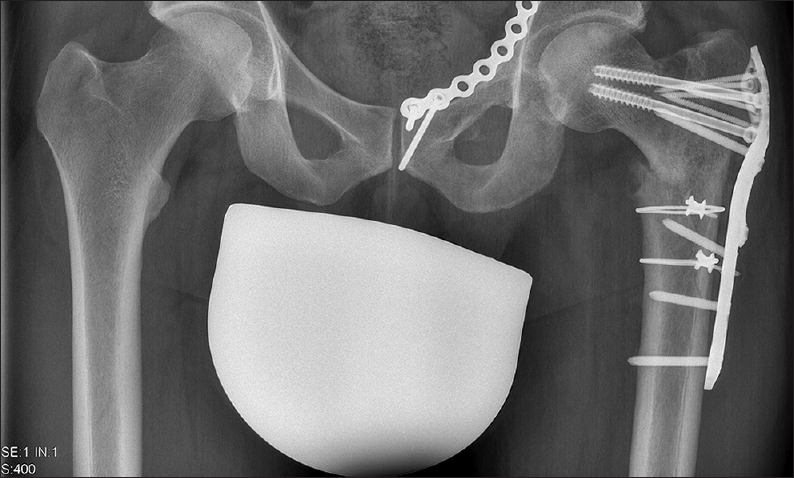
- Follow-up X-ray 4 months after trauma, the caput-collum-diaphysis angle decreased to 112°
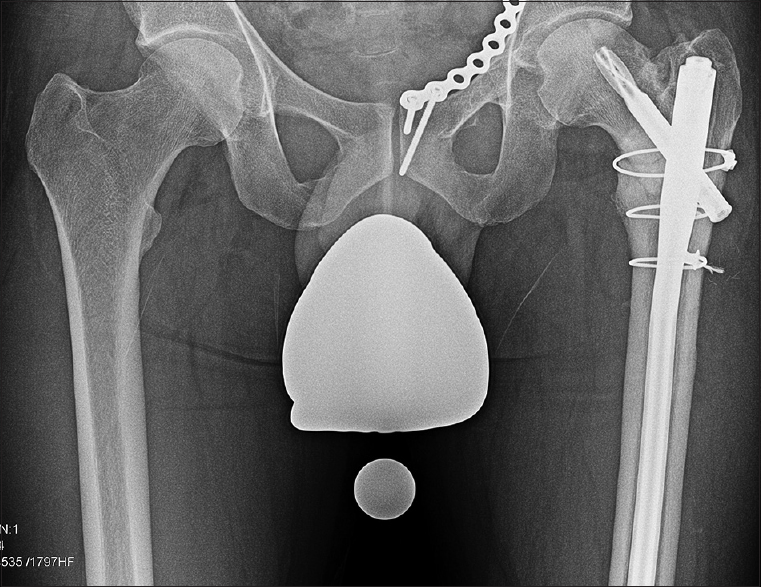
- Control X-ray after revision and change to intramedullary nailing The caput-collum-diaphysis angle was restored using a long proximal femur nail antirotation (Synthes)
Discussion
The main considerations for our therapeutic strategies were the patient's young age, location of the fragments, and fracture morphology.[2] Thus, we chose ORIF with retrieval of the dislocated fragment via direct scrotal incision. The dislocation of the femoral head puts it at high risk for necrosis when the blood supply cannot be restored in time.[3] The combination of tension wires and TSP provided sufficient fixation for both the proximal femur fragment and the greater trochanter fragment. To our surprise, follow-up CT scans showed no signs of necrosis of the head and neck fragment. The depression of the femoral head and neck fragment and loss of CCD angle may be the result of a questionable compliance concerning the advised 8-weeks of unweighted mobilization of the injured leg. To regain anatomical positioning and CCD angle, second surgery and change of fixation technique were necessary.[4] Due to the patient's young age, efforts were focused on preserving the native femoral head via repeat internal fixation using the PFN-A.[5] Firsthand use of the PFN-A might have prevented the CCD collapse, but was no option due to the greater trochanter fragment.
To our understanding, the dislocation of the fragment to the scrotum was result of a direct high-energy blow to the left hip. In all probability, the fragment was pushed along the inguinal canal to the scrotum, possibly facilitated by the distorted anatomical properties of the anterior pelvic ring.[6] Although the blood supply to the fragment must have been destroyed during the displacement to the scrotum, there were no radiologic signs of femoral head necrosis, and the PFN-A blade was implanted into bone mass of seemingly good quality. As there was metal implanted at all times, no magnetic resonance imaging was used for definitive, high sensitive detection of femoral head necrosis. An urological follow-up examination showed no damage to the left testicle, although it is known that compression of the testicles can lead to ischemia.[7]
Multifragmentary proximal fractures of the femur are quite common injuries, especially in the elderly,[8] or in high-energy injuries such as motorcycle accidents[1] in the younger population. Peringuinal luxation of the femoral head and neck fragment to the scrotum is a rare event. Despite the fact that the femoral head showed no signs of necrosis, a total hip replacement will be necessary anyway due to the fast progressing osteoarthritis. Histologic workup of the femoral head will then shed light onto the question of necrosis, whether and to what extent.
Pictures of the initial finding were published elsewhere before.[9]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Surgical treatment for ipsilateral fractures of the hip and femoral shaft. Injury. 2004;35:165-9.
- [CrossRef] [PubMed] [Google Scholar]
- Plating of femoral neck fractures: When and how? J Orthop Trauma. 2015;29(Suppl 4):S1-3.
- [CrossRef] [PubMed] [Google Scholar]
- PET/CT study of temporal variations in blood flow to the femoral head following low-energy fracture of the femoral neck. Orthopedics. 2014;37:e563-70.
- [CrossRef] [PubMed] [Google Scholar]
- When femoral fracture fixation fails: Salvage options. Bone Joint J. 2013;95-B(11 Suppl A):7-10.
- [CrossRef] [PubMed] [Google Scholar]
- Is helical blade nailing superior to locked minimally invasive plating in unstable pertrochanteric fractures? Clin Orthop Relat Res. 2012;470:2302-12.
- [CrossRef] [PubMed] [Google Scholar]
- The role of pelvic bone anatomy in the pathogenesis of inguinal hernia. Chirurgia (Bucur). 2014;109:783-7.
- [Google Scholar]
- Testicle ischemia resulting from an inguinal hernia. J Emerg Med. 2012;43:e299-301.
- [CrossRef] [PubMed] [Google Scholar]
- Hip fracture prediction in elderly men and women: Validation in the Rotterdam study. J Bone Miner Res. 1998;13:1587-93.
- [CrossRef] [PubMed] [Google Scholar]
- Femoral-head dislocation to the scrotum. New Engl J Med. 2015;372(9):863.
- [CrossRef] [PubMed] [Google Scholar]




