
Translate this page into:
Primary intraosseus meningioma of the calvarium presenting as solitary osteolytic lesion
Address for correspondence: Dr. Kanika Mehta, 512 A, Model Town, Yamuna Nagar - 135 001, Haryana, India. E-mail: kanika.mehta87@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Mehta K, Mohan V, Munshi A, Sehrawat R. Primary intraosseus meningioma of the calvarium presenting as solitary osteolytic lesion. J Orthop Allied Sci 2015;3:72-5.
Abstract
A rare case of primary intraosseous meningioma of the calvarial bones presenting as solitary osteolytic lesion on the skull radiograph and correctly diagnosed pre-operatively on computed tomography (CT) and magnetic resonance imaging (MRI) by correlating the clinical and imaging findings is reported in this communication. The clinical, radiographic, CT and MR imaging features of the case and the difficulties in making a correct clinico –radiological diagnosis are highlighted in this communication.
Keywords
Intradiploic meningioma
primary intraosseous meningioma
solitary osteolytic lesion of the calvarium

Introduction
Meningiomas are the most common benign intracranial neoplasms. Nearly 20% of all primary intracranial tumors are meningiomas. Primary intraosseous meningiomas are a subtype of the meningiomas that represents the most uncommon manifestation of meningiomas.[1] Reportedly, these neoplasms occur in the calvaria, scalp, orbit, paranasal sinuses, oropharynx, nasopharynx, neck, skin.[2] Intradiploic location of the meningioma is extremely rare.[3] According to El –Narsh (2009), a pre operative diagnosis of intradiploic meningioma is very difficult and usually these tumors are mistaken for many conitions including infections of calvarial bones;- Langerhans cell histiocytosis; and even primary benign, malignant and metastatic tumors of skull bones.[4]
Case Report
A 35 year old healthy young female presented with the chief complaints of a swelling on the scalp in the left frontoparietal region since more than 2 years.
There was no history of local trauma and local scalp infection. The swelling grew to the present size very slowly over the period and was not associated with any pain or discomfort. General physical examination of the patient was unremarkable.
All the lab investigations were reported normal. Local examination revealed a bony hard swelling on the left fronto parietal region. The skin over it appeared free. Local temperature over the swelling was not raised.
With the clinical diagnosis of an osteoma/osteochondroma, the patient had X-rays of the skull at another hospital which revealed a well defined lobulated osteolytic lesion with sclerosis of its margins [Figure 1]. The radiological differential diagnosis included dermoid/epidermoid, Langerhans cell histiocytosis, myeloma and metastatic malignancy. However, the radiographic and clinical findings were not suggestive of any of the above entities and hence computed tomography (C-T) head was performed which revealed an intradiploic mass lesion causing smooth expansion of both outer and inner tables of the skull [Figure 2].

- Lateral Xray skull showing a well defined lytic lesion, lobulated in appearance with sclerotic margins
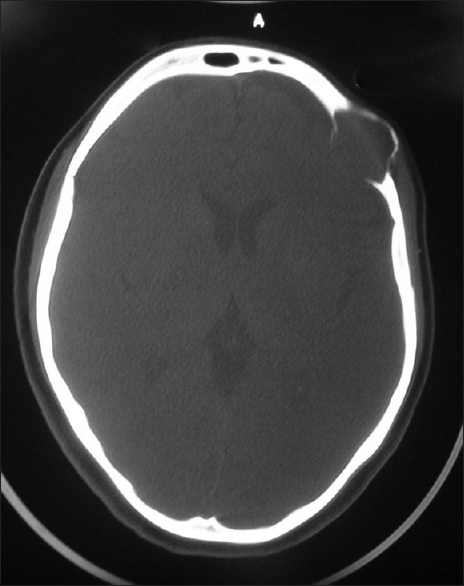
- NCCT Brain reveals an expansile lytic lesion involving both the inner and outer tables of the left frontal bone with thinning of inner and outer tables
The type of expansion and duration of illness were suggestive of it being a benign lesion and hence the possibility of giant cell tumor (G-C-T) of skull bone was made.
For further evaluation, magnetic resonance imaging (MRI) brain was performed which revealed a well defined soft tissue intradiploic mass which was isointense to brain on both T1- weighted (T1W) and T2W sequences.
