
Translate this page into:
Carpal tunnel syndrome: Ultrasonographic evaluation of median nerve diameter
Address for correspondence: Dr. Babul Reddy, Department of Orthopaedics, Kasturba Medical College, Mangalore, Karnataka, India. E-mail: babulortho@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kamath JB, Reddy B, Sivam U, Venugopal A, Jayasheelan N. Carpal tunnel syndrome: Ultrasonographic evaluation of median nerve diameter. J Orthop Allied Sci 2016;4:14-7.
Abstract
Background:
Carpal tunnel syndrome is the most frequently encountered peripheral compression neuropathy. Diagnosis of carpal tunnel syndrome involves physical examination, nerve conduction studies and electromyography. Ultrasonography (USG) examination of median nerve in carpal tunnel has been proposed as a useful alternative in diagnosing carpal tunnel syndrome.
Materials and Methods:
Patients were selected from those undergoing diagnostic workup for carpal tunnel syndrome in pre-treatment period. USG was performed using 11 MHz linear array transducer. Cross-sectional area at each level, major and minor axes were measured.
Results:
In our study, the mean median nerve cross sectional area at proximal part of carpal tunnel by direct method was 12.33 mm2 in patients and 7.33 mm2 in controls. By indirect method it was 12.01 mm2 and 6.633 mm2 in cases and controls respectively. In this study we found significant difference in flattening ratio between cases and controls. The mean flattening ratio in distal part of tunnel (at the level of hook of hamate) was 2.97 and 2.38 in cases and controls respectively. The sensitivity and specificity for cut-off value ≥2.5 was 76% and 63% respectively.
Conclusion:
We found that best discriminatory criterion for diagnosis of carpal tunnel syndrome are median nerve cross sectional area in the proximal part of carpal tunnel ≥9 mm2 (Direct method) and ≥8.5 mm2 (Indirect method). With our experience, we found it easier to evaluate the median nerve in the carpal tunnel in the disto proximal sequence by identifying the flexor pollicislongus (FPL) first with dynamic evaluation. As the percentage of space occupying lesions causing symptoms in unilateral (atypical) carpal tunnel syndrome is 35%, we highly recommend this pre-operative investigation in all carpal tunnel syndrome patients.
Keywords
Carpal tunnel syndrome
flexor pollicislongus
median nerve
ultrasonogram

Introduction
Carpal tunnel syndrome is the most frequently encountered peripheral compression neuropathy. Typical patients are the late middle aged women. In spite of many associated illness a clear mechanism of how carpal tunnel syndrome develops has yet to be elucidated. Diagnosis of carpal tunnel syndrome involves physical examination, nerve conduction studies and electromyography. The nerve conduction studies reflect the status of nerve fibre. Although they are integral to the evaluation and diagnosis of carpal tunnel syndrome they have inherent disadvantages that limit their accuracy.[1] In the diseased nerve, if there are nerve fibres unaffected by disease, the results may appear normal. Ultrasonography (USG) examination of median nerve in carpal tunnel syndrome has been proposed as a useful alternative in diagnosing carpal tunnel syndrome. In most studies, it is accepted that an increase in cross sectional area measurement of the median nerve is a significant criteria in the diagnosis of carpal tunnel syndrome.[2] Magnetic resonance imaging (MRI) has been shown to of value in diagnosis of carpal tunnel syndrome. However the advantages of USG are lower cost, shorter examination time and easy availability.
Materials and Methods
Patients were selected from those undergoing diagnostic workup for carpal tunnel syndrome in pre-treatment period. Patients were diagnosed to have carpal tunnel syndrome based on clinical findings independent of nerve conduction velocity results. This is a prospective study conducted from august 2004 to September 2006. The exclusion criteria includes: (1) patients with fracture of carpal bones or carpo-metacarpal dislocations; (2) due to edema resulting from extensive hand injuries; (3) old fractures around the wrist and (4) patients who underwent surgery around the wrist in the past.
Thirty patients (6 male, 24 female and age range 22-78 yrs) were included in the study. Total 46 wrists were studied of which 16 patients had bilateral whereas 14 patients had unilateral carpal tunnel syndrome. Forty six wrists of healthy participants (6 male 24 female, age range 23-80 yrs) without any symptoms of carpal tunnel syndrome or related illness formed the control. Electrophysiological studies were performed in all patients. Carpal tunnel syndrome was diagnosed if there was distal motor latency >4.5 ms, and distal sensory latency >3.5 ms, asymmetry of conduction between both hands of more than 1 ms for motor conduction or 0.5 ms for sensory conduction.
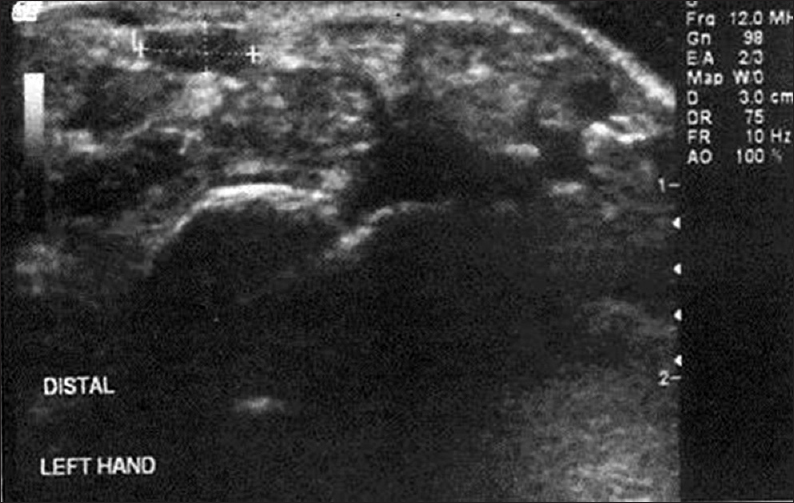
USG was performed using 11MHz linear array transducer. Transverse USG was performed at two levels: (1) At the level of pisiform (proximal part of carpal tunnel) and (2) at the level of hook of hamate (distal part of carpal tunnel). The USG was performed from distal to proximal. The Flexor pollicislongus (FPL) tendon is identified at the level of hook of hamate by asking the patient to actively move the inter phalangeal joint of the thumb. The structure just ulnar to the FPL at that level almost the same size as that of FPL tendon is the median nerve. Once the median nerve is identified, it is traced proximally by ultrasonography evaluation at the proximal border of the carpal tunnel at the level of pisiform. The transducer was always kept perpendicular to median nerve and any compression that could cause nerve deformation was avoided. Cross-sectional area at each level, major and minor axes were measured. Cross-sectional area was also calculated by making continuous boundary trace within the echogenic rim indicating epineurium of median nerve [direct method, Figure 1].

- USG of proximal part of carpal tunnel showing measurement of cross-sectional area by direct method
Cross sectional area was calculated using the formula n/4 (D1 × D2) [indirect method, Figure 2].
- USG in the distal part of carpal tunnel showing indirect method of measuring cross-sectional area
The flattening ratio was calculated at the distal part of carpal tunnel by dividing major axis by minor axis.
Results
Median nerve measurement in patients and controls were compared an accuracy of this diagnostic technique was calculated. The arithmetic mean and the range in each group were determined. The differences between the methods were compared using paired t rest. Sensitivity, specificity, positive predictive value in carpal tunnel syndrome patients was obtained by determining the cut-off point using receiver-operating characteristic (ROC) curve. SPSS was used in all statistical analysis.
Majority of patients in the study were in 41-50 years of age. The mean age of patients in the study was 47 yrs. The mean age for male was 45 yrs. The mean age for female was 48 yrs. There were 24 females (80%) and six male patients (20%) in the study. Sixteen patients had bilateral carpal tunnel syndrome. Eleven patients had right side involvement and three had left side involvement. Majority of patients had symptoms of less than 6 months duration. Most common symptom was pain in the hand followed by numbness in lateral 3 1/2 fingers. Majority of the patients in the study underwent surgical treatment (30 cases). Sixteen cases had symptomatic improvement with intermittent use of wrist splints.
Analysis
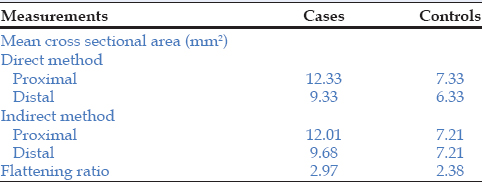
The measured values in carpal tunnel syndrome patients and in controls are summarized in Table 1. The 't' test was used to compare the groups. Following were the results of analysis: (1) The was significant difference in the mean cross sectional areas of median nerve in proximal part of carpal tunnel (both direct and indirect method) between cases and controls; (2) there was significant difference in flattening ratio between cases and controls; (3) there was no significant difference between values obtained by direct and indirect method in both cases and controls and 4) no significant difference in cross sectional areas of median nerve was found between right and left wrists. Critical diagnostic values of the test were listed in Table 2.