[Figures 3 and 4], and revealed intense uniform enhancement on post gadolinium images [Figure 5] highly suggestive of intradiploic/intraosseous meningioma with resultant bony changes in the calvarial bones, mimicking calvarial bone pathology. Complete resection of the tumor was undertaken and the patient had an uneventful recovery.
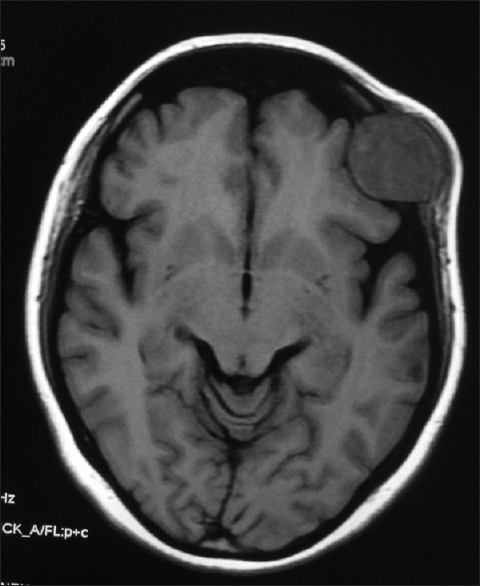
- MR images reveals a well defined extra axial mass lesion in the left frontal region, isointense onT1WI
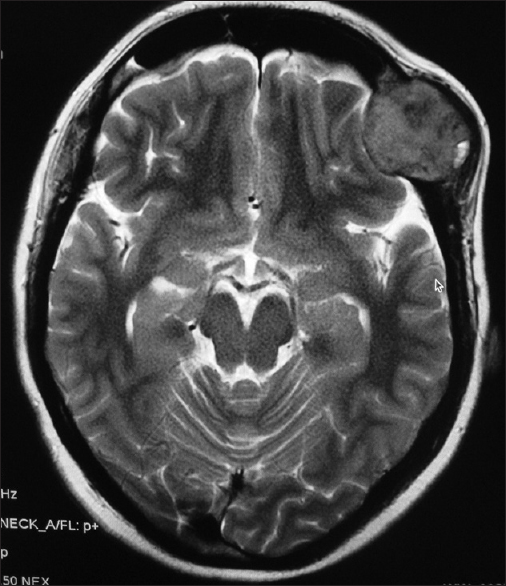
- MR images reveals a well defined extra axial mass lesion in the left frontal region, isointense on T2WI

- Post contrast MR images show intense homogenous contrast enhancement with a dural tail
Histopathological examination of the specimen confirmed the MR diagnosis. She is being regularly followed-up and is completely asymptomatic.
Discussion
When a radiologist is confronted with skull radiograph of an adult showing a well defined osteolytic lesion, the list of differential diagnosis is quite long and include entities like dermoid, epidermoid, eosinophillic granuloma, osteomyelitis, aneurysmal bone cyst(ABC), GCT, brown tumor of hyperparathyroidism, myeloma and metastatic malignancy.
Depending upon the age of the patient, duration of the complaints, local clinical and X-ray findings in rest of the calvarial bones and in the mandible, the differential diagnosis can be narrowed down to few conditions. However in the above scenario it is extremely unusual to think of the possibility of the lesion being caused by an intraosseous meningioma, unless one had diagnosed such a case earlier or come across a case report while scanning the medical literature.
Extracranial meningiomas are very rare; the reported incidence is 1–2% of all meningiomas. The meningiomas arising in locations outside the dural compartment have been called ectopic, extradural (epidural), calvarial, cutaneous, extracranial, extraneuraxial, or intraosseous meningiomas.[5] Winkler, in 1904, first described a meningioma originating in an extradural location.[6]
'Primary intraosseous meningioma' is a subset of extradural meningiomas that arise in bone.
They have been said to arise from arachnoid cell rests caught within extradural tissue during embryologic development or extruded following skull fractures after trauma. The tumors are usually observed near or at the suture lines (most commonly at the coronal oterion suture) or at previous fracture sites.[7] True primary intraosseous meningiomas do not involve the underlying dura. Extradural meningiomas that arise from the skull have been named as calvarial, intradiploic, and intraosseous.[1] To avoid confusion, [Lang et al. (2000)] classified intraosseous meningiomas as purely extracalvarial (type I), purely calvarial (type II), or calvarial with extracalvarial extension. Many different hypotheses exist regarding the origin of primary extradural and calvarial meningioma. They are thought to arise from ectopic meningiocytes or arachnoid cap cells trapped in the cranial sutures during molding of head at birth.[8] The real incidence of primary intraosseous meningioma is unknown.[1] According to the scanned literature, 68% of the primary extradural meningiomas involve the calvaria.