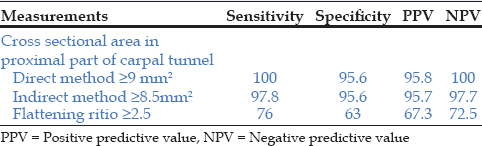
The cut off points for sensitivity and specificity using ROC analysis was 9 mm2 for cross sectional areas by direct method and 8.5 mm2 by indirect method in proximal part of carpal tunnel. We found that flattening ratios is highly variable and less predictive.
ROC curve comparing cross-sectional area by direct and indirect method in proximal part of carpal tunnel shows 0.9997 and 0.996 respectively, indicating that one test is not better than the other.
Discussion
Nerve conduction study and imaging techniques are used to support the diagnosis of carpal tunnel syndrome and revealing the underlying pathology. Each method has its advantages and disadvantages. There is still controversy about real value of nerve conduction study for diagnosis of carpal tunnel syndrome.[1,3,4,5] Many researchers now believe that diagnosis must be based on clinical findings.[4,6,7] MRI and USG are painless diagnostic techniques. By imaging the carpal tunnel anatomy, they can also discriminate pathological changes such as synovitis, tumours and anatomical malformations from idiopathic causes. Nakamichi described 35% of patients with unilateral carpal tunnel syndrome was associated with space occupying lesions.[8] In our study we had one patient with carpal tunnel syndrome showing marked synovial thickening around the flexor tendons [Figure 3]. The space occupying lesions as an etiological factor for carpal tunnel syndrome is not uncommon. Importance of knowing these secondary causes of carpal tunnel syndrome preoperatively cannot be over emphasized as it may dictate the timing of surgery, choice of anesthesia, need for admission, histopathological analysis and finally prognosis. MRI provides an excellent tissue contrast and a clear presentation of soft tissue abnormalities. The principal advantages of ultrasonography are its low cost, short study time, availability and possibility of dynamic imaging. Despite these advantages operator dependency and absence of standardized parameters prevents the wide spread use of USG in carpal tunnel syndrome.
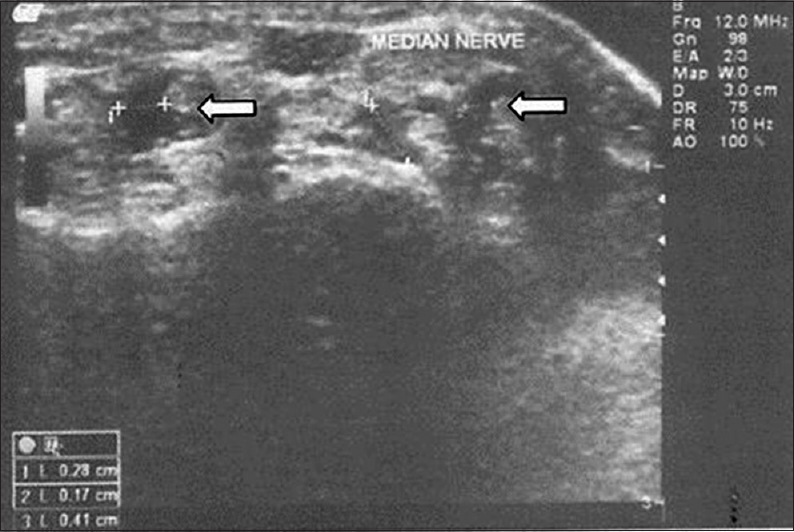
- USG in a 52 years old female with carpal tunnel syndrome showing marked synovial thickening around the flexor tendons
There has been increased interest in the use of USG for evaluation of carpal tunnel syndrome since the development of small high frequency transducers. As USG evaluation of carpal tunnel syndrome has not standardized, different measuring techniques have been used.[1,9,10,11,12] The cut-off values are higher in studies that used nerve conduction study as gold standard than those relied on clinical diagnosis.
In the present study, the mean median nerve cross sectional area at proximal part of carpal tunnel by direct method was 12.33 mm2 in patients and 7.33 mm2 in controls. By indirect method it was 12.01 mm2 and 6.633 mm2 in cases and controls respectively. Buchberger et al., found that the mean cross sectional area was 14.5 mm2 in cases and 7 mm2 in control groups. In Duncan et al., study the mean cross sectional area was 12.7 mm2 and 7 mm2 in cases and controls respectively.[10] Nakamichi et al., found that the mean cross sectional area was 16.8 mm2 in cases and 10.02 mm2 in controls.[13] The cause of this variability may be difference in the study design or measurement techniques.