Common locations for convexity intraosseous meningiomas are frontoparietal and orbital regions.[4] They are reported to occur with the same frequency in both sexes with slight female predominance. They occur predominantly during later decades of life, and also have a second peak incidence in younger patients (especially during the second decade).[5]
As in our case, patients with calvarial intraosseous meningiomas typically present with slow-growing scalp swelling that may or may not be painful. They do not show any neurologic symptoms or signs, unless the lesion extends through the inner table and compresses intracranial structures. These lesions may be asymptomatic and are detected incidentally.[9]
Biologically, calvarial meningiomas have been observed to be benign and slow-growing. On the other hand, calvarial meningiomas are more prone to develop malignant changes (11%) compared with intracranial meningiomas (2%).[5]
Calvarial meningiomas presenting with scalp swelling, osteolytic skull lesions, and extracranial soft-tissue masses are more aggressive in nature than others. Younis and Sawaya (1992) reported three patients who presented with scalp swellings, osteolytic skull lesions, and extracranial soft-tissue masses. All of their patients had malignant meningiomas. On the basis of their experience, they contended that osteolysis, when associated with a soft-tissue mass, is a strong reason to suspect a malignant meningioma.[10] Hussaini (1970) also reported a case with lytic lesion in the frontal region that was diagnosed as malignant meningioma histologically.[11]
Radiographic findings of extradural meningiomas are limited and not pathognomic because of the superimposed bony structures. These tumors are either typically osteoblastic, osteolytic or of mixed variety. Majority of intraosseous meningiomas are osteoblastic and hence produce hyperosteosis.[1] The tumors presenting with osteolytic lesions and a soft tissue component in the present case are extremely rare and hence difficult to diagnose before biopsy. Only 16 such cases have been reported earlier.[12]
On CT osteolytic lesions typically cause thinning, expansion, and interruption of outer and inner tables as in our case. The lesions are iso – hyperdense compared with brain parenchyma and show homogenous enhancement after contrast administration. On MRI these lesions appear like intracranial meningiomas which are iso – hypodense on T1W and show variable appearance(mostly hyperdense) on T2W images. Intense homogeneous enhancement after gadolinium administration is typical as noted in our case and the above MR findings are almost diagnostic.[4] The treatment of the meningiomas is always surgical removal.[9]
Histopathologically, these lesions may range from epithelial to mesenchymal in appearance like their intracranial counterparts.[1]
It is recommended that intraosseous meningioma may be included in the differential diagnosis of an osteolytic lesion found on (the skull radiograph when a young patient presents clinically with a slowly growing, painless, hard swelling over the scalp).
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Intradiploic meningioma mimicking calvarial metastasis: Case report. Turkish Neurosurg. 2009;19:297..
- [Google Scholar]
- Two cases of Primary osteolytic intraosseous meningioma of the skull metastasing to whole skull and the spine; Korean Neurosurg Soc. 2012;51:151.
- [CrossRef] [PubMed]
- Intradiploic meningioma (Study of 7 cases and review of literature) Eur J Neuro Surg. 2009;24:13-23.
- [Google Scholar]
- Primary intraosseous meningioma; CT and MRI appearance. AJNR Am J Neuroradiol. 2005;26:2053-6.
- [Google Scholar]
- Intradiploic meningioma of the orbit: A case report Neurol India. 2004;52:380-2.
- Primary intraosseous meningiomas of the skull. Clin Radiol. 1997;52:546-9.
- [CrossRef] [PubMed] [Google Scholar]
- Intracranial osteolytic malignant meningiomas appearing as extracranial soft-tissue masses. Neurosurgery. 1992;30:932-5.
- [CrossRef] [PubMed] [Google Scholar]
- Osteolytic intra-osseous meningiomas: Illustrated review. Acta Neurochir (Wien). 2004;146:1245-9.
- [CrossRef] [PubMed] [Google Scholar]