We measured the cross sectional area of median nerve at the level of pisiform. In some studies cross sectional area was measured in proximal, middle and distal level of carpal tunnel.[11,13] However, these studies report that increase in cross sectional area is maximum in proximal part of carpal tunnel. Nakamichi et al., observed "hour glass" configuration of median nerve (cross-sectional area is lower at the level of hamate than at the proximal and distal part of tunnel) both in patients and in controls.[13] We obtained the measurements of the median nerve from the inner border of echogenic epineurium surrounding hypo echoic median nerve. Because of the echogenic epineural fat, the exact border may not be clearly distinguishable and differences can be seen in measurements obtained at the inner and outer border of epineurium. In some studies the border used in the measurement was not reported; this may be one of the causes of different results.
Duncan et al., reported the direct method of measuring cross sectional area to have higher diagnostic accuracy as compared to indirect method.[10] However we did not find any significant difference between direct and indirect methods. In this study we found significant difference in flattening ratio between cases and controls. The mean flattening ratio in distal part of tunnel (at the level of hook of hamate) was 2.97 and 2.38 in cases and controls respectively. The sensitivity and specificity was ≥2.5 was used as cut-off values was 76% and 63% respectively.
Lee et al., recommended USG as the initial test in the evaluation of carpal tunnel syndrome.[6] Many authors have proposed USG a better diagnostic test compared to nerve conduction studies.[1,9,10,12,13,14] We found that best discriminatory criterion for USG diagnosis of carpal tunnel syndrome are median nerve cross sectional area in the proximal part of carpal tunnel ≥9 mm2 (Direct method) and ≥8.5 mm2 (Indirect method). However the present study has some limitations, the use of single USG and lack of repeated measurements.
Conclusion
USG is a simple technique to evaluate the median nerve and contents of carpal tunnel. The anatomy of median nerve can be clearly defined and accurate measurements of its dimensions can be obtained. The abnormalities of median nerve, including edema, contour abnormalities and cross sectional area can be determined by USG. With our experience we found it easier to evaluate the medial nerve in the carpal tunnel in the disto-proximal sequence by identifying the FPL first with dynamic evaluation. As the percentage of space occupying lesions causing symptoms in unilateral (atypical) carpal tunnel syndrome is 35%, we highly recommend this preoperative investigation in all unilateral carpal tunnel syndrome patients. High frequency USG has emerged as a reliable modality in carpal tunnel syndrome, more so because it's non-invasive and accurate.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Ultra sonographic assessment of mild and moderate idiopathic carpal tunnel syndrome. Clin Radiol. 2004;59:916-25.
- [CrossRef] [PubMed] [Google Scholar]
- The value of history in the diagnosis of carpal tunnel syndrome. J Hand Surg Br. 2000;25:445-50.
- [CrossRef] [Google Scholar]
- The utility of portal nerve conduction testing for patients with carpal tunnel syndrome: A prospective clinical study. J Hand Surg Am. 1992;17:77-81.
- [CrossRef] [PubMed] [Google Scholar]
- Value of electro diagnostic tests in carpal tunnel syndrome. J Hand Surg Br. 2000;25:361-5.
- [CrossRef] [PubMed] [Google Scholar]
- Carpal tunnel syndrome with normal nerve conduction studies. Muscle Nerve. 2004;29:515-22.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis of carpal tunnel syndrome. Radiol Clin North Am. 1999;37:859-72.
- [CrossRef] [PubMed] [Google Scholar]
- Unilateral carpal tunnel syndrome and space-occupying lesions. J Hand Surg Br. 1993;18:748-9.
- [CrossRef] [Google Scholar]
- Ultrasonography versus nerve conduction study in patients with carpal tunnel syndrome: Substantive or complementary tests? Rheumatology (Oxford). 2004;43:887-95.
- [CrossRef] [PubMed] [Google Scholar]
- Sonography in the diagnosis of carpal tunnel syndrome. AJR Am J Roentgenol. 1999;173:681-4.
- [CrossRef] [PubMed] [Google Scholar]
- Carpal tunnel syndrome: Diagnosis with high resolution sonography. AJR Am J Roentgenol. 1992;159:793-8.
- [CrossRef] [PubMed] [Google Scholar]
- The role of ultra sonography measurements of the median nerve in the diagnosis of carpal tunnel syndrome. Clin Radiol. 2004;59:910-5.
- [CrossRef] [PubMed] [Google Scholar]
- Enlarged median nerve in idiopathic carpal tunnel syndrome. Muscle Nerve. 2000;23:1713-8.
- [CrossRef] [Google Scholar]
- Dynamic high resolution sonography of the carpal tunnel. AJR Am J Roentgenol. 1997;168:533-7.
- [CrossRef] [PubMed] [Google Scholar]




